
ABSTRACT
This is the first systematic review to explore health risks on Svalbard. We have analysed data retrieved from 18 articles that met eligibility criteria and present a mixed-methods quantitative and qualitative narrative synthesis. Norwegian and Russian inhabitants on Svalbard were compared with the respective mainland populations, and we found no evidence of an increased risk for or prevalence of diseases. The rate of injuries caused by snowmobile accidents were significantly higher, but this was outweighed by a correspondingly lower rate of other injuries. A small unique risk for injuries inflicted by polar bears was confirmed. We identified knowledge gaps concerning how health care and emergency preparedness are organised.
Introduction
This review addresses health risks and health- and emergency preparedness on Svalbard, the Arctic archipelago at 74° to 81° north latitude, and how Norway and Russia collaborate. Svalbard’s unique location and status entail particular challenges related to long distances, climatic conditions and limited access to healthcare and rescue personnel.
Norway and Russia have been engaged in the coal mining industry on Svalbard for more than a century. For the past decades, mining has declined and tourism and research have become the most important industries. Norway is the sovereign state, but the Svalbard Treaty assigns the signatory countries rights to engage in commercial activities. Norwegian and Russian industries have mostly operated separately with infrastructure and frameworks provided by each country. Today approximately 3000 people live on Svalbard, most in the Norwegian settlement Longyearbyen (approximately 2500 inhabitants) and the Russian settlement Barentsburg (approximately 400 inhabitants). Longyearbyen has evolved from a traditional “company town” organised around mining, into a family community with health and welfare services resembling those on the mainland[Citation1]. An exception is care for the elderly, which is not provided, implying people who need such services must move. Barentsburg is still mainly run by the mining company.
Existing knowledge
Several previous studies conclude that healthcare in remote areas is challenged by factors such as remoteness to advanced health facilities, lack of professional health workers, and inadequate infrastructure [Citation2–4]. Some studies looking into health in small Island communities have found that complications related to inbreeding may be applicable due to a reduced gene pool in such communities [Citation4,Citation5]. This is, however, doubtfully the case on Svalbard, which has a fluctuous population pattern with an average period of living of 6 years.
Further, previous studies imply that there is a slightly increased risk for disease in circumpolar areas, such as psychological effects of long periods of isolation and extreme physical environment and potential negative effects of environmental contaminants among certain population groups in the Arctic [Citation6,Citation7]. The latter is linked with a significant consumption of carnivores on top of the food chain such as seal, whale and different fish species, typical traditional food among indigenous groups in the Arctic. This is nevertheless probably not applicable for Svalbard, as there is no indigenous population on the archipelago and where most of the food is imported.
Regarding accidents, a few studies from other Arctic areas, amongst others Canada and Finland, implies that snowmobile accidents are among the health challenges in Northern Canada and Lapland [Citation8,Citation9]. Further, there are studies from Greenland and Canada that show that mining workers struggle with specific health challenges, such as back injuries and lesions [Citation10,Citation11]. These challenges are probably applicable also for Svalbard, where the number of snowmobiles exceeds the number of inhabitants, and where a significant share of the workforce have been employed in the coal mining industry.
In circumpolar areas (Svalbard included), remoteness to advanced health facilities and limited resources in terms of health personnel and infrastructure indirectly constitute the most significant health threats[Citation2].
Some studies have looked into cooperation between circumpolar states concerning health challenges. Such cooperation has, for instance, taken place between Alaska and Russia in fields such as emergency medicine, mental health and dental treatment [Citation12–14]. In general, a rising awareness of similarities among Arctic actors has made pan-Arctic cooperation, also in health and emergency preparedness, possible through the development of international bodies such as the Arctic Council [Citation15,Citation16].
Studies that look into health challenges on Svalbard in particular have also been published, but this evidence has not been reviewed and synthesised. Covering this knowledge gap, as this study aims at contributing to, is thus considered prudent. A systematic review of health risks and health- and emergency preparedness cooperation between Norway and Russia is therefore warranted.
Methods
Research question, aims and objectives
The overall research question is: What are the health risks and how is the healthcare and emergency preparedness system on Svalbard organised to address these risks? The specific aims were: 1) to identify the risks in terms of healthcare delivery and emergency preparedness, 2) to assess how the healthcare and emergency preparedness system is organised to address these risks, and 3) to study cooperation in healthcare and emergency preparedness between Norway and Russia.
Protocol
Our protocol adhered to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA)[Citation17].
Definitions
The term “Russia” refers to the Russian federation and the Soviet Union, and “Russians” to their populations. The terms healthcare and emergency preparedness are linked because healthcare is an element in emergency preparedness. Healthcare is understood as resources used to cure disease, care for and rehabilitate the ill, and prevent disease. We include trauma in the definition of disease and illness. The term emergency preparedness is used differently, depending on the context, and often interchangeably, along with the terms “emergency response” and “crisis”[Citation18]. We use it to describe actions taken to prevent a crisis, while the term “emergency response” describes concrete actions taken when a crisis is emerging. Search and rescue (SAR) services refer to the immediate actions involving cooperating partners to rescue people from death or injury[Citation16].
Search strategy
A list of relevant search words was developed (). A test search was undertaken to identify the most suitable databases and search word combinations. The databases PubMed, Scopus, CyberLeninka and Web of Science were selected because they produced most relevant articles. The excluded databases either produced few results (Norwegian Open Research Archives and American Bibliography of Slavic and East European Studies), or results that only partially met the inclusion criteria (eLibrary and OpenGrey).
Table 1. Search words and search combinations
The test search also showed that the list of search words was too wide and unspecific. For example, combinations such as “health + north” or “crisis + polar” produced a vast number of articles, very few of which were relevant. The relevant articles were covered by more narrow search word combinations, including the words “Svalbard” or “Spitsbergen”.
shows a complete list of search words grouped into three categories: 1) healthcare, 2) emergency preparedness, and 3) Svalbard. Literature in English, Russian or a Scandinavian language was included. Search words were combined from categories 3 (Svalbard), and 1 (healthcare) or 2 (emergency preparedness).
Eligibility criteria
We included peer-reviewed academic articles that report quantitative or qualitative studies of human health and/or emergency preparedness on Svalbard. Studies of pollutants without direct connection to human health, the surrounding waters and animal health were excluded.
Study selection
shows the selection process. The search retrieved 543 citations. The main author (TAW) screened titles and abstracts for eligibility and excluded 481 citations. 22 duplicates were removed. The remaining 40 citations underwent full-text assessment (TAW), and 23 were removed because they did not fulfil the eligibility criteria. One additional article was included after screening of the reference lists of the assessed articles.
Figure 1. Process figure.
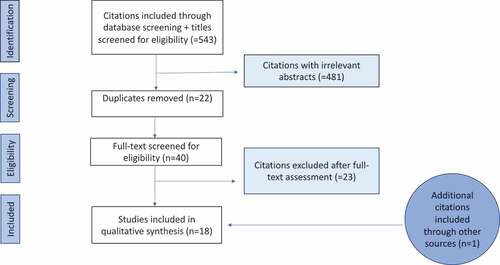
Finally, we included 18 articles published between 1999 and 2017 (median year 2002) for full text review.
Data collection and analysis
Full-text review and data extraction were done independently by the main (TAW) and the co-author (TI). The team included a master-level Russian speaker (TAW), and it had access to consult a native Russian speaker with native proficiency in English. When the reviewers disagreed about ratings of confidence in the findings or data extraction (six articles), consensus was established through discussion.
The key findings were extracted and summarised in the Critical Appraisal Skills Programme (CASP) evaluation table (). We retrieved data into five thematic categories: 1) Diseases, 2) Risk factors for diseases, 3) Traumatic injuries, 4) Search and rescue, and 5) Norwegian-Russian cooperation in healthcare and emergency preparedness. Due to thematic and methodological diversity of the included studies, meta-analysis was not possible, and a narrative synthesis was done.
Table 2. Casp evaluation table
Confidence in findings
We used CASP checklists, Grading of Recommendations, Assessment, Development and Evaluation (GRADE) and Confidence in the Evidence from Reviews of Qualitative research (GRADE-CERQual) to rate the level of confidence in findings.
The CASP checklists were developed to critically appraise the validity, risk of bias, study design, results and implications for practice of single studies [Citation19] The quantitative studies that were included had an observational design and we therefore applied the checklist for cohort studies for these studies. For the qualitative studies, the checklist for qualitative studies was applied.
We used GRADE to rate the confidence of synthesised evidence from quantitative findings. GRADE provides a systematic approach to assess the quality of study designs, risk of bias, imprecision, inconsistency, indirectness, and magnitudes of effects[Citation20]. Confidence in findings from observational studies is initially rated as low and then potentially up- (to moderate or high) or down-rated (to very low).
We used GRADE-CERQual to rate the confidence of synthesised evidence from qualitative findings[Citation21]. GRADE-CERQual provides a systematic approach when assessing study designs, methodological limitations, coherence, adequacy of data, and relevance of the findings. Confidence in findings from quantitative studies is initially rated as high, and then potentially down-rated to moderate, low or very low[Citation22].
Table 3. Evidence profile tables
Table 4. Summary of findings tables
Results
Quality of evidence
GRADE rated the confidence in the quantitative findings in the thematic categories as follows: 1) Diseases: low, 2) Risk factors for diseases: low to very low, and 3) Traumatic injuries: moderate and very low. We used dual ratings in categories 2 and 3 because there was methodological variation within studies. There were no quantitative findings in categories 4 (Search and rescue) and 5 (Norwegian-Russian cooperation in healthcare and emergency preparedness).
GRADE-CERQual rated the confidence in the qualitative findings in the thematic categories 2 (Risk factors for diseases) as very low and 4 (Search and rescue) as high. There were no qualitative findings in categories 1 (Diseases), 3 (Traumatic injuries) and 5 (Norwegian-Russian cooperation in healthcare and emergency preparedness).
Health on Svalbard
Category 1 – Diseases
Three articles reported studies of the prevalence and seasonal variation of middle ear infection, migraine and depression, respectively [Citation23–25]. They showed no indication of increased prevalence among Svalbard compared to mainland Norwegian residents. The study of middle ear infection found no association with climate conditions, and the study of migraine showed no indication of more seasonal variation among Svalbard than Norwegian mainland residents [Citation23,Citation25]. We rated the confidence in the findings as very low because the studies could not control confounders adequately and had no control group on the mainland.
Self-reported depression lasting for more than two weeks over a one-year period was more prevalent among Russians (women 44,7%, men 26,8%) than Norwegians (women 15,6%, men 10,7%)[Citation24]. We rated the confidence in this comparison as very low because the surveys were not done simultaneously, and because economic and political circumstances could have confounded the findings.
Summarised, findings rated at low to very low confidence level indicate that the prevalence of the studied diseases (middle ear infection and migraine) is not different between Svalbard and the mainland, but the prevalence of depression could be higher among Russians than Norwegians.
Category 2 – Risk factors for diseases
Nine articles reported findings from studies of risk factors for diseases or impaired health [Citation26–34].
Two intervention trials studied health outcomes for different shift schedules for Norwegian mine workers and found no differences in outcomes between the regimes [Citation29,Citation30]. We rated confidence in the findings as low because the external validity was limited.
Three observational studies explored temporal patterns in metabolic indices, serum lipid profiles and hospital attendance for health incidents among Russian miners in Barentsburg [Citation26,Citation27,Citation33]. Bojko reported seasonal variation in metabolism, and Bojko and Larsen reported increased serum levels of triglycerides after prolonged (12 months) residence [Citation26,Citation27]. Yenikeev and co-workers observed a temporal association between geomagnetic disturbances and health incidents, mainly traumas and cardiovascular disease[Citation33]. We rated the confidence in these findings as very low because there were substantial flaws in the study designs and failure to control the confounders.
A population-based cross-sectional survey of risk factors for coronary heart disease in the Norwegian population found no difference in risk profiles between Svalbard and mainland residents[Citation32]. We rated the confidence in this finding as low because few data were presented, and no comparative analysis was made accessible.
Another cross-sectional survey of Norwegian residents compared self-reported alcohol consumption with public sales statistics from the only alcohol provider to the Norwegian community[Citation31]. The self-reported consumption accounted for 40% of the sales volume. The study had a moderate response rate (63%), could not control the figures for import or export of alcohol and did not compare the data with a population on the mainland. We rated the confidence in the findings as very low.
One article reported results from a quantitative study of how young people experience and interpret the risk of snowmobile accidents[Citation34]. We rated the confidence in the findings as very low because only a small proportion (10%) of the participants resided on Svalbard, and it was unclear which findings came specifically from these participants.
Summarised, findings rated at low to very low confidence level indicate that living and working on Svalbard is not associated with exposure to particular health risks.
Category 3 – Traumatic injuries
Five articles reported results from studies of traumatic injuries [Citation35–39].
Risholt retrospectively reviewed health records at the Norwegian hospital in Longyearbyen from 1950 to 1989 and recorded 84 (mean 0,5 per year) trauma-related deaths[Citation35]. Before 1970, most occurred in the mining industry, while after 1970 the majority was caused by leisure-related activities. Risholt estimated the risk of being involved in a fatal leisure-related accident nearly three (males) and eighteen (females) times higher than in the comparable population on the mainland. One aviation accident caused the very high risk for females. We rated the confidence in these estimates low because the study did not adjust for age and sex differences between the populations, and low accident frequencies entailed a high risk for random variation for residents on Svalbard.
Risholt also reviewed hospital records and the governor’s files from 1971 to 1995 and verified six non-fatal and four fatal traumas inflicted by polar bears over 24 years[Citation36]. This confirms a small and unique risk of being injured or killed by polar bears.
Ytterstad and co-workers conducted three prospective observational studies of patients treated for injuries at the hospital in Longyearbyen over a five-year period from 1997 [Citation37–39]. The first was a study of all traumatic injuries and compared injury rates on Svalbard with the Harstad region on the Norwegian mainland. The injury rates of 100,9 for men, and 76,3 for women (Svalbard) and 115,4 for men and 80,1 for women (Harstad) per 1000 person-years were not statistically significantly different. The violence rate of 3,1 in Harstad was significantly higher than the rate of 0,9 per 1000 person-years on Svalbard. Home injuries accounted for a larger proportion in Harstad (30.5%) than on Svalbard (22% including visitors), while work- and leisure-related injuries accounted for larger proportions on Svalbard (27.2% and 41.9%) than in Harstad (13.2% and 34.8%). We rated the confidence in the findings for Svalbard residents as moderate and the confidence in the findings from the comparative analyses as very low because the authors did not adjust for the large age and sex differences in the composition of the two populations.
The two subsequent studies reported the number of and injury rates for snowmobile accidents. [Citation37,Citation39]. The studies overlapped and we therefore report findings extracted from the most recent article, which included patients prospectively registered over five years[Citation37]. 181 injured persons were registered. Nine of ten injuries occurred during leisure time. The authors calculated injury rates as the number of injuries per 1000 registered snowmobiles per year, and compared rates for Norwegian residents and visitors (250 snowmobiles were available for visitors to rent). The injury rate was significantly higher for visitors (70,0) than for residents (17,5) per 1000 snowmobiles per year. We rated the confidence in the findings as moderate for Svalbard residents and very low for the comparisons, as the exact number of visitors and duration of visits (i.e. exposure) was unknown.
Summarised, findings from observational cohort studies rated at low to moderate confidence level showed that a gradual shift from predominantly occupational injuries in the mines to leisure-related snowmobile accidents occurred in the 1970s. The studies confirm a small and unique risk of being injured or killed by polar bears. Comparative findings rated as low confidence level showed no difference in overall injury rates between Svalbard and mainland Norway, but indicated a significantly higher risk of being injured in a snowmobile accident for Svalbard residents, and correspondingly a lower risk of being injured in other traffic accidents.
Category 4 – Search and rescue
One article reported findings from a qualitative study of collaboration between volunteers from the local population and professionals during a Norwegian SAR-operation[Citation40]. The case was the avalanche that crushed houses in Longyearbyen in 2015. The study found that the local population was an important resource, that professionals expected volunteers to contribute, and that the collaboration was successful. We rated the confidence in this evidence as high.
Category 5 – Norwegian-Russian cooperation in healthcare and emergency preparedness on Svalbard
None of the articles addressed Norwegian-Russian cooperation in healthcare and emergency preparedness.
Discussion
Summary
This is the first review of health and emergency preparedness against the backdrop of Norwegian–Russian relations on Svalbard. We found no evidence of an increased risk of or presence of risk factors for diseases or other health challenges on Svalbard, except from polar bear attacks. There are, however, significant knowledge gaps. They include lack of evidence about occupational hazards and disease among miners, and about Norwegian-Russian cooperation in health and emergency preparedness.
Health risks on Svalbard
Mining injuries are hardly described in the research literature from Svalbard. However, the lack of descriptions of mining-related injuries is not a proof of their non-existence. They have probably been categorised as “occupational injuries” in the literature. Crush and burn injuries have been reported, indicating that mining-related injuries were common [Citation41,Citation42]. Other Arctic locations, such as Greenland, resemble Svalbard in terms of climatic conditions, population structure, industry and health challenges. In a small Greenlandic mining community, 13% of all medical consultations were due to occupational reasons. Hearing impairment, back pain and lesions of the eyes, hands and wrists were most frequent. This is comparable to data from the Swedish mining industry[Citation43].
Respiratory diseases such as chronic bronchitis, pneumoconiosis and silicosis are severe outcomes related to coal dust exposure in mine workers, and studies show that up to 12% of coal miners develop these serious diseases[Citation44]. One study found that between 2% and 12% of miners exposed to 2 mg/m3 of dust were expected to have pneumoconiosis after 40 years[Citation45]. This review has not detected research literature describing respiratory diseases among mine workers. There are, however, observations of pneumoconiosis and silicosis among miners in other reports, such as a report by a Norwegian mining company clinician from 1984, where 12–15 cases of pneumoconiosis/silicosis were described[Citation42].
The healthy worker effect is a form of bias caused by selection of workers who were initially healthy enough to be hired, whereas the general population include persons unfit for work[Citation46]. Such selection is likely to occur both when employers hire staff for work on Svalbard, and subsequently, as specialised health care, care for the elderly and social services are unavailable. This force residents to return to the mainland when they need such services.
The healthy worker effect could confound observational studies and under-estimate health risks. Accordingly, we cannot preclude that risks not identified by the present review exist.
In accordance, few of the deaths occurring on Svalbard are caused by disease. Instead, most of the few deaths are trauma-related, as shown in the observational study comparing injuries at the hospital in Longyearbyen with injuries registered at the hospital in Harstad in Norway. Home injuries often involve elderly patients, and, accounted for a larger proportion in Harstad (30.5%) than on Svalbard (22% including visitors), while work- and leisure-related injuries accounted for larger proportions on Svalbard (27.2% and 41.9%) than in Harstad (13.2% and 34.8%)[Citation38].
Before 1970, most traumatic injuries occurred in the mines, while after, the majority was caused by leisure-related activities[Citation35]. A Greenlandic study of death causes between 1968 and 1985 found that 16.4% were caused by accidents, most related to fishing, hunting and other traditional lifestyle activities (drowning, boat accidents, and accidental shots)[Citation47]. On Svalbard, 38 people were killed in accidents in the Norwegian communities between 1970 and 1989[Citation35]. 14 deaths were work-related and 24 non-occupational. The risk of being involved in a fatal accident after hours was nearly three times higher among people in the Norwegian communities on Svalbard than on the mainland. Alcohol was reported to be a triggering factor in six of the 24 cases[Citation35]. From Greenland, Bjerregaard reported that 23% of accidental fatalities were alcohol-related. Alcohol thus seems to have been a triggering factor both on Svalbard and in Greenland. It is uncertain whether these findings apply more than 30 years later.
In Greenland, the mortality rate in accidents involving motor vehicles was one third of the Danish rate, as expected considering the limited road networks[Citation47]. On Svalbard, most motor vehicle accidents involved snowmobiles. Between 1997 and 2001, 181 peopled involved in snow mobile accidents were registered at Longyearbyen Hospital. 94 were residents and 87 visitors. Visitors ran a four-time higher risk of being involved in a snow mobile accident, possibly due to lack of experience with snow mobiles and the climatic conditions[Citation37].
Between 1971 and 1995, six non-fatal and four fatal polar bear incidents occurred[Citation36]. Since 1995, Norwegian media have reported two more fatal accidents[Citation48]. This confirms a small and unique risk of being injured or killed by polar bears.
Differences between Norway and Russia in health and emergency preparedness on Svalbard
Most of the 18 included studies collected data from either the Norwegian (n = 13) or the Russian settlements (n = 4), and only one collected from both. The basis for comparative analyses was therefore limited. For example, all studies of trauma epidemiology collected data from the hospital in Longyearbyen only, while no such data from the Russian settlements have been published [Citation35–39]. A few severely injured Russians have probably been treated in Longyearbyen and included in the Norwegian studies. The numbers were not reported, and they would in any case represent a small subgroup of Russian trauma cases. The hospital in Longyearbyen has been organisationally integrated in the University Hospital of North Norway as a department since 2002. This relation could have inspired more research on the Norwegian side, and contributed to this imbalance in scientific publishing.
However, the only comparative study indicated differences between the Norwegian and Russian settlements[Citation24]. This study of self-reported depression revealed a higher incidence for both men and women from the former Soviet Union, compared with the Norwegian population. The authors suggest that differences in home-town latitude between prior to moving to Svalbard may be an explaining factor. The Russians came from lower latitudes and were exposed to larger contrasts in climatic and daylight conditions. It is also worth noting that the data collection for this study was performed in the late 1980s and early 1990s, when socioeconomic differences between the countries were at their highest.
Norwegian-Russian cooperation in search and rescue
Norwegian-Russian cooperation in search and rescue is exemplified by the Maxim Gorkiy accident in 1989. The Soviet cruise liner carried tourists when it hit an ice floe west of Svalbard and started to sink. The Joint Rescue Coordination Centre in Northern Norway informed their Russian counterpart in Murmansk. Soviet military vessels were put on alert and the Soviet consulate in Barentsburg sent helicopters that assisted in the rescue operation. Moreover, the hospitals in Barentsburg and Pyramiden were prepared to receive patients. All 954 people onboard were evacuated by the Norwegian coast guard. The incident is often referred to as a potential Arctic disaster that was avoided due to an excellent cooperation.
Another example is the Operafjell accident in 1996, the worst airplane accident ever in Norway [Citation49,Citation50]. All 141 people aboard (Russians and Ukrainians) were killed. Norwegians and Russians worked closely together on the accident site and with bureaucratic tasks. Although international guidelines assign the country where the accident occurs the main responsibility, it was agreed that both Norwegian and Russian personnel should take part in the search and rescue operation. Also, a joint commission worked for 2 years to establish the cause of the accident. It was concluded that inadequate planning and unsatisfactory crew resource management were among the main causes[Citation51].
Knowledge gaps and recommendations for further research
We identified clear knowledge-gaps concerning occupational hazards among miners, and about Norwegian-Russian cooperation in health and emergency preparedness. In addition, the reviewed studies were generally of low or very low quality, implying considerable uncertainty across all studied outcomes. The most frequent shortcomings were failure to control for confounding, risk for selection bias, a lack of adequate control groups and uncertain risk estimates because the number of visitors was unknown. Future studies should take design guidance from e.g. the Strengthening of the reporting of observational studies in epidemiology (STROBE) guidelines [Citation52], and utilise the potential for comparisons between the Norwegian and Russian populations. Further, publicly available health statistics, e.g. on the mortality and morbidity of infectious diseases is probably an under-utilised data source. Also, application of qualitative research methods entails a potential to address the knowledge gaps concerning Norwegian-Russian cooperation.
Strengths and weaknesses of the study
There are limitations to this review. We conducted the study in adherence with the original version of PRISMA. The updated PRISMA 2020 allows a broader range of sources, which could have provided more information. We consider it unlikely that this would have changed our conclusions. Further, only the main author screened the titles and abstracts. Additional screening may have prevented potential omissions.
Among the strengths of this study is the fact that the reviewed data covers a broad range of topics from various disciplines. Synthesis of both qualitative and quantitative data remains challenging. The analytical tools GRADE and GRADE-CERQual compensate for this challenge and are among the main strengths. It is also a strength that we were able to include studies published in both English, Russian and Scandinavian languages.
Conclusion
This is the first systematic review to explore health risks on Svalbard, and how the healthcare and emergency preparedness system is organised to address these risks. The included studies show that the main risks are associated with accidents, as well as a minor risk for polar bear attacks. There is neither evidence of an increased risk for disease, nor an increased presence of risk factors for diseases. There are significant knowledge gaps what concern health and emergency preparedness and Norwegian-Russian cooperation.
Acknowledgments
The authors thank professor Andrei Rogatchevski at UiT the Arctic University Norway for invaluable help with Russian language interpretation.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Irtun R. The Norwegian Ministry of Health and Care Services. Utredning om foreldre- og barntiltak og akuttberedskapen ved Longyearbyen sykehus. 1997. February 25;1–17.
- Artuso CE. Rural trauma challenges in Alaska. Critical Care Nursing Clinics of North America. 2012;24(4):593–600.
- Farmer J, Munoz S-A, Threlkeld G. Theory in rural health. Aust J Rural Health. 2012;20(4):185–189.
- Royle SA. Health in small Island communities: the UK’s South Atlantic colonies. Health Place. 1995;1(4):257–264.
- Polvi A, Linturi H, Varilo T, et al. The Finnish disease heritage database (FinDis) update-a database for the genes mutated in the Finnish disease heritage brought to the next-generation sequencing era. Hum Mutat. 2013;34(11):1458–1466.
- Palinkas LA, Suedfeld P. Psychological effects of polar expeditions. Lancet. 2008;371(9607):153–163.
- Van Oostdam J, Gilman A, Dewailly E, et al. Human health implications of environmental contaminants in Arctic Canada: a review. Sci Total Environ. 1999;230(1–3):1–82.
- Soininen L, Hantula L. Snowmobile accidents in Lapland. Arctic Med Res. 1992;51 Suppl 7(7):64–70.
- Do MT, Fréchette M, McFaull S, et al. Injuries in the North – analysis of 20 years of surveillance data collected by the Canadian Hospitals injury reporting and prevention program. Int J Circumpolar Health. 2013;72(1):21090.
- Mongeau S, Lightfoot N, MacEwan L, et al. Mining-related lower back injuries and the compensation process: an injured worker’s journey. Workplace Health Saf. 2020;68(1):24–31.
- Gottlieb J. The pattern of medical contacts in a geographically isolated mine village in Greenland. Arctic Med Res. 1990;49(4):195–197.
- Allen RJ, Cangemi MH, Craft CF. 1991 Magadan, USSR/Alaska, USA Dental Exchange Program Report. Alaska Med. 1992;34(1):59–61.
- Johnson MS, O’Connor S, Wennen W, et al. Alaska/Magadan EMS project: phase two. Alaska Med. 1992;34(1):28–37.
- Richards B, Lowe M, Reoux J. Report of the mental health team 1991 Alaska/Magadan medical expedition and exchange. Alaska Med. 1992;34(1):38–50.
- Huppert V, Chuffart R. Collaboration across the Arctic: a tool of regionalization or simple pragmatism? Arctic Yearbook. 2017;1–12.
- Sydnes AK, Sydnes M, Antonsen Y. International cooperation on search and rescue in the Arctic. Arctic Rev Law Politics. 2017;8:109–136.
- Moher D. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–269.
- Staupe-Delgado R, Kruke BI. Preparedness: unpacking and clarifying the concept. J Contingencies Crisis Manage. 2018;26(2):212–224.
- van Ravenhorst MB, van der Klis FRM, van Rooijen DM, et al. Use of saliva to monitor meningococcal vaccine responses: proposing a threshold in saliva as surrogate of protection. BMC Med Res Methodol. 2019;19(1):1–13.
- Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–394.
- Lewin S, Bohren M, Rashidian A, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings—paper 2: how to make an overall CERQual assessment of confidence and create a summary of qualitative findings table. Implement Sci. 2018;13(S1):11–13.
- Lewin S, Booth A, Glenton C, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings: introduction to the series. Implement Sci. 2018;13(S1):1–10.
- Andersen A-B, Ag G, Stenfors L-E. Occurrence of otitis media in an Arctic region. Acta Oto-Laryngologica. 1997;117(sup529):11–13.
- Nilssen O, Brenn T, Høyer G, et al. Self-reported seasonal variation in depression at 78 degree north. The Svalbard Study. Int J Circumpolar Health. 1999;58(1):14–23.
- Lilleng H, Bekkelund S. Seasonal variation of migraine in an Arctic population. Headache. 2009 May;49(5):721–725.
- Bojko E. Metabolical changes induced by adaptation to circumpolar conditions in Spitsbergen. Int J Circumpolar Health. 1997;56(4):134–141.
- Bojko E, Larsen T. Changes in the serum lipid profile in man during 24 months of Arctic residence. Int J Circumpolar Health. 1999;58(3):170–175.
- Breus TK, Boiko ER, Zenchenko TA. Magnetic storms and variations in hormone levels among residents of North Polar area – Svalbard. Life Sci Space Res (Amst). 2015;4:17–21.
- Forberg K, Waage S, Moen B, et al. Subjective and objective sleep and sleepiness among tunnel workers in an extreme and isolated environment: 10-h shifts, 21-day working period, at 78 degrees north. Sleep Med. 2010;11(2):185–190.
- Hanoa R, Baste V, Kooij A, et al. No difference in self reported health among coalminers in two different shift schedules at Spitsbergen, Norway, a two years follow-up. Ind Health. 2011;49(5):652–657.
- Zaman MM, Yoshiike N, Chowdhury AH, et al. The reference value of erythrocyte sedimentation rate for differential diagnosis of rheumatic fever among Bangladeshi children. Journal of Epidemiology. 1996;6(2):109–113.
- Schirmer H, Brenn T, Høyer G, et al. The Svalbard Study: risk of coronary heart disease at 78 degrees north. Arctic Med Res. 1991;Suppl:404–405.
- Yenikeev EA. Исследование воздействия гелиогеофизической активности на практически здоровых людей, работающих в полярной шапке (арх. Шпицберген). Вестник новых медицинских технологий. 2007;(1):63–65.
- Mehus G, Mehus AG, Germeten S, et al. Young people and snowmobiling in Northern Norway: accidents, injury prevention and safety strategies. Rural Remote Health. 2016;16(4):1–13.
- Risholt T. Accident toll in a Norwegian Spitsbergen mining community. Arctic Med Res. 1992;51 Suppl 7(7):37–41.
- Risholt T, Persen E, Solem OI. Man and polar bear in Svalbard: a solvable ecological conflict? Int J Circumpolar Health. 1998;57 Suppl 1(1):532–534.
- Ytterstad B, Dahlberg T. [Snowmobile injuries in Svalbard]. Tidsskrift for den Norske laegeforening: tidsskrift for praktisk medicin, ny raekke. 2005;125(23):3252–3255.
- Ytterstad B, Norheim AJ. The epidemiology of injuries in Svalbard compared with Harstad. Int J Circumpolar Health. 2001 Apr;60(2):184–195.
- Ytterstad B, Norheim J. Snowmobile injuries in Svalbard--a three year study [corrected]. Int J Circumpolar Health. 2001;60(4):685–695.
- Tengesdal SM, Kruke BI. «Vi var fullstendig avhengig av hjelpen fra lokalbefolkningen» - En kvalitativ studie av rollen lokalbefolkningen i Longyearbyen har i håndteringen av snøskred og snøskredøvelser. [Master’s thesis] Stavanger: University of Stavanger,country; 2017: 1–104.
- Sandmo J. Hvit kittel - sort kull: verksleger på Svalbard 1905-1980. Longyearbyen: Store norske Spitsbergen kulkompani; 2005.
- Hanoa R. Longyearbyen sykehus 1916-2016: fra gruvesykehus til Universitetssykehuset UNN: norsk helsetjeneste på Svalbard. Bergen: Fagbokforl; 2017.
- Gottlieb J. [Disease patterns during the first year in the Arctic mining industry]. Ugeskr Laeger. 1992;154(16):1107–1111. Sygdomskontaktmønstret i første ansaettelsesår i arktisk mineindustri.
- Stephens C, Ahern M. Worker and Community Health Impacts Related to Mining Operations Internationally. A Rapid Review of the Literature. Mmsd. 2001 November:1–59. Accessed 2021 Dec 2. https://pubs.iied.org/sites/default/files/pdfs/migrate/G01051.pdf
- Attfield MD, Morring K. An intervention into the relationship between coal workers‘ pneumoconiosis and dust exposure in U.S. Coal Miners. J Safety Res. 1993;24(2):486–492.
- Hwang S-H, Park M-Y, Lee WJ, et al. A comparison of meta-analysis results with and without adjustment for healthy worker effect: cancer mortality among workers in the semiconductor industry. Epidemiol Health. 2021;43:e2021057–0.
- Bjerregaard P. Fatal accidents in Greenland. Arctic Med Res. 1990;49(3):132–141.
- Kalajdzic P. Seks drept siden 1971: – et telt er en invitasjon for isbjørnen. NRK. Accessed 2021 Dec 2, https://www.nrk.no/norge/seks-drept-av-isbjorn-siden-1971-1.15138727
- Bistrova NV. Хроника событий отряда «Центроспас»: 1992-2007 годы. Технологии гражданской безопасности. 2007;(154):4–12.
- Ivert T, Due J. [Air crash on Svalbard. An effective disaster planning at a Norwegian hospital]. Lakartidningen. 1997;94(7):508–509.
- Aircraft Accident Investigation Board. Report on the accident to Vnukovo Airline’s Tupolev TU-154M RA 85621 near Svalbard Airport Longyear, Norway on. 1996 29 Aug ;71. http://www.aviation-accidents.net/report-download.php?id=172
- von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008 Apr;61(4):344–349.