

ABSTRACT
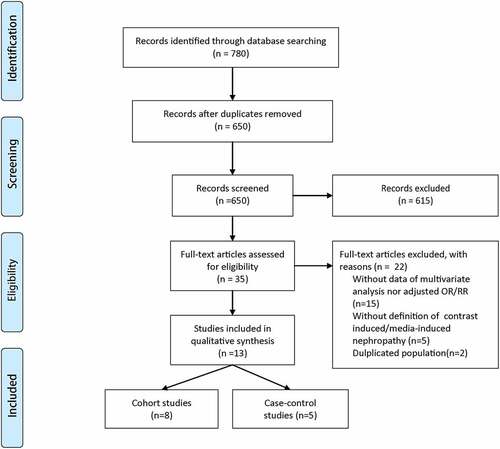
Previous studies have identified numerous risk factors of contrast-induced acute kidney injury (CI-AKI) in patients undergoing coronary angiography. However, the association between anemia and CI-AKI remains conflicting. Thus, we conducted a meta-analysis to further clarify the relationship between anemia and CI-AKI. PubMed, EMBASE and Web of Science were systematically searched from inception to June 2020 to identify eligible studies. The pooled odds ratios (ORs) with 95% confidence intervals (CIs) were used to estimate the correlation between anemia and CI-AKI. The potential publication bias was estimated using funnel plot and Begg’s test. A total of 13 studies (five case-control studies and eight cohort studies) comprising 27,135 patients were included. The pooled results showed that anemia was a significant risk factor of CI-AKI (OR, 1.82; 95% CI, 1.27–2.61). Moreover, the results of subgroup analyses and sensitivity analyses were basically consistent with the overall pooled result. Funnel plot and Begg’s test indicated that there existed potential publication bias, but the result of trim and filled analysis showed that the pooled results kept stable after adding ‘missing’ studies. This meta-analysis suggested that anemia may be correlated with an increased incidence of CI-AKI in patients undergoing coronary angiography. However, our conclusions should be interpreted with caution due to some limitations. Therefore, further high-quality trials should be conducted to confirm our findings.
Graphical abstract
Highlights
1. Anemia may be correlated with CI-AKI.
2. Association between anemia and CI-AKI may vary from ethnicity.
3. Association between anemia and CI-AKI may vary from the definition of anemia.
Acknowledgements
This study was supported by Health Industry Scientific Research Project of Gansu Province of China (NO. GSWSKY-2019-92).
Author contributions
Yu J designed this study. Liang W and Yu C took responsibility for data extraction and analysis. Liang W and Wang Q wrote this manuscript together. All co-authors have checked and approved the final version of the manuscript.
Disclosure statement
All the authors had no conflicts of interest or financial ties to disclose.