
ABSTRACT
Community-based projects place emphasis on a collaborative approach and facilitate research among Indigenous populations regarding local issues and challenges, such as traditional foods consumption, climate change and health safety. Country foods (locally harvested fish, game birds, land animals and plants), which contribute to improved food security, can also be a primary route of contaminant exposure among populations in remote regions. A community-based project was launched in the Dehcho and Sahtù regions of the Northwest Territories (Canada) to: 1) assess contaminants exposure and nutrition status; 2) investigate the role of country food on nutrient and contaminant levels and 3) understand the determinants of message perception on this issue. Consultation with community members, leadership, local partners and researchers was essential to refine the design of the project and implement it in a culturally relevant way. This article details the design of a community-based biomonitoring study that investigates country food use, contaminant exposure and nutritional status in Canadian subarctic First Nations in the Dehcho and Sahtù regions. Results will support environmental health policies in the future for these communities. The project was designed to explore the risks and benefits of country foods and to inform the development of public health strategies.
Introduction
Contaminant exposure assessment provides key insights on the environmental determinants of health at local, regional, national and global levels. Biomonitoring measures human exposure to chemical substances using biological samples [Citation1]. Biomonitoring projects have shown that contaminant and nutrient exposure is spatially and temporally dependent [Citation2]. It can be influenced by both natural and anthropogenic factors that affect air and water quality, as well as the integrity of locally harvested food sources.
In remote subarctic Indigenous (First Nations, Métis and Inuit) communities of the Northwest Territories (NTs), Canada, the ongoing reliance on country foods (ie locally harvested land mammals, fish, birds and plants) is associated with improved nutrition, food security and lower rates of chronic disease [Citation3–Citation5]. Country foods in some Dene communities were previously estimated to provide up to 32% of the daily energy of adults, mainly through the frequent consumption of some locally harvested land animals (caribou, moose), birds (spruce hen, scoter, ptarmigan) and fish (whitefish, coney, trout, cisco, walleye, pike) [Citation6]. However, elevated fish mercury levels discovered in some lakes of the Mackenzie Valley Basin of the NT prompted the release of a series of food consumption notices that suggested people limit their consumption of predatory fish species, such as walleye, northern pike and lake trout from specific lakes in the region [Citation7]. Mercury is a heavy metal and chronic exposure to its organic complex (methylmercury) is associated with neurotoxicity and developmental toxicity [Citation8,Citation9]. Furthermore, mercury concentrations in fish were observed to increase in this region in recent years [Citation10], and the local population wanted to better understand how to safely consume fish.
To address these concerns, a multi-year community-based biomonitoring project was developed to investigate current levels of contaminant exposure among participating First Nations communities of the Canadian subarctic in the NTs.
A community-based approach is dependant on the engagement of the community, and defined as those who are affected by the health issue, and also every group with a specific culture that can take the lead in engagement efforts and engage in joint action in a geographical location [Citation11–Citation13]. Community-based projects in the NTs usually focus on environmental monitoring (eg wildlife, contaminants, climate change) or Traditional Knowledge (TK) preservation [Citation14–Citation20]. Community-based approaches facilitate health programme implementation among Indigenous populations [Citation21], and are critical for the success of environmental health projects among Northern Indigenous populations [Citation22]. The involvement of Elders and local leaders is particularly important in the development of culturally relevant environmental health projects among such populations [Citation23]. As per the four critical elements of community-based projects [Citation24], communities (agents in a specific locality) were included as: i) the setting location, ii) the target group which experiences the health issue, iii) the agent vector and iv) the resource to create and implement the project.
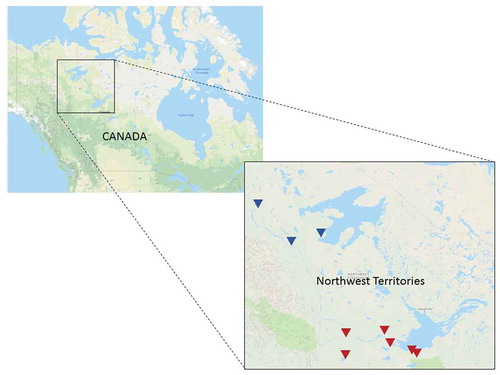
The geographic scope of this study included First Nations communities in the Dehcho and Sahtú regions of the NTs. There are a series of existing environmental monitoring programmes active in these regions, such as the Aboriginal Aquatic Resource and Oceans Management (AAROM) [Citation25] programme helping Indigenous groups to participate in decision-making processes by capacity building and collaborative management and the Sahtù Environment Research and Monitoring (SERM) programme [Citation26], developing regional strategies to manage the land wisely and with respect to the local culture. The residents of communities within these regions are predominantly South Slavey and North Slavey Dene. Specifically, in these regions, more than 77% of residents are Indigenous [Citation27]. In collaboration with regional partners, the University research members contacted 13 Dene and Métis communities (Deh Gah Gotie, Liidlii Kue, West Point, Jean Marie River, Ka’a’gee Tu, Sambaa Ke, Pehdzeh Ki, Katlodeeche, Colville Lake, Déline, K’asho Got’ine, Norman Wells, and Tulít’a) to discuss the project. These communities collectively represent 19% of Indigenous residents of the NTs [Citation27]. Of the communities approached, nine accepted to participate in the biomonitoring project (see ).
Figure 1. Northwest territories communities participating in the biomonitoring project in the Sahtú region (▼) and Dehcho region (▼).
The biomonitoring investigation discussed herein, which was designed in close collaboration with community leaders from participating First Nations of the Mackenzie Valley, included sampling of human hair, urine and blood, as well as the administration of three questionnaires. The methods and approaches taken in preparation, implementation and reporting of human biomonitoring research were adapted according to the unique regional and cultural characteristics of participating First Nations communities. The design of this community-based biomonitoring project, as well as the approaches taken to develop these procedures, is presented below. In addition to the local leadership, partners and local collaborators, an interdisciplinary team was assembled to assist the project, including experts in community-based research, human toxicology, ecotoxicology, exposure assessment, Indigenous environmental health, biology, human nutrition, lipidomics, epidemiology, risk perception and communication, and food security.
Community-based research process
Funding and proposal
The Dehcho First Nations (AAROM’s programme manager) contacted the principal investigator’s team in 2014 to get support to characterise the heath issue related to mercury advisories in the region. This was the first step of collaboration, leading to the development of the backbone of the biomonitoring project. Consultation within the region started before proposal submission, and included participation in local workshops, and the development of potential collaboration with local partners. Collaborators within the Dehcho (AAROM programme) conducted an environmental health survey that profiled participants’ perspectives on the effect of advisories on fish consumption, interest in participating in a biomonitoring study and interest in receiving additional information related to country foods. Results of the survey provided information required to build the foundation of the community-based biomonitoring project in the Dehcho First Nations communities.
Community consultations
Given the time and care needed to foster meaningful relationships with local community leaders, public consultation and dialogues for the research began in 2014, approximately 2 years prior to collection of the first samples. Substantial differences among communities, in terms of population size, governance structures and capacity, meant that the length of the consultation period varied considerably from one community to another. Consultations helped ensure that community needs and priorities were being met through the research, and that the purpose and scope of the project were well characterised, and a confirmation from all parties of the process moving forward. The research team initiated collaborative knowledge exchanges and public consultations at least 6 months (and up to 24 months depending on community) prior to commencing the contaminant biomonitoring study in any given community. In addition to frequent teleconference and email conversations, the research team met at least twice with community leaders in person in the community before implementing the project. Within each participating community, face-to-face meetings with community leaders (including Chiefs, presidents of local councils, senior administrators and resource managers) as well as at least one public meeting took place. When the opportunity was presented, the research team introduced the project to community leaders during council meetings. This consultation period was the first step in an ongoing process to solidify relationships and contextualise the relevance and importance of the project for participating communities.
Through these consultation efforts, communities shared information regarding local history, specific contaminant issues and sensitive topics that should not be included within the project (eg genetic testing). We received comments on community members’ expectations for how the results should be returned and sought feedback on the ways by which, at the end of the project, culturally appropriate sample destruction could be accomplished. A key outcome from these community meetings was that the right-to-know for each individual had to be respected; all results should be returned to each participant, even if they were difficult to interpret from a health risk perspective.
Agreements
Throughout this process, the research team worked closely with community leaders to develop a Community Research Agreement (CRA) for each participating community. The CRA clarified the responsibilities and expectations of the research team and each participating community, defined the scope of the work, articulated the expected benefits and outcomes of the study, stated principles of informed consent and proposed a data management plan. The Chief from the pilot community (the first community to participate) provided critical advice for several aspects of the CRA, including translation of documents, potential sampling dates, important training material for hiring of local research coordinators and design of a protocol for the destruction of hair samples in a culturally appropriate manner. This process was carefully outlined to respect the rights of First Nations communities to own, control, access and possess information (OCAP®) about their peoples and comply with all aspects of the principles of First Nations data collection, protection, use and sharing [Citation28]. OCAP® are principles established to properly conduct research with First Nations and provides standards to insure they remain stewards of their information. The principles of OCAP® were incorporated into the design and implementation of the study described herein. Expressed written consent of the leaders from participating First Nations is required prior to the dissemination of project results via publication or media contact. Memoranda of understanding were also developed to outline financial agreements between the research group and all participating communities, as well as between researchers and local health centres, for the hiring of registered nurses. Partnerships with regional health authorities enabled the research team to hire registered nurses who were responsible for the collection of blood samples over the course of the study.
Research and ethics licences
In preparation for the project, the research team received ethics clearance for the design and methods, and then annual ethics approval for each subsequent year of the project. Ethics and licensing reviews were conducted by the University of Waterloo Research Ethics Committee, the Stanton Territorial Health Authority (STHA) for Human Research and the Aurora Research Institute. Health Canada ethics approval was also obtained regarding additional analysis of the biobanked samples that were placed in a long-term archive.
Preparation of communities
Training of local coordinators
Project funds supported the hiring of local research coordinators, each of whom signed a Confidentiality Agreement to protect the personal information of participants. Depending on the size of the community, 1–2 local research coordinators were hired to assist with logistics, participant recruitment and survey administration during the study. All local coordinators participated in a 3-h training programme (via teleconference or video conference) that provided an overview of the project, pertinent information regarding confidentiality, the process of random recruitment selection and lastly the recruitment procedure. In addition, each coordinator completed 3 h of onsite field training to familiarise themselves with the procedures for hair and urine sample collection, as well as the administration of the surveys and questionnaires. The coordinator’s role included describing the informed consent process to each participant, and assisting with the implementation of the project by overseeing participant recruitment and facilitating completion of the clinical component with participants. During the biomonitoring clinic, the coordinators were responsible for assisting the researchers in explaining the various components of the study and verifying consent from participants, collecting samples of hair for chemical analysis, assisting in the shipping process and supporting participants in the completion of the electronic surveys.
Incorporating local knowledge
TK is defined by the United Nations Educational, Scientific and Cultural Organization (UNESCO) as the Knowledge, innovations and practices of Indigenous and local communities around the world [Citation29]. In addition, the Assembly of First Nations mentions that it is a collective knowledge unique to Indigenous communities, which includes food preparation and beliefs [Citation30]. TK was integrated within several components of the contaminants biomonitoring study. Local perspectives provided by residents of the Dehcho and Sahtú regions during community consultations helped to ensure that the mission and design of this research addressed the priorities and concerns of Indigenous people of the NTs, respecting local beliefs. For example, the method for hair incineration following the project’s completion was modified to reflect local cultural and spiritual beliefs. Furthermore, the study incorporated the knowledge of local harvesters and hunters in the development of the dietary surveys. This local knowledge was crucial to ensure that the questionnaires used locally relevant terms to describe country foods, and that those foods could be recognised by individuals in participating communities. Other important facets of local knowledge that were incorporated within the dietary questionnaire included the seasonality of foods, the availability and consumption of the types of food specific to each community, and the methods by which food is often prepared. The research team will continue to explore the ways by which TK can be incorporated into the creation and dissemination of project results.
Language and its role in defining and understanding concepts played a prominent role in the design of the study. Terminology workshops with Elders and local leaders were organised in collaboration with the Sahtú Renewable Resources Board, helping to clarify conceptual differences in language and the meaning of words between researchers and community members from participating communities. For example, this process illustrated that the term contaminant was sometimes conceptualised and translated into a substance that kills. Such a provocative definition had the potential to inflame anxieties and was inappropriate for use within biomonitoring research. As such, in collaboration with Elders and local language experts, options for how to translate each of the identified terms of interest were discussed, and the group arrived at a new translation for several words. Through the terminology workshop, contaminant became: substance that got into it [another] (Ası̨́ı̨́ beta ɂajá). Time was spent during the terminology workshop to work through more meaningful and accurate translations for several words used in the biomonitoring project.
Project components and implementation
The biomonitoring project included biological sample collection (hair, urine and blood), a pair of dietary surveys evaluating food usage patterns, and a health messages survey assessing participants’ awareness and perceptions of contaminant issues. An overview of each of these six components is described in .
Table 1. The components of the data collected.
Pilot community
As per the recommendation of the First Nations Biomonitoring Initiative [Citation31], before delivering the project across the Dehcho and Sahtú regions, the research team conducted a pilot study, including the sample collection clinic, in one of the participating communities. This was done to refine the project tools and logistics. The pilot community was chosen according to the initiative and interest of community members as well as Chief Gladys Norwegian’s (Jean Marie River First Nation, NT) strong support for the project. This pilot project helped to ensure that the project design was relevant to community needs and context, verify the recruitment process, establish an expected participation rate and refine the project logistics (eg transportation of equipment and samples). The pilot community also provided direction to the return of results strategy.
Questionnaires used in the project were previously validated during a focus group with community members. Focus groups were held with local harvesters to ensure that the foods included in the questionnaire were relevant to the region and referred to foods using names that participants would recognise. Additionally, the food frequency survey was validated through an open community forum as well as through a test/re-test approach.
Communication
Communications with collaborators and partners
The research team provided project partners (including the Government of the Northwest Territories Department of Health and Social Services (DHSS), Northwest Territories Regional Contaminants Committee, Northwest Territories Health and Social Services Authority (NTHSSA) for the Dehcho and Sahtú regions, AAROM, and the Sahtú Renewable Resources Board (SRRB)) with periodic updates by phone or email. In addition, the research team regularly participated in the Sahtú Environmental Research and Monitoring Forum, providing further opportunities for the research team to liaise with community delegates and other researchers working in the Sahtú Region.
Communication with participants and communities
Community leaders continue to receive a seasonal newsletter and bi-monthly updates by phone or email of the study’s progress within the NTs. The communication strategy with participants was adopted to reassure participants of the commitment, accessibility and presence of the research team in conducting the contaminants biomonitoring study, and to recognise the importance of participant and community involvement in this research. This strategy also served to foster long-term trust and meaningful relationships with participating communities. Handwritten post cards were sent between data collection and the returning of the results to thank participants and outlined when results would be communicated. Additionally, social media accounts were created to enhance the impact and visibility of the study in participating communities, and to improve its accessibility to study participants. Furthermore, social media became an important avenue by which the research team was contacted to conduct interviews with local media (eg local newspapers, radio). Social media has previously been identified as a means of increasing the impact and the accessibility of research for participants, including participants living in Indigenous communities [Citation32,Citation33].
The return of results
Principles guiding the return of results were established through direct consultation with participating communities and project partners. These principles included: i) all participants receive their own individual results and ii) all participating communities would receive their community-specific, aggregate results. Although emphasising the “right-to-know” can be challenging (ie for its potential to lead to misunderstandings and/or counter-productive interventions as the health implication is sometime unclear) [Citation34], this approach can help foster more transparent relationships and trust in science and study participants, and can leverage health promotion and increased empowerment [Citation35–Citation37]. Further, community consultations indicated that respect for OCAP® principles would require the project team to return all biomarker results to participants and communities. To guide this process, a Scientific Advisory Committee (including representatives from the office of the Chief Public Health Officer, the Regional Contaminants Committee of the Northwest Territories, and Health Canada) was created in 2016.
This Scientific Advisory Committee assisted with results dissemination by providing input on the: a) design of individual results letters; b) creation of plain-language community reports and c) plans for public results forums in participating communities. In particular, this Committee informed the research team of the establishment and delivery of public health messaging related to contaminant exposure in the NTs. This process helped ensure that this messaging reinforced advice (eg General Fish Consumption Guidelines) previously published by the DHSS. Additionally, the committee provided feedback on the development of factsheets for local clinicians and medical practitioners, providing additional insights on contaminant exposure profiles and guidance values.
Community level
After all analyses were completed and results were prepared for dissemination (approximately 6–10 months after the sampling period), the research team organised a preliminary results phone meeting with community leaders to summarise key messages and findings. These key messages were also provided prior to meetings in the form of community-specific short reports. After the community results forum, a full report was refined according to feedback and concerns from the community, and delivered to community leaders. These reports summarised community-specific results in terms of participant demographics, food intake patterns and biomarker levels. Further, exposure biomarkers were reported for all the compounds analysed and compared with: i) the results from previous studies (Canadian Health Measure Survey, First Nations Biomonitoring Initiative) and ii) health-based tissue guidance values. This information helped establish baseline levels for participating communities, which enables communities to monitor any changes in exposure over time.
Participant level
All study participants who provided a hair, urine and/or blood sample received a confidential, plain-language letter detailing their contaminant exposure profiles. These letters were composed in an effort to: i) provide sufficient context so that the results were meaningful without going into so much detail as to make them overwhelming and ii) emphasise the general healthfulness and importance of country foods. Each participant letter emphasised that levels of exposure above the population average do not necessarily imply that the participant’s health is at risk. Additionally, the letters incorporated several general recommendations on the types of actions individuals can take to lower their exposure to potentially harmful contaminants. With the feedback of participants from the pilot community, the researchers designed a results letter including a colour-coding system to classify the five categories of results describing whether the results exceeded the available guidance values (see Supplemental Information) in order to simplify the information provided in the letter and better communicate results. Additional materials (eg values for comparison) were available on request. On the first page, a preview of the results for three of the most harmful contaminants (ie mercury, cadmium and lead) was expressed both in value, and as a colour-coded system. The letter contained eight pages that included a letter summarising the participant’s results, a table with the participant’s results, recommendations on how to lower personal exposure to contaminants, as well as the General Fish Consumption Guidelines previously published by the Government of the Northwest Territories. The research team provided results letters in person to each participant. In the event that participants were not available while the research team was in the region, the local coordinator was placed in charge of delivering the letter to the participant in the following weeks. Follow-up testing was offered to participants with biomarker levels exceeding health-based guidance values.
Media and scientific results dissemination
After the community meeting was held and participants had received their results, community leaders were asked to provide feedback on their experiences with the communication and return of results. Results were described through the media or scientific presentations only after participants and communities had received their results. Throughout this process, the research team ensured that no mention was made of any individual’s results nor information which could potentially identify a study participant.
Data management and governance
All data collected in the contaminants biomonitoring study are personal and confidential. As such, data management plans have been designed to protect the information of communities and individuals. An electronic password-protected results file was created on an encrypted computer to secure all information considered personal or where potentially identifying characteristics (eg name, age, sex) were recorded. All other documents and samples were coded by a unique participant identification number and do not contain any identifiable information, whether direct or indirect. Participants’ consent forms and data collection sheets are kept in a locked cabinet in a locked room in a secure wing of the School of Public Health and Health Systems at the University of Waterloo.
Each participant has the right to withdraw from the study without loss of remuneration. All samples will be discarded after 10 years through the University of Waterloo’s Environmental Safety Facility. Urine and blood will be incinerated as biological waste. As per the guidelines from the University of Waterloo Research Ethics Board, data will be erased after a period of 25 years. Per a request by community leaders to ensure that the destruction and disposal of human hair samples respects and integrates culturally relevant practices, all human hair will be burned while a prayer from a spiritual leader is recited.
Collaborative future work
Community involvement
The research team continues to pursue opportunities to remain involved and maintain meaningful relationships with the communities that participated in the contaminants biomonitoring study. Annual on-the-land and community research meetings are being used to maintain visibility and impact within the region. Further capacity building opportunities are being explored, including but not limited to: the hiring of community-based social media-savvy young adults in order to maintain lines of communication between the research team and community participants, and training of local research assistants on a field-portable direct mercury analyser to enable community-based, participatory sample collection and data analysis for mercury biomonitoring. This work has been based in the Dehcho and Sahtú regions; however, similar issues and concerns are present in the other regions of the Canadian north. As such, the research team remains committed to working with interested communities to launch this type of work in other parts of the Canadian subarctic and Arctic.
Integration with research being conducted in the Northwest Territories
The contaminants biomonitoring study is complementing a long history of environmental monitoring in the NTs, a trend that is becoming increasingly associated with human health monitoring. Hair, blood and urine sampling [Citation37–Citation41], and country food consumption [Citation42] have been previously assessed in an effort to monitor contaminant exposure in the Canadian North. This study serves to provide a greater understanding of the inherent linkages between country foods, nutritional status, contaminant risk and human health in First Nations communities of the Canadian subarctic. The measurement of contaminants outside of the NCP mandate through the biobank will enable a better understanding of the impacts of contaminant exposure from store-bought foods, in comparison with contaminants found in the environment and in country foods. This study represents one of the first efforts to characterise the perception and awareness of risk from contaminant exposure, and to evaluate the methods of communication most effective in communicating this risk within Indigenous communities of the NTs.
The collaborative work crosses several disciplines and the interdisciplinary research team facilitates better methodological processes addressing the challenges related to community-based research [Citation13]. The co-location of the project with numerous other research projects (eg wildlife and fish contaminant monitoring) is directly supporting our efforts to understand pathways of contaminants exposure, and how social change, climate change, harvest levels and resource development may affect contaminants exposure in the future. Integrating traditionally segregated disciplines, such as aquatic ecology, food choice and human ecotoxicology, is not only consistent with the Indigenous world view that humans are a vital and integral part of natural ecosystems, but is also allowing the research team to explain to communities why some traditional foods have higher levels of contaminants than others. In one community, this has led to a mitigation strategy: intensive fishing is being used to lower fish mercury levels in a lake with particularly high concentrations. In other communities, members of our team explain how contaminants get to remote regions and build up in food chains. This “demystification” of contaminants is contributing to development of mitigation and risk management strategies. Finally, the research team continues to work closely with community leaders and decision-makers at the territorial level to consider how the sociocultural implications of this research can be applied in multiple contexts (eg through global policy, public health advisories, health promotion and finally the dissemination of scientific findings).
Conclusion
The research team will continue working with community and territorial representatives to: 1) ensure that any follow-up biomonitoring continues to address community concerns; 2) identify any potential sources of contaminant exposure and 3) consider practical and efficient approaches by which people can lower their exposure. Country foods provide the people of the NTs with a host of nutritional, economic, social and cultural benefits. Therefore, it is important that messages about contaminants and country foods are carefully designed so as to balance their associated benefits and risks. It was essential for the design of the contaminants biomonitoring study described herein to integrate the sociocultural characteristics of participating communities. The results of this project will report on the links between contaminant exposure, nutritional status and country food use, and will provide important baseline data in this specific region. The outputs of this project will serve to support the development of governance and messaging tools, public health interventions and health policies that maximise the nutritional, cultural and spiritual benefits of traditional food systems while minimising the risks associated with contaminant exposure in Indigenous communities of the NTs.
Ethics approval and consent to participate
Participants provided a free consent. Ethics approval was obtained by the University of Waterloo Research Ethics Committee (#20173, #20950), the Stanton Territorial Health Authority for Human Research (29/12/2015) and the Aurora Research Institute (#15560, #15775, #15966, #15977, #16021) and Health Canada ethics board (REB 2016-0022).
Acknowledgements
The authors acknowledge the funding provided by the Northern Contaminants Program (NCP), which is jointly supported by Indigenous and Northern Affairs Canada and Health Canada. Additional support was received from Global Water Futures (GWF), Northern Scientific Training Program (NSTP) and the University of Waterloo. Supplemental analyses for contaminants outside the NCP mandate were funded by the Population Biomonitoring Section (Healthy Environments and Consumer Safety Branch) of Health Canada. The research team is grateful for assistance from the following organisations: The Government of Northwest Territories Department of Health and Social Services, the Dehcho Aboriginal Aquatic Resources and Ocean Management (AAROM), the Dehcho First Nations (DFN), the Sahtú Renewable Resources Board (SRRB), the Sahtú Secretariat Incorporated (SSI), the Northwest Territories Regional Contaminants Committee (NT RCC), the Sahtú Health and Social Service Authority (SHSSA), the Dehcho Health and Social Service Authority (DHSSA), the Hay River Health and Social Service Authority (HRHSSA), the Centre de Toxicologie du Québec (CTQ), the Institut National de Santé Publique du Québec (INSPQ) and the University of Waterloo. This work represents an ongoing collaboration between researchers at the University of Waterloo (Brian Laird, Heidi Swanson, Mylène Ratelle, Kelly Skinner, Rhona Hanning, Shannon Majowicz, Ken Stark), Trent University (Chris Furgal), University of Montréal (Michèle Bouchard), the Washington State University (Amanda Boyd), the Dehcho Aboriginal Aquatic Resources and Ocean Management (George Low) and the Sahtú Renewable Resources Board (Deborah Simmons). We would like to thank all community leaders, participants and local coordinators in the Dehcho and Sahtú Region for making this work possible.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
Related Research Data
References
- Angerer J, Ewers U, Wilhelm M. Human biomonitoring: state of the art. Int J Hyg Environ Health. 2007;210(3–4):201–10.
- Schulz C, Conrad A, Becker K, et al. Twenty years of the German Environmental Survey (GerES): human biomonitoring – temporal and spatial (West Germany/East Germany) differences in population exposure. Int J Hyg Environ Health. 2007;210(3–4):271–297.
- Council of Canadian Academies (CCA). Aboriginal Food Security in Northern Canada: an Assessment of the State of Knowledge. The Expert Panel on the State of Knowledge of Food Security in Northern Canada, Council of Canadian Academies, Ottawa, ON; 2014.
- Earle L. Traditional aboriginal diets and health. Prince George, BC: National Collaborating Centre for Aboriginal Health (NCCAH); 2011.
- Food and Agriculture Organization. Edited by Kuhnlein HV, Erasmus B, Spigelski D, et al., editors Indigenous Peoples’food systems, well-being interventions and policies for healthy communities. Rome: United Nations Centre for Indigenous Peoples’ Nutrition and Environment; 2013.
- Kuhnlein H, Receveur O. Local cultural animal food contributes high levels of nutrients for Arctic Canadian indigenous adults and children. J Nutr. 2007;137:1110–1114.
- Department of Health and Social Services of the Northwest Territories (DHSS). Site specific fish consumption advice; Accessed on 2017 Jun 15. Available from: http://www.hss.gov.nt.ca/en/services/fish-consumption-guidance/site-specific-fish-consumption-advice
- Zahir F, Rizwi SJ, Haq SK, et al. Low dose mercury toxicity and human health. Environ Toxicol Pharmacol. 2005;20(2):351–360.
- Tchounwou PB, Ayensu WK, Ninashvili N, et al. Review: environmental exposure to mercury and its toxicopathologic implications for public health. Environ Toxicol. 2003;18(3):149–175.
- Chételat J, Amyot M, Arp P, et al. Mercury in freshwater ecosystems of the Canadian Arctic: recent advances on its cycling and fate. Sci Total Environ. 2015;509–510:41–66.
- Agency for Toxic Substances and Disease Registry (ATSDR). Principles of community engagement-second edition, 2011. [Accessed on 2017 Jun 15]. Available from: https://www.atsdr.cdc.gov/communityengagement/pdf/PCE_Report_508_FINAL.pdf
- MacQueen KM, McLellan E, Metzger DS, et al. What is community? An evidence-based definition for participatory public health. Am J Public Health. 2001;91:1929–1938.
- Israel BA, Schulz AJ, Parker EA, et al. Review of community-based research: assessing partnership approaches to improve public health. Annu Rev Public Health. 1998;19:173–202.
- Berkes F, Kislalioglu Berkes M, Fast H. Collaborative integrated management in Canada’s North: the role of local and traditional knowledge and community-based monitoring. Coastal Manag. 2006;35(1):143–162.
- Brook RK, Kutz SJ, Veitch AM, et al. Fostering community-based wildlife health monitoring and research in the Canadian North. Ecohealth. 2009;6(2):266–278.
- Furgal C, Seguin J. Climate change, health, and vulnerability in Canadian Northern aboriginal communities. Environ Health Perspect. 2006;114(12):1964–1970.
- Riedlinger D, Berkes F. Contributions of traditional knowledge to understanding climate change in the Canadian Arctic. Polar Rec. 2001;37:315–328.
- Tremblay M, Furgal C, Larrivée C, et al. Climate change in Northern Quebec: adaptation strategies from community-based research. Arctic Change Coastal Communities. 2008;61(1):27–34.
- Christensen J. Telling stories: exploring research storytelling as a meaningful approach to knowledge mobilization with Indigenous research collaborators and diverse audiences in community‐based participatory research. Can Geographer. 2012;56(2):231–242.
- Armitage DR. Collaborative environmental assessment in the Northwest Territories, Canada. Environ Impact Assess Rev. 2005;25(3):239–258.
- Baydala LT, Worrell S, Fletcher F, et al. Making a place of respect: lessons learned in carrying out consent protocol with first nations elders. Progress Community Health Partnerships: Res Edu Acti. 2013;7(2):135–143.
- Friendship K, Furgal C. The role of Indigenous knowledge in environmental health risk management in Yukon, Canada. Int J Circumpolar Health. 2012;71:19003.
- Varcoe C, Bottorff JL, Carey J, et al. Wisdom and influence of elders: possibilities for health promotion and decreasing tobacco exposure in first nations communities. Can J Public Health. 2010;101(2):154–158.
- McLeroy KR, Norton BL, Kegler MC, et al. Community-based interventions. Am J Public Health. 2003;93(4):529–533.
- Dehcho First Nations (DFO). Aboriginal Aquatic Resource and Oceans Management Program (AAROM); Page consulted online on 2017 Oct 1. Available from: http://www.dfo-mpo.gc.ca/fm-gp/aboriginal-autochtones/aarom-pagrao/index-eng.htm
- Sahtu Renewable Resources Board (SRRB). Programs; Page consulted online on 2017 Oct 1. Available form: http://www.srrb.nt.ca
- Bureau of Statistics, Northwest Territories. Annually calculates July 1 population estimates for every community in the Northwest Territories, estimates cover the 2001 to 2016 period by gender, age group and ethnicity; Page consulted on 2017 Apr 7 Available from: http://www.statsnwt.ca/population/population-estimates/bycommunity.php
- First Nations Information Governance Centre (FNIGC). Ownership, Control, Access and Possession principles (OCAP); Page consulted on 2017 Jun 16. Available from: http://fnigc.ca/ocap.html
- United Nations Educational, Scientific and Cultural Organization (UNESCO). Traditional knowledge; Consulted online on 2018 Jul 3. Available from: http://uis.unesco.org/node/335063
- Assembly of First Nations (AFN). Traditional knowledge; Consulted online on 2018 Jul 3. Available from: https://www.afn.ca/uploads/files/env/ns_-_traditional_knowledge.pdf
- Liang X, Su LYF, Yeo SK, et al. Building buzz: (scientists) communicating science in new media environments. Journal Mass Commun Q. 2014;91(4):772–791.
- Rae K, Weatherall L, Hollebone K, et al. Developing research in partnership with aboriginal communities – strategies for improving recruitment and retention. Rural Remote Health. 2013;13:2255.
- Brody JG, Morello-Frosch R, Brown P, et al. Improving disclosure and consent: “Is it safe?”: new ethics for reporting personal exposures to environmental chemicals. Am J Public Health. 2007;97:1547–1554.
- Brody JG, Dunagan SC, Morello-Frosch R, et al. Reporting individual results for biomonitoring and environmental exposures: lessons learned from environmental communication case studies. Environ Health. 2014;13:40.
- Exley K, Cano N, Aerts D, et al. Communication in a human biomonitoring study: focus group work, public engagement and lessons learnt in 17 European countries. Environ Res. 2015;141(2015):31–41.
- Morello-Frosch R, Brody JG, Brown P, et al. Toxic ignorance and right-to-know in biomonitoring results communication: a survey of scientists and study participants. Environ Health. 2009;8:6–19.
- Butler Walker J, Seddon L, McMullen E, et al. Organochlorine levels in maternal and umbilical cord blood plasma in Arctic Canada. Sci Total Environ. 2003;302:27–52.
- Butler Walker J, Houseman J, Seddon L, et al. Maternal and umbilical cord blood levels of mercury, lead, cadmium, and essential trace elements in Arctic Canada. Environ Res. 2006;100:295–318.
- Curren MS, Liang CL, Davis K, et al. Assessing determinants of maternal blood concentrations for persistent organic pollutants and metals in the eastern and western Canadian Arctic. Sci Total Environ. 2015;527–528:150–158.
- Delormier T, Egeland G, Kandola K, et al. Examining benefits and risks of traditional and market food: hair mercury analysis and communicating research results in the community of Tulita, NWT. Synopsis of Research Conducted under the 2011–2012, Northern Contaminants Program 2012: 58–69.
- Assembly of First Nations (AFN). First Nations Biomonitoring Initiative- National Results (2011); 2013.
- Receveur O, Boulay M, Kuhnlein HV. Decreasing traditional food use affects diet quality for adult dene/metis in 16 communities of the Canadian Northwest Territories. J Nutr. 1997;127(11):2179–2186.