
ABSTRACT
Cell-based therapeutic cancer vaccines use autologous patient-derived tumor cells, allogeneic cancer cell lines or autologous antigen presenting cells to mimic the natural immune process and stimulate an adaptive immune response against tumor antigens. The primary objective of this study is to perform a systematic literature review with an embedded meta-analysis of all published Phase 2 and 3 clinical trials of cell-based cancer vaccines in human subjects. The secondary objective of this study is to review trials demonstrating biological activity of cell-based cancer vaccines that could uncover additional hypotheses, which could be used in the design of future studies. We performed the systematic review and meta-analysis according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The final review included 36 studies − 16 single-arm studies, and 20 controlled trials. Our systematic review of the existing literature revealed largely negative trials and our meta-analysis did not show evidence of clinical benefit from cell-based cancer-vaccines. However, as we looked beyond the stringent inclusion criteria of our systematic review, we identified significant examples of biological activity of cell-based cancer vaccines that are worth highlighting. In conclusion, the existing literature on cell-based cancer vaccines is highly variable in terms of cancer type, vaccine therapies and the clinical setting with no overall statistically significant clinical benefit, but there are individual successes that represent the promise of this approach. As cell-based vaccine technology continues to evolve, future studies can perhaps fulfill the potential that this exciting field of anti-cancer therapy holds.
Introduction
The anti-cancer clinical responses seen with immune checkpoint inhibitors (ICIs) and chimeric antigen receptor (CAR)-T cell therapy have firmly established the potential of the immune system to control, or even eradicate cancer. Their success, however, has been restricted to a subset of patients. ICIs rely largely on the presence of preexisting tumor infiltrating cytotoxic T lymphocytes to produce anti-tumor effect, and these are absent in a significant proportion of patients.Citation1,Citation2 Therapeutic cancer vaccination is an active immunization strategy, which aims to stimulate an adaptive immune response against tumor antigens and generate tumor-specific functional immune effectors, including cytotoxic T lymphocytes.
Therapeutic cancer vaccines have been researched for decades, and different approaches have been used to develop vaccine constructs for anti-cancer therapy. Broadly, these can be classified as cell-based vaccines, viral vector vaccines and molecular vaccines consisting of either peptides, deoxyribonucleic acid (DNA) or ribonucleic acid (RNA).Citation3 Cell-based cancer vaccines use either replication incompetent cancer cells (autologous patient-derived tumor cells or allogeneic cancer cell lines) or autologous antigen presenting cells (APCs) loaded with cancer antigens. Tumor cell-based vaccines have the advantage of involving a broad range of neoantigens, eliminating the need to prospectively identify target antigens, though effective antigen presentation can be a limiting factor.Citation4 Dendritic cells (DCs) are professional APCs optimal for priming of T cell responses and DC-based therapeutic cancer vaccines have been extensively studied.Citation5 Sipuleucel-T (Provenge ®), a vaccine consisting of ex vivo activated peripheral blood mononuclear cells, including DCs, became the first FDA approved therapeutic cancer vaccine after the phase 3 IMPACT trial showed improved overall survival in patients with metastatic castration-resistant prostate cancer.Citation6
The increasing role of ICIs in multiple cancers has led to renewed interest in personalized cancer vaccines as a means to induce or augment the anti-tumor immune response.Citation7 Importantly, since cancer vaccines and ICIs target different stages of the cancer immune cycle, vaccine-ICI combinations have the potential to synergistically overcome each individual therapy’s resistance mechanisms.Citation8 The cell-based cancer vaccines are backed by a strong biological rationale since they mimic the natural immune process.Citation9 They have had encouraging pre-clinical results, and trials of cell-based cancer vaccines have demonstrated their ability to mount tumor-specific T-cell responses, but are yet to realize their full potential in terms of durable clinical benefit.Citation3 There is little consensus on their role, which cancer types are likely to benefit and which vaccine approach provides maximum efficacy. The current evidence is inconclusive due to limited number of studies, with relatively smaller sample sizes. This provides the rationale for undertaking this systematic review and meta-analysis, with an attempt to combine existing evidence and analyze the overall effect of cellular cancer vaccines. Hence, we sought to assess the clinical utility of cellular cancer vaccines, as measured by Response Evaluation Criteria in Solid Tumors (RECIST) response or survival benefit, by systematically reviewing and comprehensively summarizing available data on cell-based cancer vaccines from published clinical studies. The primary objective of this study is to perform a systematic literature review with an embedded meta-analysis of all published Phase 2 and 3 clinical trials of cell-based cancer vaccines in human subjects. The secondary objective of this study is to review trials demonstrating biological activity of cell-based cancer vaccines that could uncover additional hypotheses, which could be used in the design of future studies. Therefore, a more granular review of individual studies independent of the meta-analysis was done, focused on detecting biological activity as opposed to RECIST responses, as defined below.
Materials and methods
The systematic review and meta-analysis were performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.Citation10
Types of studies
In the systematic review, we included all published Phase 2 and 3 clinical trials of cell-based cancer vaccines in human subjects. We considered cell-based cancer vaccines to include autologous tumor cell, allogeneic tumor cell and dendritic cell vaccines. We included both single arm and multiple arm/controlled studies. Single-arm studies were included if they reported objective responses using RECIST. Multiple arm studies were included if they reported hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for the association between cancer vaccines and overall survival (OS). The studies were characterized based on the clinical setting being evaluated (adjuvant vs metastatic vs recurrent) and the controlled studies were also classified based on the duration of follow-up being reported (<5-year vs ≥5 year). We excluded studies in which patients were treated simultaneously with chemotherapy, immunotherapy, and/or radiation therapy along with a cell-based cancer vaccine.
Types of outcome measures
All included single-arm studies utilized the RECIST guidelines, and the meta-analyzed outcome measures reported were Complete Response (CR), Partial Response (PR), Stable Disease (SD), Progressive Disease (PD) and Disease Control Rate (DCR; [DCR=CR+PR+SD]). For multiple arm studies, the meta-analyzed outcome measure was Overall survival (OS), reported as pooled hazard ratios (HRs) with 95% confidence interval. This was reported separately for studies in the adjuvant setting, metastatic setting and with ≥5-year survival follow-up.
Search strategy
A database search was performed using the PubMed database and ClinicalTrials.gov to identify published results of all Phase 2 and 3 clinical trials of cell-based cancer vaccines from January 1, 1985, to December 31, 2021. The https://pubmed.ncbi.nlm.nih.gov/search terms were “cancer vaccine” (limited to clinical trials between 1985 and 2021). The ClinicalTrials.gov search terms were Condition or disease = “Cancer,” Search Term = “Vaccine,” Study Type = “Interventional Studies (Clinical Trials),” Study Results = “Studies with results,” Phase = “Phase 2 and Phase 3.” No limitations were placed on cancer type or disease stage. Only full-text original clinical research articles published in English were included. The search also excluded conference abstracts, editorials, commentaries, case reports, and study protocols because of incompleteness of data or small sample sizes.
Data collection process
Three independent reviewers (AT, EC, JK) screened the titles and abstracts that were identified from the database search for eligibility. The selected studies were then reviewed as full text by two reviewers independently (AT, KT). Any conflicts were resolved by discussion with a third reviewer (GC). All noted reviewers are included in this manuscript’s author list. Relevant data was then extracted from the studies selected after full-text review and conflict resolution. The data included study design, type of cell-based cancer vaccine, cancer type, clinical setting, sample size and the outcome measures reported.
Quality assessment
The single-arm studies were assessed for quality using the Methodological Index for Non-Randomized Studies (MINORS).Citation11 The quality of controlled trials was evaluated using the Cochrane Risk-of-Bias Tool.Citation12 Quality assessment was done by two independent reviewers (AT and KA), with conflict resolution done via discussion with a third reviewer (GC).
Statistical analysis
In this study, Stata Statistical Software version 17 was used to conduct all statistical analyses. Depending on the nature of the variable, each clinical outcome was analyzed separately using the meta-analysis of proportions (metaprop command) or the meta-analysis of effect sizes (metan command). The meta-analysis summary estimate of the proportions represents the estimated overall rate of the outcome, while the summary estimate of the effect sizes represents the estimated overall association between the vaccine and the outcome. The summary estimates were predicted and presented using random effects estimators. To stabilize the variances of certain proportions that were equal to (or close to) 0 or 1, the Freeman-Tukey (FT) double arcsine transformation was employed. The pooled estimate of the rate was then back transformed and presented with their Wald 95% CI estimated using the Score method. The meta-analysis of effect sizes employed the DerSimonian-Laird (DL) estimator for the variance estimation in the random-effects model. The ICitation2 statistic and its P-value were used to estimate heterogeneity between studies.
Results
Studies selected
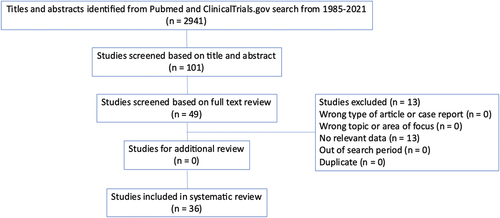
A total of 2,941 studies were identified in the initial database search. After screening of the titles and abstracts, 101 publications were selected for full-text review. After reviewing the full-text articles, 49 studies were included, and no additional articles were identified via review of references. The final review after data extraction included 36 studies, 16 single-arm studies,Citation13–27 and 20 controlled trials.Citation6,Citation28–46 shows the PRISMA flow diagram for steps in the study selection process.
Figure 1. PRISMA flow diagram.
Quality assessment
shows the quality assessment of the single-arm studies using MINORS. There was one study of good quality (score 15–16), 15 studies of moderate quality (score 8–15) and 0 studies of poor quality (score <8). shows the Risk of Bias assessment for the randomized controlled trials along with the sources of funding for the study, when reported. While most of the newer studies were well designed with low risk of bias, lack of blinding was a common drawback seen in the older studies leading to some concerns of bias.
Figure 2. Quality assessment of the controlled studies.
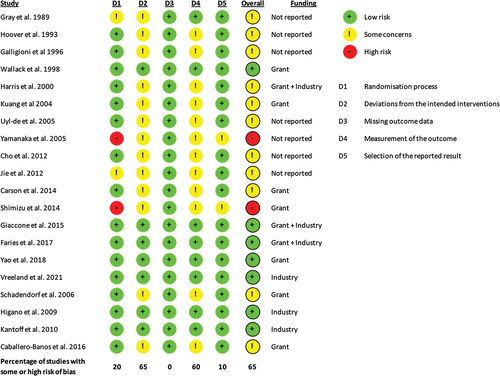
Table 1. Quality assessment of the single-arm studies.
Study characteristics
summarizes the major characteristics of all included studies. Among the 16 single-arm studies included, 12 (75%) were conducted in the advanced/metastatic setting, 3 (19%) looked at recurrent tumors and 1 study, Powell et al.Citation15, looked at primary malignant pleural mesothelioma irrespective of stage, since curative surgical resection was not standard of care (SOC).Citation15 Of the 20 controlled studies included, 16 (80%) were conducted in the adjuvant setting and 4 (20%) were conducted among patients with advanced/metastatic disease. Most of the studies (53%) looked at dendritic cell vaccines, while 8 (22%) and 9 (25%) of the studies tested autologous and allogeneic tumor cell vaccines, respectively. Melanoma was the most common cancer type, in 10 (28%) of the studies. For the controlled studies, nine studies (45%) reported OS data with length of follow-up less than 5 years and 11 studies (55%) reported OS for 5 years or longer.
Table 2. Characteristics of all studies included in the systematic review.
Outcomes
Response based on RECIST criteria from single-arm studies
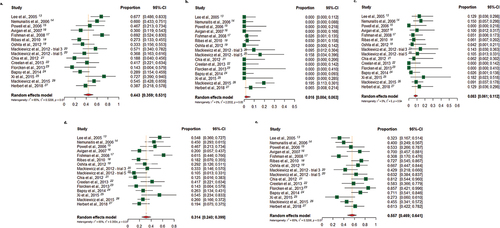
depicts the findings of the meta-analysis evaluating objective response to cell-based cancer vaccines in single-arm trials, using the RECIST criteria. The overall disease control rate (DCR), calculated as the proportion of complete responses (CR), partial responses (PR) and stable disease (SD) was 0.44 (0.36–0.53) using the random effects model (). Looking at the breakdown of the different responses, the proportion of CR was 0.02 (0.00–0.06) (); PR proportion was 0.08 (0.06–0.11) (); and the proportion of SD was 0.31 (0.24–0.40) (). Correspondingly, the rate of progressive disease (PD) was 0.56 (0.47–0.64) ().
Figure 3. Meta-analysis of objective response to cell-based cancer vaccine therapy in single-arm trials, using the response evaluation criteria in solid tumors (RECIST). Figure 3a depicts the findings of the meta-analysis evaluating the disease control rate (DCR) with cell-based cancer vaccines. Figures 3b–e depict the findings of the meta-analysis evaluating the rates of complete response (CR), partial response (PR), stable disease (SD) and progressive disease (PD), respectively.
Overall survival (OS) from controlled studies
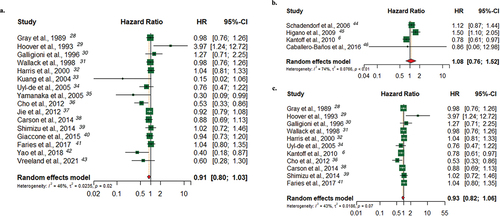
depicts the findings of the meta-analysis evaluating the association between cell-based cancer vaccine therapy and clinical outcome (OS) in controlled trials. Overall, there was no statistically significant improvement in OS across different settings. In the adjuvant setting, a pooled HR of 0.89 (0.79–1.00) was seen () while in the advanced/metastatic setting, a pooled HR of 1.08 (0.76–1.52) was seen (). Looking specifically at studies that reported survival data with ≥5-year follow-up, a pooled HR of 0.91 (0.80–1.03) with a random effects model was observed ().
Figure 4. Meta-analysis of cell-based cancer vaccine therapy and overall survival (OS). Figure 4a depicts the findings of the meta-analysis evaluating the association between cell-based cancer vaccine therapy and clinical outcome (OS) in the adjuvant setting. Figure 4b depicts the findings of the meta-analysis evaluating the association between cell-based cancer vaccine therapy and clinical outcome (OS) in the advanced/metastatic disease setting. Figure 4c depicts the findings of the meta-analysis evaluating the association between cell-based cancer vaccine therapy and clinical outcome (OS) with ≥ 5-year survival follow-up.
Literature review to evaluate biologic activity
While our rigorous systematic review and meta-analysis revealed several negative studies and an overall lack of clinical effect, there are important positive studies that highlight the promise of cell-based cancer vaccines. As we looked beyond the stringent inclusion criteria of our systematic review, we identified significant examples of biological activity of cell-based cancer vaccines that are worth highlighting with the aim of providing a separate and useful summary of approaches involving cellular vaccines that have the potential to be of clinical benefit.
The studies involving Sipuleucel-T, which consists of autologous dendritic cells pulsed with prostatic acid phosphatase (PAP) linked to granulocyte macrophage-colony stimulating factor (GM-CSF), stand out as successful trials that have led to change in clinical practice. Four different trials looking at its effect in metastatic castrate-resistant prostate cancer (CRPC) have demonstrated biological activity that has translated to improved clinical outcomes and has led to Sipuleucel-T becoming FDA approved for metastatic CRPC.Citation6,Citation45,Citation47,Citation48 Several other studies show evidence of biological activity, though they did not meet their primary endpoints. In 2013, Skachkova et al. conducted a study of DCs pulsed with mechanically activated microparticles of lyophilized autologous tumor cells in Stage IIB – IIIA Non-Small Cell Lung Cancer (NSCLC) following surgery.Citation49 They observed distant recurrences in 25% (15/60) of patients who received only surgery (disease-free period – 9.55 ± 1.37 months) versus only 10% (6/60) of patients treated with DC-immunotherapy (disease-free period – 24.92 ± 2.39 months).Citation49 Liau et al. studied autologous tumor lysate-pulsed dendritic cells in newly diagnosed glioblastoma after surgery. Though the cross-over nature of the study made interpretation of the result difficult, the median overall survival (mOS) of 23.1 months from surgery compares favorably with the mOS of 15–17 months from surgery typically achieved with standard of care (SOC).Citation50
Phase III studies of autologous cancer immunotherapies, all in the adjuvant setting, have also had positive data. This included irradiated autologous cancer cells with mixed with Bacillus Calmette-Guerin (BCG) in stage I and III colorectal cancer (CRC) after surgery, which failed to meet the primary endpoint, but did see a significant improvement in survival and disease-free survival (DFS) in eligible colon cancer patients who received autologous cell therapy.Citation29 In another study of autologous tumor cells mixed with BCG in stage II and stage III colon cancer patients, the intention-to-treat (ITT) recurrence free interval was better for active treatment compared with observation (OR 0.75, 95% CI, 0.56–1.00).Citation51 In a second study of the same therapy a beneficial effect of autologous cell immunotherapy was statistically significant for all endpoints including recurrence-free interval (RFI), OS, and recurrence-free survival (RFS) in Stage II colon cancer patients, while there was no beneficial effect in stage III patients.Citation34 A study of autologous tumor cell-lysate in M0 renal cell carcinoma (RCC) post-radical nephrectomy initially showed no significant differences between immunotherapy versus no treatment, but a later analysis of the ITT population showed 5-year and 70-month hazard ratios (HRs) for tumor progression were 1.58 (95% CI 1.05–2.37) and 1.59 (95% CI 1.07–2.36), respectively, in favor of the immunotherapy group and the 5-year and 70-month PFS rates were 77.4% and 72.0%, respectively, in the immunotherapy group versus 67.8% and 59.3%, respectively, in the control group.Citation52,Citation53
For allogeneic cell therapies in the therapeutic setting, a study of Stage III/IV NSCLC patients who did not progress after platinum-based chemotherapy compared treatment with four transforming growth factor (TGF)-β2-antisense gene-modified, irradiated, allogeneic NSCLC cell lines (Belagenpumatucel-L) with placebo.Citation40 Although there were statistically insignificant increases in OS and PFS (median OS 20.3 versus 17.8 months; and, PFS 4.3 months versus 4.0 for immunotherapy vs placebo, both favoring the immunotherapy group, but not statistically significant), in a pre-specified Cox regression analysis of 161 patients who received chemoradiation therapy prior to randomization, median survival was 28.4 months with immunotherapy versus 16.0 months with placebo; HR 0.61, p = .032. In the adjuvant setting, a study of allogeneic melanoma cell lysate plus the detoxified Freund’s adjuvant compared with observation in resected, clinically node negative melanoma.Citation38 While the overall endpoint of OS and DFS was not met (statistically insignificant increases in 5-year and 10-year survival), if the analysis was focused on patients who were HLA-A2+ and/or HLA-Cw3+, there were significant differences in both and OS at 5 years 10 years. Other studies of immunotherapy or a similar live vaccinia virus-augmented allogeneic polyvalent melanoma cell lysate did not show significant improvement in survival. But, it is noteworthy that these studies used cell lysates and not live cells, which may make a difference in mechanism of action and activity.Citation31,Citation54,Citation55
Discussion
Therapeutic cancer vaccination, particularly cell-based cancer vaccines, has been an attractive concept for a long time that is yet to fulfill its promise in the clinical setting. Despite extensive pre-clinical and clinical work, success has remained elusive with only Sipuleucel-T gaining FDA approval, while most attempts have resulted in negative clinical trials. The utility of meta-analysis lies in teasing out effect when individual studies are limited by smaller sample sizes. This provides an important rationale for undertaking this study, as we notice individual trials trending toward survival benefit but failing to reach statistical significance. Another reason to systematically review and meta-analyze the trials on cell-based cancer vaccines is to provide a snapshot and graphically represent the current literature on the topic. This study, to the best of our knowledge, is the first to systematically review the entire spectrum of cell-based cancer vaccines for all cancer types and analyze efficacy. We sought to evaluate measures of objective response from single-arm studies as well as OS outcomes from controlled studies.
Among the included single-arm studies, the highest DCR was observed in the trial by Xi et al., looking at a dendritic cell vaccine for prostate cancer.Citation25 They also had the highest partial response rate of all the included studies, confirming the utility of cellular vaccines in prostate cancer. The maximum proportion of complete responders were observed in the trials by Mackiewicz et al. using an allogeneic whole cell vaccine in melanoma, another cancer known to be responsive to immunotherapy.Citation20,Citation26 On the other hand, high rates of progressive disease were seen in the studies by Chia et al. looking at advanced metastatic nasopharyngeal carcinoma, and Florcken et al. looking at metastatic renal cell cancer.Citation21,Citation23 These are both, of course, aggressive diseases that are challenging to control.
Among the controlled studies that were included, the majority were negative trials and did not demonstrate survival benefit. One of the early studies by Hoover et al. in 1993 was a successful trial, showing survival benefit with an autologous tumor cell vaccine in colon cancer.Citation29 Though limited by sample size, this early trial highlights the promise of cellular cancer vaccines. Since that time, systemic chemotherapy and radiation therapy has improved significantly, possibly contributing to the lack of positive trials with cellular cancer vaccines. Except for the studies with Sipuleucel-T in prostate cancer that have been discussed earlier, the only trials demonstrating survival benefit were Yamanaka et al., Cho et al. and Yao et al.Citation35,Citation36,Citation42 All of these looked at dendritic cell vaccines in patients with glioblastoma, which has poor prognosis with conventional treatments.
Prior meta-analyses on this subject have mostly focused on a particular cancer type. Some of them primarily analyzed the safety of the vaccines while some of them looked at cell-based and peptide vaccines. Botrel et al. in 2012 pooled together the already strong evidence of Sipuleucel-T in metastatic CRPC to further confirm its survival benefit.Citation56 Wang et al. in 2015, and Zhou et al. in 2016 showed survival benefit with therapeutic vaccines in NSCLC though their meta-analyses included cellular and peptide vaccines.Citation57,Citation58 Chen et al. in 2018 meta-analyzed studies on DC-based vaccines in HCC and showed enhanced anti-tumor immunity as well as improved survival.Citation59 More recently, Han et al. in 2023 looked at therapeutic vaccines for HCC, though they included peptide and cell-based vaccines, and focused on safety.Citation60 Lv et al. in 2020 looked at phase II RCTs of DC vaccines in GBM and observed improved survival, though they included studies that used other concurrent therapies in the vaccine arm comparing best supportive care as control.Citation61 Shamshiripour et al. also meta-analyzed studies of DC-based therapy for gliomas, concluding it was safe with minimal grade III/IV adverse events.Citation62 Dafni et al. in 2021 meta-analyzed cancer vaccines (peptide and cell-based vaccines) in breast and ovarian cancer, looking primarily at ORR and observed a modest response rate.Citation63 These studies have provided important evidence for potential benefits of therapeutic cancer vaccines in specific cancer types.
Our systematic review of the existing literature revealed largely negative trials and our meta-analysis did not show evidence of clinical benefit from cell-based cancer-vaccines. A major limitation of this analysis is the heterogeneity of the included studies. Since our focus was solely on cell-based cancer vaccines, irrespective of other factors, a diverse range of studies have been included in our analysis. We have attempted to minimize the impact of heterogeneity by using a random-effects model, as well as classifying the studies based on clinical setting and length of follow-up, yet significant variability still exists with respect to cancer type and vaccine platform used, as reflected in the ICitation2 statistics. While this limits the interpretation of the results, this was expected by virtue of the design of our study and is reflective of the variability of existing literature on the topic of therapeutic cancer vaccination. Broadly speaking, the review suggests a low level of activity for this therapeutic modality as it has been implemented in prior trials.
However, as evidenced by the success of Sipuleucel-T among men with metastatic castration-resistant prostate cancer, there have been successful studies of cellular cancer vaccines. In order to evaluate the potential differentiating features of the successful study, a more granular approach was employed. This revealed that several phase III studies had convincing evidence of biological activity, although some failed to meet their primary endpoints. Interestingly, and contrary to the convential wisdom, phase III studies in the therapeutic setting were as successful or more successful than those in the adjuvant or neoadjuvant settings. This is counter-intuitive as an earlier stage patient might be expected to have a more robust immune system and thus be able to mount a more potent immune response to the vaccination. This may suggest that even in late-stage cancer patients, the immune system may still be robust enough to develop significant anti-cancer activity.
As mentioned earlier, the combination of ICI and therapeutic cancer vaccines has a strong biological rationale to produce synergistic anti-tumor effect. In our systematic review and meta-analysis, we excluded any published trials that were evaluating these combinations. This was done to try and gauge the effect of vaccination alone, without the confounding effect of concurrent treatments. Already there exists early evidence of potential efficacy of the ICI-vaccine combination approach, and we recognize this as a limitation of our study.Citation64–66
Despite these limitations, our study provides an important and timely overview of what has been observed thus far in the field of therapeutic cell-based cancer vaccines and should help serve as a starting place for future trials evaluating the biological activity and clinical impact of cell-based cancer vaccines. Our analysis has identified individual successes that underscore the promise of this therapeutic cell-based cancer vaccine approach. The summary of trials included in this study, along with the pooled meta-analysis, aims to provide an initial step for future, more targeted research.
Conclusions
The existing literature on cell-based cancer vaccines is highly variable in terms of cancer type, vaccine therapies and the clinical setting. Overall, with our applied systematic review and meta-analysis, we found no statistically significant benefit with cell-based cancer vaccines in the adjuvant setting or the metastatic setting. However, individual success, especially with dendritic cell-based vaccines and in the advanced cancer setting, have been well documented. As our understanding of cancer immunology keeps improving and cell-based vaccine technology continues to evolve, future studies can perhaps fulfill the potential that this exciting field of anti-cancer therapy holds.
Author contributions
AT, KA, AS, WW, and GC prepared and drafted the manuscript. GC, AN, WW, TV, ML, GDP, and GP planned the concept and scope of the review. AT, KA, EC, KT, and JK collected the data. AN, SVD, TS, and FV contributed data or analysis tools. KA and AT performed the analysis. AT, ML, GDP, WW, AS, GP, and GC all substantially edited the review. All authors contributed to the article and approved the submitted version.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Kim JM, Chen DS. Immune escape to PD-L1/PD-1 blockade: seven steps to success (or failure). Ann Oncol. 2016;27(8):1492–11. doi:10.1093/annonc/mdw217.
- Gide TN, Wilmott JS, Scolyer RA, Long GV. Primary and acquired resistance to immune checkpoint inhibitors in metastatic melanoma. Clin Cancer Res. 2018;24(6):1260–70. doi:10.1158/1078-0432.CCR-17-2267.
- Hollingsworth RE, Jansen K. Turning the corner on therapeutic cancer vaccines. NPJ Vaccines. 2019;4(1):7. doi:10.1038/s41541-019-0103-y.
- Melief CJ, van Hall T, Arens R, Ossendorp F, van der Burg SH. Therapeutic cancer vaccines. J Clin Invest. 2015;125(9):3401–12. doi:10.1172/JCI80009.
- Wculek SK, Cueto FJ, Mujal AM, Melero I, Krummel MF, Sancho D. Dendritic cells in cancer immunology and immunotherapy. Nat Rev Immunol. 2020;20(1):7–24. doi:10.1038/s41577-019-0210-z.
- Kantoff PW, Higano CS, Shore ND, Berger ER, Small EJ, Penson DF, Redfern CH, Ferrari AC, Dreicer R, Sims RB. et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. 2010;363(5):411–422. doi:10.1056/NEJMoa1001294.
- Hu Z, Ott PA, Wu CJ. Towards personalized, tumour-specific, therapeutic vaccines for cancer. Nat Rev Immunol. 2018;18(3):168–182. doi:10.1038/nri.2017.131.
- Oladejo M, Paulishak W, Wood L. Synergistic potential of immune checkpoint inhibitors and therapeutic cancer vaccines. Semin Cancer Biol. 2023;88:81–95. doi:10.1016/j.semcancer.2022.12.003.
- Sellars MC, Wu CJ, Fritsch EF. Cancer vaccines: building a bridge over troubled waters. Cell. 2022;185(15):2770–2788. doi:10.1016/j.cell.2022.06.035.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71.
- Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. 2003;73(9):712–6. doi:10.1046/j.1445-2197.2003.02748.x.
- Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC. Chapter 8: assessing risk of bias in a randomized trial. In: Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page M, Welch V, editors. Cochrane handbook for systematic reviews of interventions version 6.3 (updated February 2022). Cochrane. www.training.cochrane.org/handbook.
- Lee WC, Wang HC, Hung CF, Huang P-F, Lia C-R, Chen M-F. Vaccination of advanced hepatocellular carcinoma patients with tumor lysate-pulsed dendritic cells: a clinical trial. J Immunother. 2005;28(5):496–504. doi:10.1097/01.cji.0000171291.72039.e2.
- Nemunaitis J, Dillman RO, Schwarzenberger PO, Senzer N, Cunningham C, Cutler J, Tong A, Kumar P, Pappen B, Hamilton C. et al. Phase II study of belagenpumatucel-L, a transforming growth factor beta-2 antisense gene-modified allogeneic tumor cell vaccine in non–small-cell lung cancer. J Clin Oncol. 2006;24(29):4721–30. doi:10.1200/JCO.2005.05.5335.
- Powell A, Creaney J, Broomfield S, Van Bruggen I, Robinson B. Recombinant GM-CSF plus autologous tumor cells as a vaccine for patients with mesothelioma. Lung Cancer. 2006;52(2):189–97. doi:10.1016/j.lungcan.2006.01.007.
- Avigan DE, Vasir B, George DJ, Oh WK, Atkins MB, McDermott DF, Kantoff PW, Figlin RA, Vasconcelles MJ, Xu Y. et al. Phase I/II study of vaccination with electrofused allogeneic dendritic cells/autologous tumor-derived cells in patients with stage IV renal cell carcinoma. J Immunother. 2007;30(7):749–761. doi:10.1097/CJI.0b013e3180de4ce8.
- Fishman M, Hunter TB, Soliman H, Thompson P, Dunn M, Smilee R, Farmelo MJ, Noyes DR, Mahany JJ, Lee J-H. et al. Phase II trial of B7-1 (CD-86) transduced, cultured autologous tumor cell vaccine plus subcutaneous interleukin-2 for treatment of stage IV renal cell carcinoma. J Immunother. 2008;31(1):72–80. doi:10.1097/CJI.0b013e31815ba792.
- Ribas A, Camacho LH, Lee SM, Hersh EM, Brown CK, Richards JM, Rodriguez MJ, Prieto VG, Glaspy JA, Oseguera DK. et al. Multicenter phase II study of matured dendritic cells pulsed with melanoma cell line lysates in patients with advanced melanoma. J Transl Med. 2010;8(1):89. doi:10.1186/1479-5876-8-89.
- Oshita C, Takikawa M, Kume A, Miyata H, Ashizawa T, Iizuka A, Kiyohara Y, Yoshikawa S, Tanosaki R, Yamazaki N. et al. Dendritic cell-based vaccination in metastatic melanoma patients: phase II clinical trial. Oncol Rep. 2012;28(4):1131–1138. doi:10.3892/or.2012.1956.
- Mackiewicz A, Mackiewicz J, Wysocki PJ, Wiznerowicz M, Kapcinska M, Laciak M, Rose-John S, Izycki D, Burzykowski T, Karczewska-Dzionk A. et al. Long-term survival of high-risk melanoma patients immunized with a hyper-IL-6-modified allogeneic whole-cell vaccine after complete resection. Expert Opin Investig Drugs. 2012;21(6):773–783. doi:10.1517/13543784.2012.684753.
- Chia WK, Wang WW, Teo M, Tai WM, Lim WT, Tan EH, Leong SS, Sun L, Chen JJ, Gottschalk S. et al. A phase II study evaluating the safety and efficacy of an adenovirus-ΔLMP1-LMP2 transduced dendritic cell vaccine in patients with advanced metastatic nasopharyngeal carcinoma. Ann Oncol. 2012;23(4):997–1005. doi:10.1093/annonc/mdr341.
- Creelan BC, Antonia S, Noyes D, Hunter TB, Simon GR, Bepler G, Williams CC, Tanvetyanon T, Haura EB, Schell MJ. et al. Phase II trial of a GM-CSF-producing and CD40L-expressing bystander cell line combined with an allogeneic tumor cell–based vaccine for refractory lung adenocarcinoma. J Immunother. 2013;36(8):442–50. doi:10.1097/CJI.0b013e3182a80237.
- Florcken A, Kopp J, van Lessen A, van Lessen A, Movassaghi K, Takvorian A, Jöhrens K, Möbs M, Schönemann C, Sawitzki B. et al. Allogeneic partially HLA-matched dendritic cells pulsed with autologous tumor cell lysate as a vaccine in metastatic renal cell cancer: a clinical phase I/II study. Hum Vaccin Immunother. 2013;9(6):1217–27. doi:10.4161/hv.24149.
- Bapsy PP, Sharan B, Kumar C, Das RP, Rangarajan B, Jain M, Suresh Attili VS, Subramanian S, Aggarwal S, Srivastava M. et al. Open-label, multi-center, non-randomized, single-arm study to evaluate the safety and efficacy of dendritic cell immunotherapy in patients with refractory solid malignancies, on supportive care. Cytotherapy. 2014;16(2):234–244. doi:10.1016/j.jcyt.2013.11.013.
- Xi HB, Wang GX, Fu B, Liu W-P, Li Y. Survivin and PSMA loaded dendritic cell vaccine for the treatment of prostate cancer. Biol Pharm Bull. 2015;38(6):827–35. doi:10.1248/bpb.b14-00518.
- Mackiewicz J, Karczewska-Dzionk A, Laciak M, Kapcinska M, Wiznerowicz M, Burzykowski T, Zakowska M, Rose-John S, Mackiewicz A. Whole cell therapeutic vaccine modified with hyper-IL6 for combinational treatment of nonresected advanced melanoma. Medicine (Baltimore). 2015;94(21):e853. doi:10.1097/MD.0000000000000853.
- Herbert GS, Vreeland TJ, Clifton GT, Greene JM, Jackson DO, Hardin MO, Hale DF, Berry JS, Nichol P, Yin S. et al. Initial phase I/IIa trial results of an autologous tumor lysate, particle-loaded, dendritic cell (TLPLDC) vaccine in patients with solid tumors. Vaccine. 2018;36(23):3247–3253. doi:10.1016/j.vaccine.2018.04.078.
- Gray BN, Walker C, Andrewartha L, Freeman S, Bennett RC. Controlled clinical trial of adjuvant immunotherapy with BCG and neuraminidase-treated autologous tumour cells in large bowel cancer. J Surg Oncol. 1989;40(1):34–7. doi:10.1002/jso.2930400109.
- Hoover HC Jr., Brandhorst JS, Peters LC, Surdyke MG, Takeshita Y, Madariaga J, Muenz LR, Hanna MG. Adjuvant active specific immunotherapy for human colorectal cancer: 6.5-year median follow-up of a phase III prospectively randomized trial. J Clin Oncol. 1993;11(3):390–9. doi:10.1200/JCO.1993.11.3.390.
- Galligioni E, Quaia M, Merlo A, Carbone A, Spada A, Favaro D, Santarosa M, Sacco C, Talamini R, Gruppo Oncologico Clinico Coope T. Adjuvant immunotherapy treatment of renal carcinoma patients with autologous tumor cells and Bacillus Calmette-Guèrin: five-year results of a prospective randomized study. Cancer. 1996;77(12):2560–6. doi:10.1002/(SICI)1097-0142(19960615)77:12<2560:AID-CNCR20>3.0.CO;2-P.
- Wallack MK, Sivanandham M, Balch CM, Urist MM, Bland KI, Murray D, Robinson WA, Flaherty L, Richards JM, Bartolucci AA. et al. Surgical adjuvant active specific immunotherapy for patients with stage III melanoma: the final analysis of data from a phase III, randomized, double-blind, multicenter vaccinia melanoma oncolysate trial. J Am Coll Surg. 1998;187(1):69–77; discussion 77–69. doi:10.1016/S1072-7515(98)00097-0.
- Harris JE, Ryan L, Hoover HC Jr., Stuart RK, Oken MM, Benson AB, Mansour E, Haller DG, Manola J, Hanna MG. Adjuvant active specific immunotherapy for stage II and III colon cancer with an autologous tumor cell vaccine: eastern cooperative oncology group study E5283. J Clin Oncol. 2000;18(1):148–57. doi:10.1200/JCO.2000.18.1.148.
- Kuang M, Peng BG, Lu MD, Liang LJ, Huang JF, He Q, Hua YP, Totsuka S, Liu SQ, Leong KW. et al. Phase II randomized trial of autologous formalin-fixed tumor vaccine for postsurgical recurrence of hepatocellular carcinoma. Clin Cancer Res. 2004;10(5):1574–1579. doi:10.1158/1078-0432.CCR-03-0071.
- Uyl-de Groot CA, Vermorken JB, Hanna MG Jr., Verboom P, Groot M, Bonsel G, Meijer C, Pinedo H. Immunotherapy with autologous tumor cell-BCG vaccine in patients with colon cancer: a prospective study of medical and economic benefits. Vaccine. 2005;23(17–18):2379–87. doi:10.1016/j.vaccine.2005.01.015.
- Yamanaka R, Homma J, Yajima N, Tsuchiya N, Sano M, Kobayashi T, Yoshida S, Abe T, Narita M, Takahashi M. et al. Clinical evaluation of dendritic cell vaccination for patients with recurrent glioma: results of a clinical phase I/II trial. Clin Cancer Res. 2005;11(11):4160–4167. doi:10.1158/1078-0432.CCR-05-0120.
- Cho DY, Yang WK, Lee HC, Hsu D-M, Lin H-L, Lin S-Z, Chen C-C, Harn H-J, Liu C-L, Lee W-Y. et al. Adjuvant immunotherapy with whole-cell lysate dendritic cells vaccine for glioblastoma multiforme: a phase II clinical trial. World Neurosurg. 2012;77(5–6):736–744. doi:10.1016/j.wneu.2011.08.020.
- Jie X, Hua L, Jiang W, Feng F, Feng G, Hua Z. Clinical application of a dendritic cell vaccine raised against heat-shocked glioblastoma. Cell Biochem Biophys. 2012;62(1):91–9. doi:10.1007/s12013-011-9265-6.
- Carson WE 3rd, Unger JM, Sosman JA, Flaherty LE, Tuthill RJ, Porter MJ, Thompson JA, Kempf RA, Othus M, Ribas A. et al. Adjuvant vaccine immunotherapy of resected, clinically node-negative melanoma: long-term outcome and impact of HLA class I antigen expression on overall survival. Cancer Immunol Res. 2014;2(10):981–7. doi:10.1158/2326-6066.CIR-14-0052.
- Shimizu K, Kotera Y, Aruga A, Takeshita N, Katagiri S, Ariizumi S-I, Takahashi Y, Yoshitoshi K, Takasaki K, Yamamoto M. Postoperative dendritic cell vaccine plus activated T-cell transfer improves the survival of patients with invasive hepatocellular carcinoma. Hum Vaccin Immunother. 2014;10(4):970–6. doi:10.4161/hv.27678.
- Giaccone G, Bazhenova LA, Nemunaitis J, Tan M, Juhász E, Ramlau R, van den Heuvel MM, Lal R, Kloecker GH, Eaton KD. et al. A phase III study of belagenpumatucel-L, an allogeneic tumour cell vaccine, as maintenance therapy for non-small cell lung cancer. Eur J Cancer. 2015;51(16):2321–2329. doi:10.1016/j.ejca.2015.07.035.
- Faries MB, Mozzillo N, Kashani-Sabet M, Thompson JF, Kelley MC, DeConti RC, Lee JE, Huth JF, Wagner J, Dalgleish A. et al. Long-term survival after complete surgical resection and adjuvant immunotherapy for distant melanoma metastases. Ann Surg Oncol. 2017;24(13):3991–4000. doi:10.1245/s10434-017-6072-3.
- Yao Y, Luo F, Tang C, Chen D, Qin Z, Hua W, Xu M, Zhong P, Yu S, Chen D. et al. Molecular subgroups and B7-H4 expression levels predict responses to dendritic cell vaccines in glioblastoma: an exploratory randomized phase II clinical trial. Cancer Immunol Immunother. 2018;67(11):1777–1788. doi:10.1007/s00262-018-2232-y.
- Vreeland TJ, Clifton GT, Hale DF, Chick RC, Hickerson AT, Cindass JL, Adams AM, Bohan PMK, Andtbacka RHI, Berger AC. et al. A phase IIb randomized controlled trial of the TLPLDC vaccine as adjuvant therapy after surgical resection of stage III/IV melanoma: a primary analysis. Ann Surg Oncol. 2021;28(11):6126–6137. doi:10.1245/s10434-021-09709-1.
- Schadendorf D, Ugurel S, Schuler-Thurner B, Nestle FO, Enk A, Bröcker E-B, Grabbe S, Rittgen W, Edler L, Sucker A. et al. Dacarbazine (DTIC) versus vaccination with autologous peptide-pulsed dendritic cells (DC) in first-line treatment of patients with metastatic melanoma: a randomized phase III trial of the DC study group of the DeCOG. Ann Oncol. 2006;17(4):563–570. doi:10.1093/annonc/mdj138.
- Higano CS, Schellhammer PF, Small EJ, Burch PA, Nemunaitis J, Yuh L, Provost N, Frohlich MW. Integrated data from 2 randomized, double-blind, placebo-controlled, phase 3 trials of active cellular immunotherapy with sipuleucel-T in advanced prostate cancer. Cancer. 2009;115(16):3670–9. doi:10.1002/cncr.24429.
- Caballero-Banos M, Benitez-Ribas D, Tabera J, Varea S, Vilana R, Bianchi L, Ayuso JR, Pagés M, Carrera G, Cuatrecasas M. et al. Phase II randomised trial of autologous tumour lysate dendritic cell plus best supportive care compared with best supportive care in pre-treated advanced colorectal cancer patients. Eur J Cancer. 2016;64:167–174. doi:10.1016/j.ejca.2016.06.008.
- Beer TM, Bernstein GT, Corman JM, Glode LM, Hall SJ, Poll WL, Schellhammer PF, Jones LA, Xu Y, Kylstra JW. et al. Randomized trial of autologous cellular immunotherapy with sipuleucel-T in androgen-dependent prostate cancer. Clin Cancer Res. 2011;17(13):4558–4567. doi:10.1158/1078-0432.CCR-10-3223.
- George DJ, Nabhan C, DeVries T, Whitmore JB, Gomella LG. Survival outcomes of sipuleucel-T phase III studies: impact of control-arm cross-over to salvage immunotherapy. Cancer Immunol Res. 2015;3(9):1063–9. doi:10.1158/2326-6066.CIR-15-0006.
- Skachkova OV, Khranovska NM, Gorbach OI, Svergun NM, Sydor RI, Nikulina VV. Immunological markers of anti-tumor dendritic cells vaccine efficiency in patients with non-small cell lung cancer. Exp Oncol. 2013;35:109–13.
- Liau LM, Ashkan K, Tran DD, Campian JL, Trusheim JE, Cobbs CS, Heth JA, Salacz M, Taylor S, D’Andre SD. et al. First results on survival from a large Phase 3 clinical trial of an autologous dendritic cell vaccine in newly diagnosed glioblastoma. J Transl Med. 2018;16(1):142. doi:10.1186/s12967-018-1507-6.
- Hanna MG Jr., Hoover HC Jr., Vermorken JB, Harris JE, Pinedo HM. Adjuvant active specific immunotherapy of stage II and stage III colon cancer with an autologous tumor cell vaccine: first randomized phase III trials show promise. Vaccine. 2001;19(17–19):2576–82. doi:10.1016/S0264-410X(00)00485-0.
- Doehn C, Richter A, Lehmacher W, Jocham D. Adjuvant autologous tumour cell-lysate vaccine versus no adjuvant treatment in patients with M0 renal cell carcinoma after radical nephrectomy: 3-year interim analysis of a German multicentre phase-III trial. Folia Biol (Praha). 2003;49(2):69–73. doi:10.1016/S1569-9056(03)80393-7.
- Jocham D, Richter A, Hoffmann L, Iwig K, Fahlenkamp D, Zakrzewski G, Schmitt E, Dannenberg T, Lehmacher W, von Wietersheim J. et al. Adjuvant autologous renal tumour cell vaccine and risk of tumour progression in patients with renal-cell carcinoma after radical nephrectomy: phase III, randomised controlled trial. Lancet. 2004;363(9409):594–599. doi:10.1016/S0140-6736(04)15590-6.
- Sondak VK, Liu PY, Tuthill RJ, Kempf RA, Unger JM, Sosman JA, Thompson JA, Weiss GR, Redman BG, Jakowatz JG. et al. Adjuvant immunotherapy of resected, intermediate-thickness, node-negative melanoma with an allogeneic tumor vaccine: overall results of a randomized trial of the Southwest Oncology Group. J Clin Oncol. 2002;20(8):2058–2066. doi:10.1200/JCO.2002.08.071.
- Wallack MK, Sivanandham M, Balch CM, Urist MM, Bland KI, Murray D, Robinson WA, Flaherty LE, Richards JM, Bartolucci AA. et al. A phase III randomized, doúble-blind, multiinstitutional trial of vaccinia melanoma oncolysate-active specific immunotherapy for patients with stage II melanoma. Cancer. 1995;75(1):34–42. doi:10.1002/1097-0142(19950101)75:1<34:AID-CNCR2820750108>3.0.CO;2-0.
- Botrel TE, Clark O, Pompeo AC, Bretas FFH, Sadi MV, Ferreira U, Reis RBD. Immunotherapy with Sipuleucel-T (APC8015) in patients with metastatic castration-refractory prostate cancer (mCRPC): a systematic review and meta-analysis. Int Braz J Urol. 2012;38(6):717–27. doi:10.1590/1677-553820133806717.
- Wang M, Cao JX, Liu YS, Xu B-L, Li D, Zhang X-Y, Li J-L, Liu J-L, Wang H-B, Wang Z-X. et al. Evaluation of tumour vaccine immunotherapy for the treatment of advanced non-small cell lung cancer: a systematic meta-analysis. BMJ Open. 2015;5(4):e006321. doi:10.1136/bmjopen-2014-006321.
- Zhou L, Wang XL, Deng QL, Du Y-Q, Zhao N-Q. The efficacy and safety of immunotherapy in patients with advanced NSCLC: a systematic review and meta-analysis. Sci Rep. 2016;6:32020. doi:10.1038/srep32020.
- Chen C, Ma Yh, Zhang Yt, Zhang F, Zhou N, Wang X, Liu T, Li Y-M. Effect of dendritic cell–based immunotherapy on hepatocellular carcinoma: a systematic review and meta-analysis. Cytotherapy. 2018;20(8):975–89. doi:10.1016/j.jcyt.2018.06.002.
- Han CL, Yan YC, Yan LJ, Meng G-X, Yang C-C, Liu H, Ding Z-N, Dong Z-R, Hong J-G, Chen Z-Q. et al. Efficacy and security of tumor vaccines for hepatocellular carcinoma: a systemic review and meta-analysis of the last 2 decades. J Cancer Res Clin Oncol. 2023;149(4):1425–1441. doi:10.1007/s00432-022-04008-y.
- Lv L, Huang J, Xi H, Zhou X. Efficacy and safety of dendritic cell vaccines for patients with glioblastoma: a meta-analysis of randomized controlled trials. Int Immunopharmacol. 2020;83:106336. doi:10.1016/j.intimp.2020.106336.
- Shamshiripour P, Nikoobakht M, Mansourinejad Z, Ahmadvand D, Akbarpour M. A comprehensive update to dendritic cell therapy for glioma: a systematic review and meta-analysis. Expert Rev Vaccines. 2022;21(4):513–31. doi:10.1080/14760584.2022.2027759.
- Dafni U, Martin-Lluesma S, Balint K, Tsourti Z, Vervita K, Chenal J, Coukos G, Zaman K, Sarivalasis A, Kandalaft LE. et al. Efficacy of cancer vaccines in selected gynaecological breast and ovarian cancers: a 20-year systematic review and meta-analysis. Eur J Cancer. 2021;142:63–82. doi:10.1016/j.ejca.2020.10.014.
- Le DT, Lutz E, Uram JN, Sugar EA, Onners B, Solt S, Zheng L, Diaz LA, Donehower RC, Jaffee EM. et al. Evaluation of ipilimumab in combination with allogeneic pancreatic tumor cells transfected with a GM-CSF gene in previously treated pancreatic cancer. J Immunother. 2013;36(7):382–389. doi:10.1097/CJI.0b013e31829fb7a2.
- Scholz M, Yep S, Chancey M, Kelly C, Chau K, Turner J, Lam R, Drake C. Phase I clinical trial of sipuleucel-T combined with escalating doses of ipilimumab in progressive metastatic castrate-resistant prostate cancer. Immunotargets Ther. 2017;6:11–16. doi:10.2147/ITT.S122497.
- De Keersmaecker B, Claerhout S, Carrasco J, Bar I, Corthals J, Wilgenhof S, Neyns B, Thielemans K. TriMix and tumor antigen mRNA electroporated dendritic cell vaccination plus ipilimumab: link between T-cell activation and clinical responses in advanced melanoma. J Immunother Cancer. 2020;8(1):e000329. doi:10.1136/jitc-2019-000329.