
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Although arsenic contamination was originally considered an environmental problem, its impact on human beings is now widely deemed a serious health issue. This study examines whether international communities perceive arsenic as a health issue and discusses current challenges regarding arsenic contamination in Cambodia. Using comprehensive panel data covering 122 health aid recipient countries across three-plus decades (1990–2020), the first part of our study finds that the recipients’ health needs caused by major incidences (HIV, tuberculosis, and malaria) are all important factors determining health aid. However, health aid is conditionally effective on countries with high arsenic contamination when they have a better governance level. In this context, we conduct a case study focusing on Cambodia, where arsenic contamination is quite serious but given less attention than in other countries. In Cambodia, both inter-governmental coordination and coordination among international organizations are weak, and no long-term blueprint for arsenic mitigation has yet been developed. To fundamentally and sustainably address this problem, we suggest that Cambodia establish a control tower incorporating government, research institutes, and international agencies.
1. Introduction
Development assistance to the health sector has soared over the past two decades. Ravishankar et al. (Citation2009) found that the amount of such aid rose from $5.6 billion USD in 1990 to $21.8 billion in 2007, and that it has skyrocketed since 2002 because of increased funds from bilateral donor governments (in particular, the United States) and private funding, including philanthropic donations and corporate contributions. Meanwhile, Piva and Dodd (Citation2009) showed that health initiatives have become increasingly prioritized in international development over the past decade. Since the COVID-19 pandemic, in particular, official development assistance to the health sector has scaled up considerably, from approximately $16.22 billion in 2019 to $31.86 billion in 2021 (constant price) (Ahmad and Carey Citation2021; OECD Citation2023).
Three of the eight Millennium Development Goals (MDGs) address health issues – Goal 4 (reduce child mortality), Goal 5 (improve maternal health), and Goal 6 (combat HIV/AID, malaria, and other diseases) These issues are more comprehensively and specifically discussed in in Goals 3 (Good Health and Well-being), 6 (Clean Water and Sanitation), 14 (Life Below Water), and 15 (Life on Land) of the Sustainable Development Goals (SDGs). The World Health Organization (WHO Citation2005) pointed out that ‘Health is the heart of the MDGs,’ thus recognizing its importance in reducing poverty and achieving human well-being, as well as emphasizing further disbursement.
While many studies – from McKinlay and Little (Citation1977), Burnside and Dollar (Citation2000), and Berthélemy and Tichit (Citation2004) to Kim and Oh (Citation2012) and Oh and Kim (Citation2015) – have empirically examined the determinants and effectiveness of aid in general, studies examining health-specific aid remain relatively scarce (Lane and Glassman Citation2007; Lim et al. Citation2012; Ravishankar et al. Citation2009). Lane and Glassman (Citation2007) found that health aid improvements in terms of consolidation and increased attention to efficiency generally meet recipients’ needs. Lim et al. (Citation2012) measured risk factors for different disease burdens and found that those risks differed by periods, transitioning from communicable diseases in children to non-communicable diseases in adults. In another vein, Ravishankar et al. (Citation2009) examined 1990–2007 Development Assistance to Health (DAH) from the Institute for Health Metrics and Evaluation (IHME) and found that DAH quadrupled during that period (from $5.6 billion to $21.8 billion), with the proportion varying by organization and the increase boosting funds to improve global health – addressing HIV/AIDS (most notably), tuberculosis, and malaria.
After reviewing past literature, we employ DAH (Ravishankar et al. Citation2009) as a dependent variable and empirically examine its determinants, adopting the same approach as Lane and Glassman (Citation2007) but using a comprehensive dataset that includes more variables and up-to-date time periods. In particular, we pay special attention to arsenic as a determining factor, which previous studies have not done despite it being linked directly to the Sustainable Development Goal 6.1 – that is, universal and equitable access to safe and affordable drinking water by 2030 (UNICEF Citation2019). In fact, although arsenic itself was originally an environmental problem because it contaminates drinking water, it is now a major health issue to which over 140 million people in 70 countries are exposed (WHO Citation2023). Indeed, arsenic is highly toxic – it can cause skin lesions, cancer, and developmental defects in children. Moreover, it is invisible, odorless, and tasteless, which exacerbates the difficulty of raising public awarenessFootnote1 regarding the danger of this deadly poison.
Against this backdrop, we develop hypotheses to investigate various determinants of health aid. While Lane and Glassman (Citation2007) selected income, population, and health expenditures as main explanatory variables, we go further, adding recipients’ health needs stemming from major incidences (HIV, tuberculosis, malaria, as well as arsenic contamination), and governanceFootnote2 levels and employing a dataset that includes data up until 2020, based on the IHME’s DAH’s availability.
This study focuses on Cambodia, a country that has received little academic attention (Petrusevski et al. Citation2008) even though the well water in certain areas of the country have some of the world’s highest arsenic levels (Jones and Khaira Citation2014). The risk is relatively higher for residents in Kandal province than in Kampong Cham and others. In examining the Cambodian case, we give particular attention to coordination among the country’s different stakeholders, including government ministries, bilateral development agencies, international organizations, non-governmental organizations (NGOs), and universities (e.g. Gibson et al. Citation2016), closely examining the country’s Arsenic Inter-Ministerial Sub Committee (AISC).
This paper is organized as follows. Section two explains the research design and presents the hypotheses. Section three describes the study’s data and methodology. Section four summarizes the findings and discusses key results. Section five addresses the Cambodian case. Finally, section six concludes the study by discussing the implications of our findings.
2. Research design and hypotheses
To examine determinants of health aid, we test the following hypotheses. We derive Hypothesis 1 from Lane and Glassman (Citation2007), who set income, population, and health expenditures as main explanatory variables, and Hypothesis 2 from Alesina and Dollar (Citation2000), who focused on aid effectiveness. We go further than both of these previous studies, adding factors to be analyzed, including disease incidence, governance, and – crucially – arsenic contamination.
Hypothesis 1: The most important determinant of health aid (DAH) is the health need of recipient countries; specifically, because countries in which HIV, tuberculosis (TUB), and malaria are prevalent receive more funding, these three health needs along with life expectancy (a natural indicator of a country’s health status) are key determinants of health aid.
Hypothesis 2: Since governance in recipient countries is an important determining factor, countries with stronger governance receive more DAH funding.
Hypothesis 3: When the international community regards arsenic as a health issue rather than an environmental one, countries with serious arsenic contamination receive more health aid (DAH), depending on their governance level.
Fundamentally, Hypothesis 1 posits that health aid volumes (measured by IHME’s DAH) are proportional to countries’ needs (i.e. more funding for HIV, TUB, and malaria in countries where the corresponding diseases are prevalent). Therefore, we expect all these factors to have positive signs. In addition to sector-specific disbursement, we consider health aid total disbursement to test whether it is positively associated with the health needs. Here, we include life expectancy and expect its sign to be negative.
We derive Hypothesis 2 from studies on aid efficacy, which have shown associations between growth in aid and recipients’ governance levels; countries with good governance have both the capacities and capabilities to link aid amounts and growth (Burnside and Dollar Citation2000). Measuring governance numerically can be challenging. This study employs three indicators from the following sources – the Country Policy Institutional Assessment (CPIA), produced solely by World Governance Indicator (WGI), jointly produced by the World Bank and Brookings Institution. The former ranges from 1 (low) to 6 (high) based on 16 criteria in four clusters (economic management, structural policies, policies for social inclusion and equity, and public sector management and institutions), out of which this study used two criteria that are directly relevant to governance (property rights and rule-based governance, and transparency, accountability, and corruption). The WGI ranges from −2.5 to 2.5, capturing perceptions of the quality of public and civil services as well as the quality of policy formulation and implementation. We used an unweighted average of these three, based on which we hypothesize that donor countries tend to provide more aid to countries with good governance, making the expected sign of governance positive.
Hypothesis 3 is the primary focus of this study; in it, we postulate that countries with high arsenic contamination receive more funding. Our analysis interacts this dummy variable with governance, the main variable in Hypothesis 2, to check whether it magnifies the effects on the determinants of DAH. The interaction term could partially differentiate the dependent variable (DAH) with respect to governance level, thereby revealing its marginal effect. Thus, it should demonstrate whether the arsenic binary dummy makes any difference in the governance-aid nexus.
3. Data and methodology
We employ panel data, covering 122 countries whose health sectors received development assistance over the three-plus decades between 1990 and 2020.Footnote3 As dependent variables (denoted as DAH), we mainly use the total amount of DAH each country received (thousand constant 2021 US dollars), collected by the Institute for Health Metrics and Evaluation (IHME). In addition, we use specific DAH amounts to fight HIV, tuberculosis, and malaria (thousand constant 2021 US dollars), all of which we derive from the IHME, as well.
We derive all our independent variables from the World Bank’s World Development Indicator (WDI). The first, a group of variables, denoted as Health in Equations (1) and (2), refers to the incidence of major diseases – HIV (per 1000 uninfected population), tuberculosis (per 100,000 people), and malaria (per 1000 population at risk), followed by life expectancy at birth (years). Next, we adopt the arsenic dummy, coded as 1 for countries that have reported substantial arsenic contamination in their ground water and 0 otherwiseFootnote4 (Shaji et al. Citation2021; WHO Citation2023).
The remaining explanatory variables concern socio-economic status; we consider GDP per capita (denoted as PGDP, constant 2017 international dollar), population (denoted as POP, the number of people), and health expenditures per capita (denoted as EXP, current international dollar). Lastly, we use governance, denoted as GOV – an unweighted average of three criteria, two from CPIA and one from WGI, introduced in the previous section – in the second estimation, interacting it with the arsenic dummy. This leads to the following two equations, Equation (1) for the first estimation and (2) for the second.
(1)
(1)
(2)
(2)
Except for the binary dummy for arsenic and (the unweighted average of) the categorical variable for governance, we log-transform all the explanatory variables to consider different units. provides more detailed explanations of the variables and their summary statistics. We lag all the variables for one year to avoid any potential endogeneity problems.
Table 1. Summary statistics for variables and grouping.
Regarding methodology, this study uses a Tobit estimation because several dependent variables include zero values. Theoretically, a Tobit model provides the censored result, coding a dependent variable of zero as the left-censored lower limit – a practice that is frequently used in other empirical studies of foreign aid, which naturally contain many zero values in each observation (Alesina and Dollar Citation2000; Berthélemy and Tichit Citation2004; Kim and Oh Citation2012; Li, Zeng, and Fan Citation2008).Footnote5
4. Results
shows results for Hypothesis 1 and part of Hypothesis 3, based on Equation (1). The first five columns use total amount of DAH as a dependent variable (denoted as TOTAL in ). Three of them contain only one health-incidence variable in each analysis (HIV, tuberculosis, and malaria), followed by life expectancy in the fourth column, and finally, all the incidences together (column five). For the remainder, we use specific DAHs to HIV, tuberculosis, and malaria as dependent variables (denoted as HIV, TUB, and MAL in the table) to test the corresponding disease risk (e.g. HIV-specific DAH to HIV incidence, etc.)
Table 2. Determinants of DAH (Development Assistance to Health): Tobit model.
In general, we find that the health status variables consistently have the expected signs, regardless of the dependent variables (total DAH or specific ones). That is, the coefficients for HIV, tuberculosis, and malaria are all significantly positive, and those for life expectancy are significantly negative, confirming Hypothesis 1. The fact that the signs of the arsenic dummy variables are positive also confirms Hypothesis 3; countries with major arsenic contamination receive, on average, 1.12–1.22Footnote6 times more funding than others; although this difference may not appear dramatic, it is statistically significant across all estimations.
Following the approach of several international development studies (Alesina and Dollar Citation2000; Berthélemy and Tichit Citation2004; Kim and Oh Citation2012), we use both linear and quadratic terms for GDP per capita and population – a more advanced approach than that of Lane and Glassman (Citation2007), who only used linear terms. Across all estimations, the signs for GDP per capita are all significantly positive for the linear term and negative for the quadratic term. This implies that a country’s GDP per capita positively impacts health aid, albeit at a diminishing rate. We find the same pattern for the population variable, although the results are neither as consistent nor as significant as those for GDP per capita. Lastly, consistent with Lane and Glassman (Citation2007), our analyses shows positive signs for health expenditures in all columns.
shows results related to Hypothesis 2, which concerns the effects of arsenic incidence on the aid countries receive. With total DAH as the only dependent variable, we conduct five Tobit regression analyses, corresponding to the first five columns in . The overall results are essentially the same as the previous outcomes, generating positive coefficients for HIV, tuberculosis, malaria, arsenic, and health expenditures, negative coefficients for life expectancy, and consistent results for GDP per capita and population.
Table 3. Determinants of DAH: extended Tobit model.
What differentiates this table from the preceding table is the inclusion of a new variable, governance ( in Equation [2]), which we find to be significantly positive (ranging from 0.134 to 0.148). This is an expected result, given that governance is measured based on a mixture of CPIA (1 for low and 6 for high) and WGI (−2.5 for low and 2.5 for high), capturing rule-based governance, transparency, accountability, and quality of public and civil services; in short, we find that countries with better governance tend to secure more funding. Very interestingly, when we interact this variable with the arsenic dummy (
in Equation [2]), the coefficients become significantly negative in all cases. The partial derivative with respect to governance level (known as the marginal effect) reveals that when the arsenic dummy is zero, the marginal effect is equal to β3 (significantly positive), which becomes β3 + β4, when the dummy is equal to one (countries with high arsenic contamination). The negative coefficients of
cancel out the positive impact of β3, and β3 + β4 turns negative in all columns (e.g. 0.135–0.272 = −0.137 in the first column) except the second one. In other words, the finding that the level of DAH a country receives is positively associated with its governance level does not apply to countries with high arsenic incidence; for these countries, having good governance is not enough to secure DAH funding and they may need more. In this regard, this study argues that, for the DAH funding to be effectively channeled to the arsenic sector, these countries may need to focus on improving coordination between various stakeholders, including government ministries. This is because arsenic inherently requires an inter-ministerial approach in countries that originally viewed it an environmental problem but now consider its impact on humans a public health issue, for which coordination is often easier said than done. Focusing on Cambodia, the next section discusses the challenges and possible ways forward in such circumstances.
5. The Cambodian case
In the flat and densely populated area around the Mekong River in Cambodia, the arsenic-contaminated groundwater has not been properly treated. This water is often used for drinking water via wells, and even where it is not, it is used for agricultural purposes, such as rice cultivation. As shown in the map below (), high concentrations of arsenic have been detected in the groundwater in the Mekong River basin (represented by the shaded areas, which have been denoted ‘At Risk’). This phenomenon can also be observed in , which demonstrates that in the Kandal and Kampong Cham areas, the proportion of wells with arsenic levels of 50μg/L or more is quite high (Ratha et al. Citation2017), with Kandal being more severely affected. In fact, estimates indicate that approximately 2.4 million people have been exposed to such groundwater (Shaji et al. Citation2021). Arsenic-contaminated food and water pose a greater threat than manganese, cadmium, and lead, and past studies have strongly emphasized the negative impacts of arsenic on public and community health (Murphy et al. Citation2021; Phan et al. Citation2016; Pravalprukskul, Aung, and Wichelns Citation2018; Ratha et al. Citation2017), highlighting the linkages between arsenic toxicity and the immune system deterioration (Bellamri et al. Citation2018).
Figure 1. Arsenic risk areas in Cambodia. Source: Ratha et al. (Citation2017).
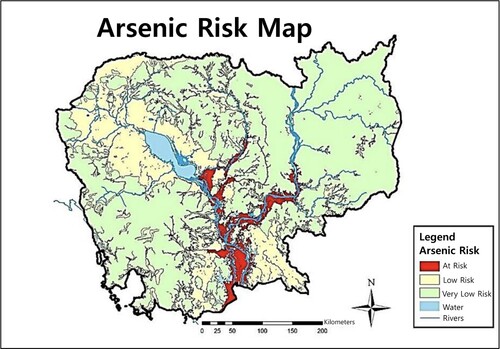
Table 4. Testing results in affected provinces.
Recognizing this risk, Cambodia has implemented national-level programs to address arsenic issues. For example, the National Action Plan on Rural Water Supply and Sanitation Phase 2 (2019–2023) aims to extend access to clean water to 90 percent of the country (including rural areas) by 2023 (Phnom Penh Post Citation2022). Additionally, The National Strategy for Rural Water Supply, Sanitation and Hygiene (2011–2025) has set the ambitious goal of achieving 100 percent coverage of rural sanitation services by 2025 (World Bank Citation2020).
In 2002, The Cambodian government established the Arsenic Inter-ministerial Sub Committee (AISC), which comprises five relevant ministries: the Ministry of Rural Development (MRD), the Ministry of Water Resource and Meteorology (MOWRAM), the Ministry of Health (MoH), the Ministry of Mines and Energy (MIME), and the Ministry of Environment (MoE). As shown in , the MRD chairs the AISC alongside two major departments – the Department of Rural Water Supply (DRWS) and the Department of Rural Health Care (DRHC) (MRD Citation2011).
Figure 2. Structure of the Arsenic Inter-Ministerial Sub Committee (AISC). Source: (MRD 2011).
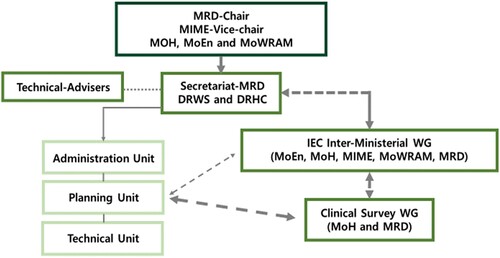
The fact that the committee includes a variety of ministries bespeaks the widespread recognition that effective arsenic mitigation inherently requires an inter-disciplinary approach involving careful coordination among these ministries. Unfortunately, that is not the case for the AISC; the MRD, the chairing ministry, does not have a strong drive to serve as a control tower, given that the main two departments in the MRD handling the committee lack budget, personnel, and decision-making power.Footnote7
From a broader perspective, coordination between the Cambodian government and the international community (international organizations, bilateral development agencies, NGOs, etc.) and among these entities is arguably even more challenging. Indeed, the fact that the latest MDGs and SDGs emphasize their partnership – namely, harmonization or coordination among aid donors – reflects this hardship. In Cambodia, incoherence and hierarchy exacerbated by fragmentation pose fundamental challenges to inter-agency collaboration, hampering so-called Delivery as One (DaO) (Melle and Cappellaro Citation2018).
Moreover, although several projects have been implemented in Cambodia, the country has yet to reach the level of action necessary to address the arsenic problem, which is mostly concentrated in South Asian regions with Bangladesh as the hub (Hossain Citation2006; Murphy et al. Citation2021). This situation is truly an obstacle for Cambodia in terms of coordinating with and achieving solidarity from international organizations regarding the urgency of the arsenic problem.Footnote8
6. Conclusion and discussions
To sustain its arsenic mitigation funding, Cambodia must identify a best-fit model for the specific arsenic contamination case it faces. Rouhi, Gorji, and Maleki (Citation2019) explored eight coordination models that could be used to manage natural disasters, and Cambodia could adopt such a model to address its dangerous arsenic contamination.
First, the MRD-focused AISC must be reformed. Since arsenic contamination is a major environmental problem that significantly impacts people’s health, either the Ministry of Environment or the Ministry of Health should replace the MRD as the control tower. Meanwhile, the Ministry of Education should spearhead efforts to raise public awareness about the arsenic problem, while the Ministry of the Interior – generally tasked with collaborating with provinces – should facilitate communication among each local provinces. The establishment of a cooperative model with health- and/or environment-related international organizations and university research institutions is also crucial. Although several laboratories have the capacity to conduct arsenic studies (Research Development International, Institute of Technology of Cambodia, Royal University of Phnom Penh, University of Health Sciences, International University, Ministry of Commerce, Ministry of Industry, Science, Technology & Innovation and Ministry of Environment), most of them lack stable electrical service, face budget constraints, and do not cooperate among themselves. Most importantly, given the top-down nature of the country’s decision-making process, it is of the utmost importance that the Prime Minister’s office makes tackling this problem a focal point – to use a game-theory term – around which (among several possible options) coordination becomes a self-fulfilling belief (Basu Citation2018).
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 Awareness, locally and globally, regarding the danger of arsenic is still quite low. Without targeted public awareness campaigns, arsenic remains an abstract and remote concept for many people, particularly for those with less education. The WHO’s threshold for defining arsenic contamination in ground water is 10 ug/L (micrograms per liter) or 10 ppb, but the threshold is set much higher in Cambodia at 50 ug/L (WHO Citation2023).
2 This variable plays a key role in this paper, serving as a bridge between the first part of the empirical analyses with the second part of the Cambodian case.
3 The DAH data covers 173 developing countries and the WDI covers over 200. However, the data of only 122 countries is included in both sources over this study’s entire time span. Additionally, the DAH dataset only includes data through 2020.
4 Afghanistan, Algeria, Armenia, Azerbaijan, Bangladesh, Bolivia, Botswana, Burkina Faso, Cambodia, Cameroon, Costa Rica, China, Cuba, Dominica, Ecuador, El Salvador, Egypt, Ethiopia, Ghana, Honduras, India, Indonesia, Jamaica, Kenya, Kyrgyzstan, Laos, Libya, Malawi, Malaysia, Mexico, Mongolia, Morocco, Myanmar, Namibia, Nepal, Nicaragua, Niger, Nigeria, Pakistan, Papua New Guinea, Paraguay, Philippines, Peru, South Africa, Sri Lanka, Tajikistan, Tanzania, Thailand, Togo, Turkmenistan, Uganda, Uzbekistan, Vietnam, and Zambia. A continuous variable would have been more desirable, but data are unavailable.
5 Given the relatively lower number of zero values, we conduct panel fixed effect analyses as a robustness check. These analyses generate results that are the same as those shown in , with a lower significance level and an omitted finding for the arsenic dummy variable, due to its time-invariant nature. They can be provided upon request.
6 Given that the coefficients vary from 0.116 to 0.199, Exp (0.116) = 1.12 and Exp(0.199) = 1.22.
7 This is based on interviews with the Director and his team in the Department of Rural Water Supply of the Ministry of Rural Development. (11 November 2022) in Phnom Penh, Cambodia. The director and his department oversee the AISC.
8 After visiting ADB, WFP, and UNESCO in July 2022, the authors confirmed that no current projects tackle arsenic problems. In the ADB Cambodia office, actions to address arsenic problems have been stalled since 2009. This is the case even though the Country Director is fully cognizant of arsenic issues. While experts at WFP claim that problems such as food poisoning may occur when arsenic is present in rice cultivation, none of their projects seek to address the issue. Additionally, experts at UNESCO do not conduct any educational programs to raise public awareness about the arsenic problem.
References
- Ahmad, Y., and E. Carey. 2021. “Development Co-Operation During the COVID-19 Pandemic: An Analysis of 2020 Figures and 2021 Trends to Watch.” In Development Co-Operation Profiles. Paris: OECD Publishing. https://doi.org/10.1787/e4b3142a-en.
- Alesina, Alberto, and David Dollar. 2000. “Who Gives Foreign Aid to Whom and Why?” Journal of Economic Growth 5 (1): 33–63. https://doi.org/10.1023/A:1009874203400.
- Basu, Kaushik. 2018. The Republic of Beliefs: A New Approach to Law and Economics. Princeton University Press. https://doi.org/10.1515/9781400889358.
- Bellamri, N., C. Morzadec, O. Fardel, and L. Vernhet. 2018. “Arsenic and the Immune System.” Current Opinion in Toxicology 10:60–68. https://doi.org/10.1016/j.cotox.2018.01.003.
- Berthélemy, Jean-Claude, and Ariane Tichit. 2004. “Bilateral Donors’ aid Allocation Decisions: A Three-Dimensional Panel Analysis.” International Review of Economics & Finance 13 (3): 253–274. https://doi.org/10.1016/j.iref.2003.11.004.
- Burnside, Craig, and David Dollar. 2000. “Aid, Policies, and Growth.” American Economic Review 90 (4): 847–868. https://doi.org/10.1257/aer.90.4.847.
- Gibson, J. M., D. Rigby, D. A. Polya, and N. Russell. 2016. “Discrete Choice Experiments in Developing Countries: Willingness to Pay Versus Willingness to Work.” Environment Resource Economics 65 (4): 697–721. https://doi.org/10.1007/s10640-015-9919-8.
- Hossain, M. F. 2006. “Arsenic Contamination in Bangladesh – An Overview.” Agriculture, Ecosystems & Environment 113 (1–4): 1–16. https://doi.org/10.1016/j.agee.2005.08.034.
- Jones, Samantha, and Punam Khaira. 2014. “A Comparative Analysis of the Effects of Awareness Raising Knowledge of the Problems Associated with Arsenic-Contaminated Tube Well Water in Three Cambodian Villages.” Population, Space, and Place 20 (8): 709–727. https://doi.org/10.1002/psp.1808.
- Kim, E., and J. Oh. 2012. “Determinants of Foreign Aid: The Case of South Korea.” Journal of East Asian Studies 12 (2): 251–274. https://doi.org/10.1017/S1598240800007852.
- Lane, Christopher, and Amanda Glassman. 2007. “Bigger and Better? Scaling Up and Innovation in Health Aid.” Health Affairs 26 (4): 935–948. https://doi.org/10.1377/hlthaff.26.4.935.
- Li, Er, Xiangying Zeng, and Yuehua Fan. 2008. “Air-water Ratio as a Characteristic Criterion for Fine Bubble Diffused Aeration Systems.” Chemical Engineering Journal 137 (2): 214–224. https://doi.org/10.1016/j.cej.2007.04.023.
- Lim, Stephen S, Theo Vos, Abraham D Flaxman, Goodarz Danaei, Kenji Shibuya, Heather Adair-Rohani, Mohammad A. AlMazroa, et al. 2012. “A Comparative Risk Assessment of Burden of Disease and Injury Attributable to 67 Risk Factors and Risk Factor Clusters in 21 Regions, 1990–2010: A Systematic Analysis for the Global Burden of Disease Study 2010.” The Lancet 380 (9859): 2224–2260. https://doi.org/10.1016/S0140-6736(12)61766-8.
- McKinlay, R. D., and R. Little. 1977. “A Foreign Policy Model of U.S Bilateral Aid Allocation.” World Politics 30 (1): 58–86. https://doi.org/10.2307/2010075.
- Melle, Valentina, and Giulia Cappellaro. 2018. “Cross-level Coordination Among International Organizations: Dilemmas and Practices.” Public Administration 96 (4): 736–752. https://doi.org/10.1111/padm.12525.
- Ministry of Rural Development (MRD). 2011. National Strategy for Rural Water Supply, Sanitation, and Hygiene 2011-2025. http://cdc-crdb.gov.kh/en/twg-jmi/sector_strategy/mrd_b_rssw_straigy_Eng.pdf.
- Murphy, Thomas, Kongkea Phan, Kim Neil Irvine, and David Lean. 2021. “The Role of Micronutrients and Toxic Metals in the Management of Epidemics in Cambodia.” International Journal of Environmental Research and Public Health 18 (21): 11446. https://doi.org/10.3390/ijerph182111446.
- OECD. 2023. Aid (ODA) by Sector and Donor [DAC 5]. OECD CRS. https://stats.oecd.org/Index.aspx?DataSetCode=crs1#.
- Oh, Jinhwan, and Yoon Jeong Kim. 2015. “Proliferation and Fragmentation: Uphill Struggle of Aid Effectiveness.” Journal of Development Effectiveness 7 (2): 192–209. https://doi.org/10.1080/19439342.2014.983537.
- Petrusevski, B., S. Sharma, W. G. van der Meer, F. Kruis, M. Khan, M. Barua, and J. C. Schippers. 2008. “Four Years of Development and Field-Testing of IHE Arsenic Removal Family Filter in Rural Bangladesh.” Water Science and Technology 58 (1): 53–58. https://doi.org/10.2166/wst.2008.335.
- Phan, K., K. W. Kim, L. Huoy, S. Phan, S. Se, A. G. Capon, and J. H. Hashim. 2016. “Current Status of Arsenic Exposure and Social Implication in the Mekong River Basin of Cambodia.” Environmental Geochemistry and Health 38 (3): 763–772. https://doi.org/10.1007/s10653-015-9759-z.
- Phnom Penh Post. 2022. “100% Access to Clean Water Nationwide by 2025.” Accessed July 5, 2023. https://www.phnompenhpost.com/national/100-access-clean-water-nationwide-2025.
- Piva, Paolo, and Rebecca Dodd. 2009. “Where Did All the Aid Go? An In-Depth Analysis of Increased Health Aid Flows Over the Past 10 Years.” Bull World Health Organization 87 (12): 930–939. https://doi.org/10.2471/BLT.08.058677.
- Pravalprukskul, P., May Thazin Aung, and Dennis Wichelns. 2018. Arsenic in Rice: State of Knowledge and Perceptions in Cambodia. Stockholm: Stockholm Environment Institute.
- Ratha, P., K. D. W. Nandalal, H. M. T. G. A. Pitawala, H. A. Dharmagunawardhane, and S. B. Weerakoon. 2017. “Arsenic Contamination in Cambodia: A Status Review.” In Proceedings of the 2nd International Symposium on Conservation and Management of Tropical Lakes, Siem Reap, Cambodia. 24–26.
- Ravishankar, Nirmala, Paul Gubbins, Rebecca J Cooley, Katherine Leach-Kemon, Catherine M Michaud, Dean T Jamison, and Christopher J. L. Murray. 2009. “Financing of Global Health: Tracking Development Assistance to Health from 1990 to 2007.” The Lancet 373 (9681): 2113–2124. https://doi.org/10.1016/S0140-6736(09)60881-3.
- Rouhi, N., H. Gorji, and M. Maleki. 2019. “Nongovernmental Organizations Coordination Models in Natural Hazards: A Systematic Review.” Journal of Education and Health Promotion 8:44.
- Shaji, E., M. Santosh, K. V. Sarath, P. Prakash, V. Deepchand, and B. V. Divya. 2021. “Arsenic Contamination of Groundwater: A Global Synopsis with Focus on the Indian Peninsula.” Geoscience Frontiers 12 (3): 101079. https://doi.org/10.1016/j.gsf.2020.08.015.
- UNICEF. 2019. Policy Brief: Mitigating Arsenic in Drinking Water.
- WHO. 2005. Health and the Millennium Development Goals. World Health Organization.
- WHO. 2023. WHO Fact Sheets. World Health Organization. https://www.who.int/news-room/fact-sheets/detail/arsenic.
- World Bank. 2020. “Strengthening Institutions to Bring Water and Sanitation Services to Cambodia’s Rural Areas.” The World Bank Results Brief.
- World Bank. 2023. World Development Indicator. Accessed June 30, 2023. https://databank.worldbank.org/source/world-development-indicators.