

ABSTRACT
Colorectal cancer (CRC) is one of the most important causes of morbidity and mortality in the developed world and is gradually more frequent in the developing world including Saudi Arabia. According to the Saudi Cancer Registry report 2015, CRC is the most common cancer in men (14.9%) and the second most prevalent cancer. Oncogenic mutations in the KRAS gene play a central role in tumorigenesis and are mutated in 30–40% of all CRC patients. To explore the prevalence of KRAS gene mutations in the Saudi population, we collected 80 CRC tumor tissues and sequenced the KRAS gene using automated sequencing technologies. The chromatograms presented mutations in 26 patients (32.5%) in four different codons, that is, 12, 13, 17, and 31. Most of the mutations were identified in codon 12 in 16 patients (61.5% of all mutations). We identified a novel mutation c.51 G>A in codon 17, where serine was substituted by arginine (S17R) in four patients. We also identified a very rare mutation, c.91 G>A, in which glutamic acid was replaced by lysine (E31K) in three patients. In conclusion, our findings further the knowledge about KRAS mutations in different ethnic groups is indispensable to fully understand their role in the development and progression of CRC.
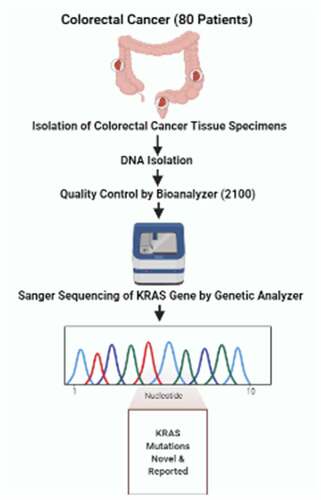
GRAPHICAL ABSTRACT
Highlights
Frequency and mutational spectrum of KRAS gene in colorectal cancer patients.
Discovery of a novel mutation c.51G>A (S17R) in four patients.
Identification of a very rare mutation c.91G>A (E31K).
Limitations and Future Recommendations
More studies with larger patient samples are needed to establish mutational spectrum in Saudi population. Further functional characterization of these mutations is needed to fully understand their role in the development and progression of CRC.
Acknowledgements
This study was funded by King Abdulaziz University under grant No. (1-117-1434-HiCi). The authors acknowledge the technical and financial support of KAU.
Open Access funding provided by the Qatar National Library.
Disclosure statement
No potential conflict of interest was reported by the author(s).