
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
The study is a register-based cross-sectional study aiming to estimate the prevalence of treated osteoporosis in Greenland compared to Denmark and provide a description of the patients with osteoporosis in Greenland. In addition, the study estimates the incidence of hip fractures in Greenland from 2018 to 2020 among people aged 65 years or older. The overall prevalence of patients prescribed medication for osteoporosis among those aged 18 years or older was 0.56% in Greenland and 2.36% in Denmark (p < 0.001). Among those aged 50 years or older, the prevalence was 1.28% and 4.71% in Greenland and Denmark, respectively (p < 0.001). The prevalence increased to 3.41% and 11.18% among patients aged 80 years or older in Greenland and Denmark, respectively. The incidence of hip fractures in Greenland was 6.55 per 1,000 inhabitants in 2020 compared to 5.65 per 1,000 inhabitants in Denmark (NS). In conclusion, the prevalence of treated osteoporosis in Greenland was less than one in four of that of Denmark. The incidence of hip fractures was similar in Greenland than in Denmark. Hence, our findings suggest that a marked number of subjects with osteoporosis in Greenland go untreated.
Introduction
Osteoporosis is a chronic condition defined by low bone mass density (BMD) and microarchitectural deterioration leading to decreased bone strength and a raised fracture risk [Citation1]. Both low BMD and low-impact fractures of the hip or lumbar spine are diagnostic for osteoporosis [Citation1]. Osteoporosis is the most common bone disorder worldwide, and the International Osteoporosis Foundation estimates that one in three women and one in five men older than 50 years will suffer an osteoporotic fracture at some point in life [Citation2]. This is problematic, as the fractures are associated with pain, decreased quality of life, disability, and premature death [Citation1,Citation3], and have an economic impact on society [Citation3,Citation4].
Major risk factors for osteoporosis include female sex and high age [Citation5], and the incidence of osteoporosis in developed countries is expected to increase with the rising life expectancy [Citation3]. Other risk factors include low serum levels of vitamin D, calcium, oestrogen, and a number of diseases such as hyperthyroidism and primary hyperparathyroidism [Citation6], in addition to lifestyle parameters such as smoking, alcohol intake, dietary deficits, certain medications, and immobility [Citation5].
However, despite distinct risk factors [Citation2,Citation5,Citation6] and readily available treatment [Citation7], osteoporosis remains underdiagnosed and undertreated both in Denmark and globally [Citation3,Citation4].
In Greenland, life expectancy increases steeply, smoking is frequent [Citation8,Citation9], and the intake of vitamin D rich traditional Greenlandic foods decreases, lowering vitamin D levels among the population [Citation10,Citation11]. Furthermore, a long season of snow, ice, and reduced daylight may contribute to falls [Citation12].
Only a few studies describe osteoporosis among the native populations in the Arctic, but they emphasise the need for a more comprehensive evaluation of osteoporosis. A study of American Indian and Alaska Natives (AI/AN) report a prevalence of 20.8% of self-reported fractures, of which five per cent were located to hip, spine, or wrist [Citation13]. In Greenland, a questionnaire survey in the capital city Nuuk reported osteoporotic fractures among one in three women aged 70 years or older and low use of prescription medication for osteoporosis [Citation14]. This is in keeping with a review of chest X-rays in Nuuk reporting frequent vertebral fractures but a low treatment frequency [Citation15].
Including data from 96% of Greenland, we thus aimed to estimate the age- and gender-specific prevalence of treatment for osteoporosis and compare the results to data from Denmark, which has a similar health care system to Greenland. We include characteristics of patients treated for osteoporosis in Greenland, and finally, we assess the incidence of proximal hip fractures in Greenland.
Method
Design
The study was performed as a register-based cross-sectional study using data from the electronic medical record (EMR) in Greenland and public registers in Denmark.
Setting
Greenland is the largest Island in the world and is inhabited by 56,081 people. The same EMR is used throughout Greenland, except in the city Tasiilaq in East Greenland, which holds four per cent of the total population. Smaller towns have healthcare centres staffed by doctors and nurses, and settlements have minor healthcare units equipped by staff with basic health care education. Most towns have some regular physicians, but lack of continuity is a common challenge for the Greenlandic healthcare system. All healthcare and prescription medicine is free of charge for inhabitants of Greenland.
Advanced diagnostics such as CT- and MR-scans are accessible only in the capital, but lateral chest radiographs are widely used and available in most towns in Greenland [Citation15,Citation16]. There is no DXA scanner in Greenland, and clinical fracture risk assessment tools (such as FRAX® or QFracture®) are not systematically used in Greenland.
Alendronate, an orally administrated bisphosphonate, is currently the only available pharmacological treatment for osteoporosis in Greenland.
Study population
Greenland
Data on patients treated for osteoporosis in Greenland was extracted from the EMR. Criteria for inclusion were an active prescription of alendronate (anatomical therapeutic chemical (ATC) code M05BA04) by September 21st, 2021, and age 18 years or older.
Data on the numbers of proximal hip fractures from 2018 to 2020 in Greenland was extracted from the EMR on November 8th, 2021, using the International Statistical Classification of Diseases and Related Health Problems (ICD-10) codes DS72.0, DS72.1, and DS72.2. An additional inclusion criterium was age 65 years or older at the time of discharge to match the Danish group. Reoperations, defined as discharges within two years with identical ICD-10 codes to the initial discharge, were excluded.
Denmark
Criteria for inclusion were the purchase of osteoporotic treatment in 2020, which were the most recently available data at the time of the study. Patients were identified in the public online register Medstat.dk, which also provided information on the patients’ age and gender [Citation17].
Treatment of osteoporosis in Denmark was based on a predefined medication group in Medstat, which included ATC codes: M05BA01, M05BA04, M05BA06, M05BA07, M05BB01, M05BB03, M05BX03, M05BX04, G03XC01, H05AA02, H05AA03.
For comparison with the Greenlandic data on hip fractures, the prevalence of hip fractures in Denmark was assessed via a report from The Danish Multidisciplinary Hip Fracture Registry [Citation18]. The report includes data from 2018 to 2020 on patients aged 65 years or older at the time of hospitalisation and operation of a hip-related fracture, including ICD-10 codes DS720, DS721, and DS722. Reoperations within two years after the primary fracture were excluded in the Danish report.
Population numbers, stratified by age and gender as of January 1st 2020, were obtained through public registers in Greenland and Denmark [Citation19,Citation20]. Furthermore, age- and gender stratified population numbers in Greenland were obtained as of January 1st 2018, and 2019 [Citation19].
Variables
Included variables were basic characteristics and all risk factors for osteoporosis available in the EMR at the time of the study: age at the time of the study, gender, height, weight, body mass index (BMI) calculated as weight divided by height squared, and the most recently registered blood pressure measurement. Lifestyle factors included smoking status (yes/no) and physical activity, with inactivity defined as less than 5,000 daily steps. Comorbidities registered in the EMR included diabetes and chronic obstructive pulmonary disease (COPD) and were extracted by date of initial diagnosis.
Diagnostic codes are not used consequently in the primary care setting outside of Nuuk. Thus, active ordinations of medications used in treating thyroid- and parathyroid disorders, defined by ATC codes H03 and H05, respectively, were used as a proxy of the risk factors hyperthyroidism and hyperparathyroidism. ATC codes on steroids for systemic use (H02), psycholeptics (N05), vitamins (A11) and minerals (A12) were used as a proxy of the following osteoporotic risk factors: systemic use of steroids, intake of anxiolytics, sedatives, neuroleptics, tricyclic antidepressants, selective serotonin reuptake inhibitors and supplements of vitamin D and calcium.
The most recent measurements of the following biochemical parameters were extracted from the EMR: plasma low-density lipoprotein (LDL) cholesterol, haemoglobin A1c (HbA1c), plasma thyrotropin (TSH), plasma alanine-transaminase (ALAT), plasma cholesterol, estimated glomerular filtration rate (eGFR), total plasma calcium, free calcium-ion in plasma at pH 7.4, plasma level of 25-hydroxy vitamin D (vitamin D) and plasma parathyrin (PTH).
Statistics
The prevalence of patients treated with antiosteoporotic medicine in Greenland and Denmark was determined by gender and stratified in age groups. Estimates of prevalence and prevalence ratios (PR) were calculated as means ± standard deviation (SD) with 95% confidence intervals (95% CI). tests were performed to compare Greenlandic and Danish age groups, and the results were considered statistically significant when p < 0.05.
The incidence of proximal hip fractures in Greenland was stratified by year of the fracture and gender. The estimates were calculated as fractures per year per 1,000 inhabitants aged 65 years or older and included 95% CIs.
Regarding the descriptive data, continuous data were tested for normality using QQ-plots and variables were described using means ± SD if parametric, otherwise with medians and 95% CIs. When parametric, differences between two groups were tested with the student’s t-test. When non-parametric, the logarithm of the variable was tested with the student’s t-test. Dichotomous data were tested with Pearson’s test.
Ethics
The study was approved by The Ethics Committee for Medical Research in Greenland (no. 2021–10) and The Agency for Health and Prevention in Greenland.
Results
A total of 228 patients taking antiosteoporotic medication were identified in Greenland. The characteristics of these patients are shown in . It may be noted that 79% were women, and more than half were daily smokers. Vitamin D levels were available in 82% of the patients, and mean values were 79 nmol/L. The mean plasma calcium and PTH were within the reference range among the 185 and 28 patients with measured values. The use of systemic steroids and psycholeptics was markedly higher among men compared to women ().
Table 1. Characteristics of patients treated with alendronate in Greenland
In comparison, 110,111 patients were treated for osteoporosis in Denmark, of which 82% were women. The gender distribution was like that of Greenland (p = 0,166).
illustrates the prevalence of patients treated for osteoporosis in Greenland and Denmark, both in total and by age groups. The overall prevalence in Greenland was 0.56% (95% CI: 0.49–0.64), and 0.95% (95% CI: 0.81–1.09) among women and 0.22% (95% CI: 0.16–0.29) among men. In Denmark, the total prevalence was 2.36% (95% CI: 2.35–2.37), 3.84% (95% CI: 3.82–3.87) among women and 0.84% (95% CI: 0.83–0.85) among men.
Figure 1. Prevalence of treated osteoporosis (% of population) in Greenland and Denmark, stratified by age. Total prevalence for each country is presented separately in upper left part of the figure. Vertical bars representing 95% confidence intervals. Significant p-values marked as <0.05*, <0.01**, and <0.001***.
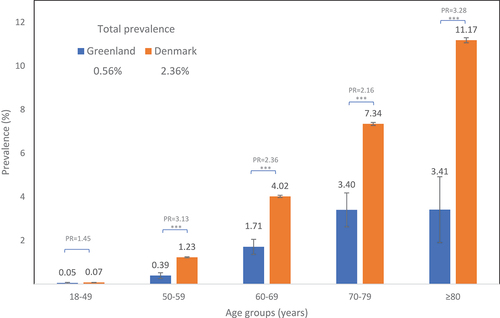
The total treatment frequency was markedly higher in Denmark compared to Greenland, with a PR of 4.18 (p < 0.001) (). The higher treatment frequency in Denmark accounted for all the age groups 50–59, 60–69, 70–79, and 80 years or older (all p < 0.001). Treatment frequency increased with age in both populations. Among those aged 50 years or older, the frequency of treatment for osteoporosis in Greenland was 1.28% (95% CI: 1.11–1.145) compared to 4.71% (95% CI: 4.68–4.74) in Denmark (p < 0.001), and it was highest among age group 80 years or older (3.41% (95% CI: 1.90–4.92) and 11.18% (95% CI: 11.06–11.29) in Greenland and Denmark, respectively).
presents the prevalence of prescription medication for osteoporosis by age and gender in Greenland and Denmark. The gender-specific prevalence of osteoporosis in Greenland increased with age until the age of 80 years, with the highest prevalences found among those aged 70–79 years for both women (6.30% (95% CI: 4.75–7.86)) and men (1.04% (95% CI: 0.46–1.63)). In Denmark, the prevalence increased continuously with higher age with the prevalence peaking in the age group 80 years or older for both women (15.60% (95% CI: 15.43–15.78)) and men (4.49% (95% CI: 4.37–4.62)) (). Except for the men aged 70–79 years (p = 0.122), Denmark treated significant more patients within all the age- and gender stratified groups (all p < 0.01) than Greenland, counting for patients aged 50 years or older.
Table 2. Age- and gender-specific prevalence of treated osteoporosis in Greenland and Denmark
presents the incidences of hip fractures between 2018 and 2020 in Greenland and Denmark for inhabitants 65 years or older. All the incidences of hip fractures in Greenland were higher than corresponding estimates from Denmark, except for men in 2020. However, there was no statistically significant difference between the two countries.
Table 3. Incidents of hip fractures in Greenland and Denmark for inhabitants ≥ 65 years * all danish values from the danish multidisciplinary hip fracture registry’s year report 2020 [Citation18]
Discussion
Our results suggest that the prevalence of treated osteoporosis in Greenland is one-fourth of that of the population in Denmark, despite similar incidences of hip fractures. This discrepancy indicates a marked undertreatment of osteoporosis in Greenland.
Treatment frequency for osteoporosis among patients aged 50 years or older was above two percent in 20 out of 25 European countries, and the average prevalence was around five per cent [Citation3]. The corresponding prevalence of 1.3% in our data places Greenland among the three countries with the lowest treatment frequency for osteoporosis, just above Bulgaria and Lithuania. Denmark is closer to the average value with an estimated treatment prevalence of around 5% [Citation3]. This suggests either a low occurrence of fragility fractures or room for improvement of diagnostics in Greenland.
The total prevalence of treatment in Greenland and Denmark increased with age, as the highest total prevalence was found in the age group 80 years or older. In addition, 79% of treated patients in Greenland were women, comparable to 82% of patients in Denmark. Our findings regarding age and gender comply with the underlying disease mechanisms, as it has been established elsewhere [Citation21,Citation22].
A low treatment rate for osteoporosis was previously described in the capital of Greenland as evaluated by a questionnaire study. Less than 3.4% of 181 participants aged 54–77 years reported using antiosteoporotic medicine [Citation14]. In addition, only 6.5% of those reporting a previous fragility fracture took an antiosteoporotic drug. Interestingly, risk factors for osteoporosis were frequent in these data [Citation23], and 15% reported a family history of osteoporosis, 18% of women reported premature menopause and one out of three women aged 70 years or older reported at least one prior fragility fracture verified by X-ray. Lastly, Sørensen et al. evaluated vertebral deformation, including all 203 people having a lateral thoracic X-ray taken over three months at the hospital in the capital Nuuk [Citation17]. They found vertebral fractures that merit antiosteoporotic treatment to be common. They further reported a marked discrepancy between fracture frequency and pharmacy handouts of treatment for osteoporosis during parallel months in 2007.
Although the abovementioned studies are all limited to Nuuk, they indicate that osteoporosis is present in Greenland and possibly underdiagnosed, suggesting that more patients in Greenland could benefit from treatment.
The Danish estimates of hip fracture incidence correlate well with equivalent estimates from the US. In 2015, the incidence in the US was 7.30 fractures per 1,000 women [Citation24], compared to 7.41 fractures per 1,000 women in Denmark in 2018 [Citation18]. In contrast, the estimate for women in Greenland was 8.43 per 1,000 women in 2018 ().
An increased incidence of hip fractures among Inuit people compared to Caucasians from the southern US has been described by Pratt et al., who examined hip fracture rates among Alaskan Inuit aged 65 years or older in 1996–99. The authors report that Inuit women suffered twice as many hip fractures as US women within all age groups, except when aged 85 years or older [Citation25]. However, this study did not consider environmental differences, like sun exposure or slippery winter conditions. Another study of aboriginals, including First Natives, Metis and Inuit people in Canada, found an almost twofold higher rate of osteoporotic fractures than among non-aboriginals but ascribed this to a greater prevalence of comorbidities and substance abuse [Citation26].
The higher incidence of fractures found in our study could be due to ethnic differences in osteoporotic fracture risk, as reported in other studies [Citation27–29]. Secondly, it could be due to environmental differences, as some studies have found increased incidences of falls during icy winters and in slippery conditions [Citation30,Citation31]. Lastly, the higher incidence of hip fractures in Greenland could indicate that the lower prevalence of patients treated for osteoporosis in Greenland is leaving undiagnosed patients at a higher risk of osteoporotic fractures.
Strengths and limitations
A major strength of this study is the use of national registers leading to the inclusion of more than 96% of the adult population in Greenland and 100% of the adult population in Denmark. This makes it the first national study to estimate the prevalence of patients receiving antiosteoporotic treatment in Greenland. However, data on some variables extracted from the EMR was of older date or completely missing, especially biochemical parameters and lifestyle factors. Data on vitamins and minerals were used as a proxy for supplements of vitamin D and calcium but also included all other vitamin and mineral supplements. In addition, some important risk factors were unavailable in the EMR, such as information on prior fractures, family history of osteoporotic fractures, and time of menopause. However, similar rates of premature menopause in Denmark and Greenland have been reported previously [Citation23,Citation32]. In addition, data regarding whether alendronate was prescribed because of fracture or as prophylactic treatment would have been preferred but was not obtainable.
Alendronate is the only available antiosteoporotic medication in Greenland, making it feasible as a proxy for antiosteoporotic treatment in Greenland. In Denmark, some patients are treated for osteoporosis with other medications than those included in our data extraction, e.g. zoledronic acid. Zoledronic acid is also used to treat Paget’s Disease, and it would be impossible to distinguish whether it was explicitly used against osteoporosis in our data extraction. For this reason, the actual number of patients treated in Denmark may be slightly higher than our estimate.
We included the most recent available data on antiosteoporotic treatment. However, the data covers different periods of time. In Greenland, the data included patients with an active prescription of alendronate at the time of data extraction (September 21st, 2021), while data from Denmark included patients who purchased antiosteoporotic treatment throughout 2020. Still, we consider our data valid for providing a comparative view of treatment frequency.
Regarding hip fractures, our data was limited by the lack of information on whether a low or high impact trauma led to the fracture and thus if the fracture was diagnostic for osteoporosis. However, hip fractures in old age are mainly osteoporotic, and the comparative data of similar groups between the two countries include the same limitations in both groups, thus justifying the comparison. Finally, an important limitation was the relatively small study population in Greenland, limiting the statistical strength, especially in the older age groups. Life expectancy is ten years shorter in Greenland than in Denmark, and more osteoporosis and fractures are expected in an older population, which should be taken into account in the comparison.
In conclusion, the prevalence of treated osteoporosis was four times lower among the general population in Greenland than in Denmark, while the incidence of hip fractures was similar between the two countries. Our results suggest that osteoporosis is undertreated and may be underdiagnosed in Greenland, and a national strategy for diagnosing and treating osteoporosis is desirable.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Kanis JA, Melton LJ 3rd, Christiansen C, et al. The diagnosis of osteoporosis. J Bone Miner Res. 1994 Aug;9(8):1137–8.
- International Osteoporosis Foundation, Epidemiology of osteoporosis and fragility fractures. [Internet]: International Osteoporosis Foundation; cited 2021 Oct 22]. Available from 2021 Oct 22: https://www.osteoporosis.foundation/facts-statistics/epidemiology-of-osteoporosis-and-fragility-fractures
- Hernlund E, Svedbom A, Ivergård M, et al. Osteoporosis in the European Union: medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos. 2013;8(1):136.
- Vestergaard P, Rejnmark L, Mosekilde L. Osteoporosis is markedly underdiagnosed: a nationwide study from Denmark. Osteoporos Int. 2005 Feb;16(2):134–141.
- Foundation IO. International osteoporosis foundation, risk factors. Internet] [cited 2021 Oct 22]. Available from 2021 Oct 22: https://www.osteoporosis.foundation/health-professionals/about-osteoporosis/risk-factors
- Holm JP, Hyldstrup L, Jensen JB. Time trends in osteoporosis risk factor profiles: a comparative analysis of risk factors, comorbidities, and medications over twelve years. Endocrine. 2016 Oct;54(1):241–255.
- Kanis JA, Cooper C, Rizzoli R, et al. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. 2019 Jan;30(1):3–44.
- Bjerregaard P, Larsen CVL, Sørensen IK, et al. Alcohol in Greenland 1950-2018: consumption, drinking patterns, and consequences. Int J Circumpolar Health. 2020 Dec;79(1):1814550.
- Bjerregaard P, Larsen CVL. Three lifestyle-related issues of major significance for public health among the Inuit in contemporary Greenland: a review of adverse childhood conditions, obesity, and smoking in a period of social transition. Public Health Rev. 2018;39:5.
- Nielsen NO, Jørgensen ME, Friis H, et al. Decrease in vitamin D status in the Greenlandic adult population from 1987-2010. PLoS One. 2014;9(12):e112949.
- Andersen S, Laurberg P, Hvingel B, et al. Vitamin D status in Greenland is influenced by diet and ethnicity: a population-based survey in an Arctic society in transition. Br J Nutr. 2013 Mar 14 109(5):928–935.
- Close JC, Lord SL, Menz HB, et al. What is the role of falls? Best Pract Res Clin Rheumatol. 2005 Dec;19(6):913–935.
- Frech T, Ma KN, Ferrucci ED, et al. Prevalence of fracture and osteoporosis risk factors in American Indian and Alaska Native people. J Health Care Poor Underserved. 2012 Aug;23(3):1157–1173.
- Jakobsen A, Laurberg P, Andersen S. Osteoporosis is common in Greenland and treatment is scarce. Int J Circumpolar Health. 2013;72:332–334.
- Sørensen VN, Wojtek P, Pedersen DS, et al. An efficient case finding strategy to diagnose osteoporosis in a developing society with low treatment frequency. J Endocrinol Invest. 2015 Aug;38(8):841–847.
- Fleischer I, Schæbel LK, Albertsen N, et al. Diagnosis of osteoporosis in rural Arctic Greenland: a clinical case using plain chest radiography for secondary prevention and consideration of tools for primary prevention in remote areas. Rural Remote Health. 2017 Jan-Mar;17(1):3910.
- Sundhedsdatastyrelsen, medstat: lægemiddelgrupper: osteoporose behandling. 2020, Denmark, hele landet, køn, samlet, mænd, kvinder, 1 års grupper 0-95+ år, antal personer [danish healt authority, medstat; medication groups: osteoporosis treatment. 2020, Denmark, whole country, sex, gathered, men, women, 1 year groups 0-95+ years, number of people] [internet]. cited 2021 sep 21]. Available from 2021 sep 21: https://medstat.dk/da/.
- Röck ND, Riahi LB, Christensen HC, et al. Dansk tværfagligt register for hoftenære lårbensbrud, national årsrapport 2020 [the danish multidisciplinary hip fracture registry, National year report 2020]. the danish clinical quality program and the danish multidisciplinary hip fracture registry. Clinical Epidemiology. 2020;12(19):9–21.
- Danmarks Statistik, Befolkningen i distrikter og kommuner 1. januar efter bosted, fødested, alder, område, køn og tid [Statistics Denmark, Population in districts and municiplities 1st of January by place of residence, place of birth, age, territory, sex and time] [Internet]. 2018, 2019, 2020 cited 2021 Sep 21]. Available from 2021 Sep 21: https://bank.stat.gl/pxweb/da/Greenland/Greenland.
- Danmarks Statistik, Folketal pr. 1. januar efter tid, alder og køn, Danmark [Statistics Denmark, Population by 1st of January by time, age and sex, Denmark] [Internet]. 2020 cited 2021 Sep 21]. Available from 2021 Sep 21: https://www.statistikbanken.dk/.
- Looker AC, Orwoll ES, Johnston CC Jr., et al. Prevalence of low femoral bone density in older U.S. adults from NHANES III. J Bone Miner Res. 1997 Nov;12(11):1761–1768.
- Wade SW, Strader C, Fitzpatrick LA, et al. Estimating prevalence of osteoporosis: examples from industrialized countries. Arch Osteoporos. 2014;9:182.
- Jakobsen A, Laurberg P, Vestergaard P, et al. Clinical risk factors for osteoporosis are common among elderly people in Nuuk, Greenland. Int J Circumpolar Health. 2013;72(1):19596.
- Lewiecki EM, Wright NC, Curtis JR, et al. Hip fracture trends in the USA, 2002 to 2015. Osteoporos Int. 2018 Mar;29(3):717–722.
- Pratt WB, Holloway JM. Incidence of hip fracture in Alaska Inuit people: 1979-89 and 1996-99. Alaska Med. 2001 Jan-Mar;43(1):2–5.
- Leslie WD, Derksen S, Prior HJ, et al. The interaction of ethnicity and chronic disease as risk factors for osteoporotic fractures: a comparison in Canadian Aboriginals and non-Aboriginals. Osteoporos Int. 2006;17(9):1358–1368.
- Barrett-Connor E, Siris ES, Wehren LE, et al. Osteoporosis and fracture risk in women of different ethnic groups. J Bone Miner Res. 2005 Feb;20(2):185–194.
- Bow CH, Cheung E, Cheung CL, et al. Ethnic difference of clinical vertebral fracture risk. Osteoporos Int. 2012 Mar;23(3):879–885.
- Cauley JA. Defining ethnic and racial differences in osteoporosis and fragility fractures. Clin Orthop Relat Res. 2011 Jul;469(7):1891–1899.
- Kakara RS, Moreland BL, Haddad YK, et al. Seasonal variation in fall-related emergency department visits by location of fall - USA, 2015. J Safety Res. 2021 Dec;79:38–44.
- Lépy É, Rantala S, Huusko A, et al. Role of winter weather conditions and slipperiness on tourists’ accidents in finland. Int J Environ Res Public Health. 2016 Aug15;13(8):822.
- Andersen S, Laurberg P. Age discrimination in osteoporosis screening–data from the Aalborg university hospital record for osteoporosis risk assessment (aurora). Maturitas. 2014 Apr;77(4):330–335.