
Abstract
Despite the fact that healthcare spending in Kazakhstan increased annually from 2011 to 2020, the country’s healthcare system is seriously underfunded. For this reason, household spending in Kazakhstan plays a significant role in overall health spending. According to WHO, if the share of private spending in total health care spending does not exceed 20%, the health care system can be considered sustainable. The risk of a decrease in the purchasing power of the population increases in cases where this indicator is exceeded, which in turn leads to negative consequences for the population itself. Therefore, the Government of Kazakhstan needs to take decisive measures to reduce the “out-of-pocket expense” of the population for health care, especially the cost of purchasing medicines. Effective government policy, timely reforms and mutually beneficial cooperation with pharmaceutical market actors can reduce the level of “out-of-pocket expenses” of the population for health care to generally accepted world indicators. Based on this, the study of different views on solving problems related to public and private spending in health care, price regulation and building an effective drug pricing system is an important condition for building an effective health care system.
1. Introduction
Kazakhstan spent less on current health care spending in 2018 (2.9% of GDP) than OECD countries (USA 16.9%; Canada 10.7%; Australia 9.3%; an average of OECD—8.8%, Turkey—4.2% of GDP). Kazakhstan’s neighbors, such as Russia (5.3% of GDP) and China (4.9% of GDP), also spent more money on healthcare. In 2019, Kazakhstan’s health spending as a share of GDP increased to 3.3% (public spending 1.9%, private spending 1.4%), and by 2025, total spending is expected increasing to 5% of GDP. According to the data for 2020, Kazakhstan’s healthcare system ranked 174th out of 189 countries in terms of healthcare costs (3.1% of GDP; World Health Organization, Citation2021). Weak state financing of the health care system forces the population of Kazakhstan to spend personal finances on medical services. The growth of current spending on health care per capita was 106% and government spending per capita was 86% in Kazakhstan from 2011 to 2018. In 2018, total health spending per capita in Kazakhstan was 276 US dollars (2.82% of GDP), in the USA—10.515 US dollars (16.69% of GDP), in Canada—5.018 US dollars (10.81% of GDP), in Australia—5.364 US dollars (9.16% of GDP), in Turkey—390 US dollars (4.12% of GDP), in Russia—609 US dollars (5.36% of GDP), in China—501 US dollars (5.17% of GDP). For correct comparability of the values of health expenditure indicators with the rest of the world, it is necessary to convert them into dollars at PPP. The level of current expenditure per capita in Kazakhstan in 2018 amounted to 735 US dollars according to PPP (current international US dollars). The value of this indicator is more than 4 times lower than the level of expenditures per capita in OECD member countries (3.992 US dollars according to PPP). In the United States, the level of current health care spending per capita in 2018 was (10.515 US dollars according to PPP), Canada (5.427 US dollars according to PPP), Australia (4.876 US dollars according to PPP), Turkey (1.152 US dollars according to PPP), Russia (1.570 US dollars according to PPP) and China (784 US dollars according to PPP). It is worth noting that Kazakhstan in terms of income per capita (7.830 US dollars) in 2018 was slightly inferior to China (9.470 US dollars), Russia (10.230 US dollars), Turkey (10.380 US dollars) and lagged far behind Canada (44.860 US dollars), Australia (53.190 US dollars) and the USA (62,850 US dollars).
In Kazakhstan a significant share is occupied by the costs of purchasing medicines and medical supplies in the structure of health care expenditures; these costs increased by 183% from 2011 to 2018. In 2018, total spending on drugs and medical devices was 70 US dollars per capita in Kazakhstan (government spending 15 US dollars, private spending 55 US dollars). Similar average spending per capita in OECD countries in 2018 was 376.7 US dollars. In Kazakhstan, the structure of private health spending includes household spending, business spending, and voluntary health insurance. In 2018, household expenditures dominated the most in the structure of expenses—85.8% were out-of-pocket expenses, which most of all money were spent on the purchase of drugs and medical goods (60%; Zagidullina & Omirbaeva, Citation2019).
It can be noticed that in 2019, private spending in Kazakhstan reached 1.7 billion US dollars, 85% of which was spent by households. And still most of their expenses were spent on purchasing of drugs. The problem of the high cost of medicines has becoming extremely relevant for Kazakhstan recently. Since 2009, the government of Kazakhstan has been taking measures to stabilize prices for medicines, despite this, inflation still affects negatively on the purchasing power of the population. Thus, the official inflation for medicines in Kazakhstan in 2015 amounted to 31.3%; in 2016–17.7%; in 2017–6.6%; in 2018–7.8%; in 2019–6.2%; in 2020–9.9%. In 2018, the population of Kazakhstan spent 780 million US dollars on medicines, while the government spent 280 million US dollars. As you know, Kazakhstan has set the goal of joining the 30 most developed countries of the world by 2050, and in order to achieve this goal, it is necessary to overcome the existing gap in development between the OECD countries and Kazakhstan, including the reduction of population expenditures on healthcare. Drugs account for the largest “out-of-pocket expense” of the population on health care. Therefore, one of the solutions to the problem of reducing the “out-of-pocket expense” of the population for health care may be measures to regulate the prices of medicines, create mechanisms for health insurance, increasing of government spending, etc.
2. Literature review
Financial protection of the population is a key component of universal coverage of health services and its monitoring which is based on two indicators: catastrophic expenditures and poverty rates. Measuring catastrophic expenditures and poverty rates is difficult because there are different calculation methods, and there are no universally accepted ones. Measuring the out- pocket expenses of the population helps to assess the impact on living standards and the impact of the health care financial system on improving financial protection (Hsu et al., Citation2018). Lee et al. (Citation2016) showed in their research that even with universal health insurance, the Republic of Korea faces the problem of high “out-of-pocket” expenses. People with disabilities have higher costs than people without disabilities. It was found that 44.3% of households in which people with disabilities lived spent more than 10% of their total spending on health care. According to scientists, low paying capacity and high health care costs lead to the impoverishment of the population. Without additional external financial assistance, households with people with disabilities will be forced to save on other members of the household. It was also found that financial assistance from the state helps to reduce household spending on health and medicines.
Research studies in countries with Universal Health Coverage (UHC) show that a high “out-of-pocket expense” is a risk factor for death, physical disability and impoverishment (Baggio et al., Citation2018). Baggio et al. came to the conclusion that reducing personal expenses and developing voluntary private insurance can protect against large financial losses, premature illness and death. The data show that there are health inequalities in OECD countries, with public health insurance covering an average of 70% of health care costs in these countries (Pierre & Jusot, Citation2017). A study by Grima et al. (Citation2018) analyzed 6 Mediterranean countries and concluded that these countries spend less on health care than the EU average, and the population’s out-of-pocket spending on health care is higher than the EU average. The Mediterranean countries tried to reduce out-of-pocket spending on health care through reforms, but the economic crisis led to cuts in public spending, for example, in Greece and Italy.
Most developed countries are trying to reduce private spending to an optimal level. The specific features of the medical services market explain the need for such a state policy, citizens cannot postpone the purchase of most services when a need for treatment arises, in case of illness, there is a high probability of loss of income, information asymmetry arises in health care, etc. (Callander et al., Citation2019). In the event of an increase in health care costs from households with serious illnesses, there are excessively high risks of unavailability of medical care and catastrophic costs for households (Salari et al., Citation2019).
The problem of impoverishment of the population, especially rural residents, due to the cost of expensive diseases (cancer, cardiovascular diseases) is typical for most countries of the Global South. Undoubtedly, various factors such as economic development, political system, traditions, religion, population aging, etc., affect the health care systems of these countries in different ways. The development of economies has led to an increase in health care spending in South Africa, Brazil, Jordan and other countries of the Global South. Despite this, the level of spending on health care in most developing countries (Turkey, China and Russia) is still lower than the world average. Increasing investment in people’s health undoubtedly has a positive impact on the population and net income generation in the future (Jakovljevic et al., Citation2021).
Boing et al. (Citation2014) in their research argue that high household health spending has a significant impact on the population, forcing people to delay treatment or not buy necessary drugs. High health spending can reduce the consumption of other goods and services needed in everyday life, thereby increasing social risks and tensions. A study in Brazil found that prescription drugs account for a large share of the population’s health care spending. It is prescription drugs that cause high costs for poor Brazilian households.
According to the WHO, the rise in poverty due to health spending occurs in countries at all income levels, but higher in countries with higher private health spending. According to a 2006 study in 11 Asian countries, a 2.7% increase in private health care spending on the day of payment for health care led to an increase of 78 million people living on less than 1 US dollar the next day (Van Doorslaer et al., Citation2006). Jakovljevic et al. (Citation2020) compared the performance of health care systems in 9 leading Asian countries. The study determined that the main factors influencing efficiency were the quality of management and ongoing health care costs. In 7 non-OECD Asian countries, in addition to the above factors, other factors played an important role, such as: urbanization, population density, ecology, water and food quality. It is also noted that in order to achieve universal health coverage, the governments of these countries need to control private health spending through risk-sharing agreements.
Some households channel most of their budgets to health care, thereby limiting the ability to cover other costs which leads to disastrous consequences. The government must implement policies to improve access to and quality of coverage of health care, including medicines for reducing the economic burden on families prone to catastrophic health spending (Koch et al., Citation2020).
The continuing lack of public resources makes it necessary and unavoidable for the population to participate in the financing of health care. In addition, the growth of incomes and the formation of a solvent middle class that is ready to invest in their health, increase the demand for paid medical services (Pallegedara & Grimm, Citation2018).
For socially vulnerable segments of the population, “out-of-pocket” expenses can become an unbearable financial burden, because obtaining the necessary medical care requires significant costs from limited budgets (Mahumud et al., Citation2017). If countries have effective health insurance and co-payment systems, socially vulnerable citizens of these countries will be less exposed to financial risks, and inequality among the population will decrease accordingly (Baird, Citation2016).
3. Background
After the collapse of the Soviet Union in 1991, Kazakhstan inherited the Soviet healthcare model based on the Semashko system. In the transition from a command economy to a market economy, the healthcare system faced a number of problems that are still relevant today. For example, from 1995 to 1998, they tried to introduce a system of compulsory medical insurance in Kazakhstan, but due to a number of difficulties, the system of compulsory medical insurance was introduced only in 2020. In addition, there were other challenges for the health care system, such as rising drug prices, low life expectancy compared to developed countries, high mortality from treatable causes, chronic underfunding of the health care system, and organizational problems.
The government of Kazakhstan has been trying for several years to solve the problem of rising prices for medicines. So, the Ministry of Health in Kazakhstan began to participate in negotiations with pharmaceutical companies and associations to curb the rise in prices for socially important drugs in 2009. Also the government began to regulate wholesale and retail drug mark-ups under the “Guaranteed volume of free medical care” (GVFMC) in 2009. In February 2009, the Government of Kazakhstan established LLP “SK-Pharmacy”, a single distributor of medicines and medical devices in order to reduce government spending. Thanks to centralized procurement, the government began to regulate the prices of purchased medicines and medical products, thereby increasing the population’s availability to medicines and medical products.
Memorandums on prices for medicines concluded since 2009 have not yielded positive results, due to the large number of intermediaries between the population and drug manufacturers, due to the lack of legislative frameworks in the field of pricing, unjustified pricing in the wholesale and retail sale of medicines, poor development of pharmaceutical infrastructure in rural areas and etc. In May 2013, the Chairman of the Agency of the Republic of Kazakhstan for the Protection and Development of Competition Kuandykov B.B. spoke about the need for active state intervention in the process of pricing for medicines and the development of legislative acts in this area (Orazbayev, Citation2013).
In 2013, the “Rules for the organization and monitoring of prices for medicines, medical devices, as well as their formation within the GVFMC” came into force in Kazakhstan. According to these rules, Kazakhstan entered to external reference pricing (ERP) within the framework of GVFMC. Having a legislative base, Kazakhstan actually began the transition to ERP only after 2015. According to the new rules, Kazakhstan began to use 8 countries in its reference basket, which were divided into main and reserve countries. Main countries are: Belarus, Hungary, Latvia, the Czech Republic. Reserve countries are: Turkey, Russia, Austria, Ukraine. Together with the reference countries, the British National Pharmaceutical Formula and International Price Bases were used for ERP.
In 2017, Kazakhstan expanded the reference basket to 39 countries (Vogler et al., Citation2019). In comparison with the EAEU, CIS, EU and OECD countries, the Kazakhstani reference basket in 2017–2018 was the largest in terms of the number of reference countries (Table ).
Table 1. External reference basket of Kazakhstan in 2017 and 2019
Thus, from the OECD and EU countries, Hungary and Poland had 31 countries in the reference baskets, Bulgaria had 17 countries in the reference basket, Japan and New Zealand had 3 reference countries each, Australia had 2 reference countries, and Luxembourg used the country of origin of the medicine as a reference country (Rémuzat et al., Citation2015).
April 19 in 2019, new rules for regulating prices for drugs were approved, and the ERP system was changed. According to the new rules, prices began to be regulated for all types of drugs, including drugs purchased under MSHI and GVFMC. According to the new rules, Kazakhstan has reduced the number of reference countries to 16 (Table ). Instead of the British national drug formulary and international prices, Kazakhstan began to use the prices of the countries of drug manufacturers.
As we can see from the given examples, Kazakhstan having studied the world experience not so well enough, changed the ERP system 3 times in 6 years, in 2015, in 2017, in 2019. In the new 2019 reference basket, Kazakhstan does not use the principle of geographic proximity to the reference country and has not included any Central Asian country in its reference basket. Some OECD countries necessarily include countries with which they have common borders in their reference baskets (Ruggeri & Nolte, Citation2013).
Kazakhstan in its reference basket mainly uses high-income countries, 11 out of 16. Azerbaijan, Belarus, Bulgaria, Turkey and Russia were classified as upper-middle-income countries. Countries with lower middle income are not used in Kazakhstan’s reference basket. It would be advisable to exclude from the Kazakhstan’s reference basket countries with high GDP per capita indicators: Slovenia, the Czech Republic, Greece and Estonia. Our proposals are based on the research of the Medical Technology Research Group (MTRG), which in their studies on the example of Spain proved that the inclusion of countries with a high level of GDP per capita in the reference basket leads to higher prices. Accordingly, if countries with lower GDP are included in the reference basket of countries, this will lead to a decrease in drug prices on the contrary.
Kazakhstan did not include in its reference basket the EAEU integration countries such as Armenia and Kyrgyzstan with which close economic relations have been established. Unlike Kazakhstan, 15 EU countries use the principle of close economic relations when compiling reference baskets. For example, this principle is used by: Austria, Belgium, Italy, Spain, Slovakia, Finland, etc. (Robinson et al., Citation2019). Kazakhstan should include Armenia, Kyrgyzstan, Uzbekistan, Moldova, Ukraine and Georgia in its reference basket.
Although the ERP method is easy to use and helps to optimize prices, as well as it does not require large costs and administrative resources, this method of determining prices is not used in some developed and developing countries. For example, from the OECD countries the ERP method is not used by the USA, Great Britain, Sweden and Chile (Espin et al., Citation2011). It should be noted that in most EU and OECD countries, ERP is used for reimbursement policy (Kawalec et al., Citation2017). Since 2020, Kazakhstan has introduced a co-payment system, so according to the order of the Minister of Health of the Republic of Kazakhstan dated 31 December 2019 № 154, Kazakhstan has established the rules for making co-payment for medicines and medical devices. The introduction of reimbursement was supposed to increase the responsibility of citizens for their health, reduce illegal payments, increase the transparency of the healthcare system, and minimize the costs of the population and the government. However, due to the unavailability of the information system for drug supply, the reimbursement procedure in Kazakhstan was postponed indefinitely.
Kazakhstan needs to establish an effective reimbursement system that, interacting with ERP, would be able to control public and private costs of medicines. ERP and reimbursement mechanisms could be effectively applied to reimbursable drugs, as it is done in developed countries by the OECD. Many OECD countries use other pricing methods to contain drug prices, largely due to the shortcomings of the ERP method:
1) In the European market, large pharmaceutical companies begin to set prices for medicines from the northern Scandinavian countries or from the UK, Germany or Switzerland, where the income level is much higher than in Southern or Eastern Europe (Stargardt & Schreyögg, Citation2006);
2) During negotiations on drug prices, pharmaceutical companies can give discounts to governments. Such negotiations mask the real price that countries are paying and “undermine” the ERP process (Persson & Jönsson, Citation2016);
3) According to research from the London School of Economics, the use of ERP in the long term can lead to a significant increase in drug prices (example of Greece in 1996; Yfantopoulos, Citation2008);
4) Price fluctuations in one country can cause large price fluctuations in another country (Elek et al., Citation2017);
5) Countries using ERP may differ in terms of morbidity, medical culture, paying capacity of the population, structure of the pharmaceutical market, distributor margins, tax system, etc. (Vandoros & Stargardt, Citation2013).
Global experience shows that different pricing methods are used for different medicines. For example, when determining prices for “generic drug”, internal reference pricing is often used; “Original” and reimbursed drugs are better defined by the ERP method; the prices of “innovative” medicines are determined by the method of assessing the value of the medicine. Many developed and developing countries use mixed pricing methods for medicines.
One of the mechanisms for reducing the “out-of-pocket expense” of the population for health care is social health insurance. The lack of a health insurance system or insufficient funding of the health insurance system hinders access to health services for vulnerable groups of the population. The increase in coverage and the consolidation of 5 fragmented insurance systems in Turkey led to a reduction in the annual “out-of-pocket expense” of the population for health care, including medicines. Turkey, through the Green Card health insurance program, has been able to provide financial protection to the poor (Tirgil et al., Citation2019). In Indonesia and Vietnam, the introduction of social health insurance has reduced the “out-of-pocket expense” of the population. In China and India, studies have shown that health insurance systems have not been very successful in reducing the “out-of-pocket expense” of the population (Sriram & Khan, Citation2020). The different results are due to differences in health insurance systems.
From 1 January 2020, the MSHI system began to operate in the Republic of Kazakhstan. According to the Ministry of Health of Kazakhstan, the introduction of the MSHI system will reduce the “out-of-pocket expense” of the population for medical services, including the purchase of drugs. Thus, by 2025, the government plans to reduce the “out-of-pocket expense” of the population for health care to 30%. Also, thanks to MSHI, it is planned to increase access to drug provision to 3.5 million people in 2020. MSHI’s 2020 budget was 1.2 billion US dollars.
4. Results
4.1. Data
We conducted a sociological survey of drug consumers in the Karaganda agglomeration. This agglomeration is one of the largest urban agglomerations in the country. Moreover it is the industrial center of Kazakhstan. 88% of the population of the Karaganda region lives in the Karaganda agglomeration. 303 respondents took part in the survey, the largest number of respondents belonged to the age group of 35–63 years old (113 people), 25–34 years old (112 people), 18–24 years old (64 people), 63 and over years old (14 people). The survey involved 228 women and 75 men. Of the respondents: employed—204 people; students—51 people, pensioners—21 people; unemployed—14 people; chose the other option—13 people. It should be noted that according to a study by “Dosmart”, the main buyers of drugs in Kazakhstan are women (87% of sales), the average age of drug buyers is 36–50 years. Respondents were asked the question: “What problems do you face when looking for and buying medicines?” Respondents had the opportunity to select multiple answers.
Figure 1. Problems faced by the population when buying medicines.
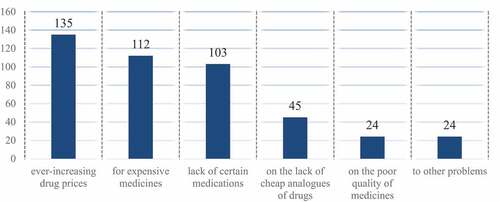
shows a sociological survey showing what problems the population faces when buying medicines. Most respondents (135 people) complained about the constant rise in prices; 112 people mentioned expensive medicines; lack of certain medicines was noticed by 103 people; the lack of cheap analogues of medicines by 45 people; 24 respondents complained about the poor quality of medicines and other problems. The result of the survey showed that the population is concerned about the rise in prices for medicines and their high current cost.
4.2. Method
The government seeks to contain the rise in prices for medicines by regulating pricing in the pharmaceutical market and sets the task of reducing the “personal expenses” of the population for health care through the introduction of the MSHI system. Applying various methods to reduce the “out-of-pocket expense” of the population, the government must increase funding for the health care system, including drug provision. The government needs to increase funding for the health care system, without shifting this task to the population and private organizations.
H1 A hypothesis was put forward to empirically test the problem under study: it is assumed that an increase in government spending helps to reduce household spending on medicines.
To test this hypothesis, it is necessary to construct a multiple linear regression equation. The parameters of the multiple regression equation are estimated using the least squares method. When applied, a system of normal equations is constructed, the solution of which allows one to obtain estimates of the regression parameters.
To calculate the model, the national health accounts of the «Republican Center for Health Development» and data from the Committee on Statistics of the Ministry of National Economy of the Republic of Kazakhstan for 2010–2019 were used (Table ).
Table 2. The source data for 2010–2019 in the context of the analyzed parameters
Household pocket expenses will act as a dependent variable, to ensure statistical reliability of the results, we use data for 10 years and two factors: 1) government spending on medicines 2) average wages of people in Kazakhstan. It should be noted that in the Republic of Kazakhstan, the average salary is calculated to measure the income of citizens of Kazakhstan. Since the baseline indicator of government spending on medicines is subject to fluctuations, we have performed an exponential smoothing of this time series (smoothing parameter) in advance. Let us define the vector of estimates of the regression coefficients. According to the method of least squares, the vector s is obtained from the expression: s = (XTX)−1XTY
In the matrix, (XTX) the number 10 lying at the intersection of the 1st row and 1st column is obtained as the sum of the products of the elements of the 1st row of the XT matrix and the 1st column of the matrix X
As a result of calculations, we got the multiple regression equation:
Y = −64,442,640,908.902–0.4679X1 + 2,197,622.1486X2.
The result showed that an increase in government spending by 2,3 million US dollars (1 billion tenge) will lead to a decrease in “out-of-pocket expenses” by approximately of 1,1 million US dollars (468 million tenge); an increase in the average salary by 2.3 US dollars (1 thousand tenge) leads to an increase in the general “out-of-pocket expenses” of the population by an average of 5 245 thousand US dollars (2,197,622 million tenge).
After constructing the multiple linear regression equation, we evaluate the quality of the model by checking the significance of the regression equation (Fisher’s criterion).
The observed value of the Fisher criterion is Fobsrvd = 7.185
The critical value of the Fisher criterion at the level of significance and the number of degrees of freedom k1 = 2 and k2 = n-m-1 = 10–2—1 = 7, Fkp (2;7) = 4.74
Since the actual value is 7.185 > 4.74, the coefficient of determination is statistically significant and the regression equation is statistically reliable. shows the strong relationship between public spending on health care and private spending on medicines.
Figure 2. Dependence of public spending on health care and private spending on medicines.
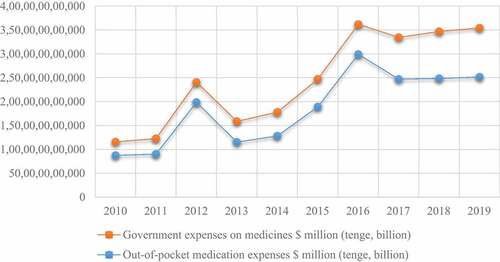
Graphical analysis shows that the empirical values are positively correlated (r = 0.78). This indicates a strong relationship between public spending on health and private spending on medicines.
Thus, an increase in government funding for the health care system, together with an effective health insurance system and drug pricing policies, can reduce health care costs for the population.
5. Conclusions
The study of the problem of “out-of-pocket expense” of the population for health care, in particular for medicines, made it possible to draw the following conclusions:
1) In this article, using a multiple regression equation shows that an increase in government spending will reduce the “out-of-pocket expense” of the population for medicines. The population spends a significant part of their budget on health care.
2) The government of Kazakhstan increases spending on health care every year, including spending on medicines. Various reforms are being adopted to reduce the “out-of-pocket expense” of the population on health care, such as the introduction of the MSHI system.
3) The high level of “out-of-pocket expenses” of the population indicates the need to attract additional sources of financing and reform health care through the financial flow management system.
4) It was revealed that the government needs to finance the health care system more, without shifting the responsibility of financing to organizations or to voluntary insurance in the course of the study. The health care deficit was 956.8 million US dollars for 2019, which indicates insufficient public funding.
5) Kazakhstan needs to reform the ERP system using the recommendations of the “Euripid Collaboration” and consider using other widely used methods for determining drug prices.
6) It should be noted that due to the devaluation of the national currency, government spending per capita in dollars does not increase significantly, despite the fact that a significant part of drugs and medical equipment is purchased abroad. So, in 2016, health spending per capita was 165 US dollars, 173 US dollars—in 2017, 171 US dollars—in 2018, 171 US dollars—in 2019.
Thus, Kazakhstan needs to bring the level of current expenditures up to international standards. The increase in total recurrent health care expenditures within the GVFMC and MSHI will reduce the level of private health care expenditures in the structure of recurrent health care expenditures. The government needs to invest more in health care, reducing the share of household spending. It is clear that well-thought-out policies to reduce private and personal spending can have a positive impact on the population and the health care system.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors

Yerik Bukatov
This study focuses on government measures to reduce household spending on health care in the Republic of Kazakhstan. Increased private spending on health, coupled with high levels of inequality, can lead to problems in accessing health services for low-income citizens. Therefore, every country needs an effective public policy aimed at controlling public and private spending on health care. In Kazakhstan, spending on medicines is the largest share of out-of-pocket spending on health care. Based on this, we conducted a sociological survey and found out what problems the population faces when buying medicines. A number of measures have also been proposed to help reduce private spending on health care.
Yerik Bukatov, Master of Economics in the direction of «Health Management and Economics». Senior Lecturer at the Department of Economic Theory and State and Local Government. General experience of scientific and pedagogical activity: 10 years. Area of expertise: management and economics of health care, public administration of medicines circulation.
Galiya Gimranova
Galiya Gimranova, Candidate of Sciences in Economics, professor, Dean of the Faculty of Economics, Management and Entrepreneurship, Karaganda University of Kazpotrebsoyuz. General experience of scientific and pedagogical activity: 28 years. Area of expertise: management and economics of health care, regional Economics and Management
This article is part of a research project on state regulation of drug circulation in the Republic of Kazakhstan.
References
- Baggio, S., Dupuis, M., Wolff, H., Bodenmann, P., & Bowen, M. (2018). Associations of lack of voluntary private insurance and out-of-pocket expenditures with health inequalities. Evidence from an international longitudinal survey in countries with universal health coverage. PloS one, 13(10), e0204666. https://doi.org/10.1371/journal.pone.0204666
- Baird, K. (2016). High out of pocket medical spending among the poor and elderly in nine developed countries. Health Services Research, 51(4), 1467–13. https://doi.org/10.1111/1475-6773.12444
- Boing, A. C., Bertoldi, A. D., Posenato, L. G., & Peres, K. G. (2014). The influence of health expenditures on household impoverishment in Brazil. Revista de Saúde Pública, 48(5), 797–807. https://doi.org/10.1590/S0034-8910.2014048005113
- Callander, E. J., Fox, H., & Lindsay, D. (2019). Out-of-pocket healthcare expenditure in Australia: Trends, inequalities and the impact on household living standards in a high-income country with a universal health care system. Health Economics Review, 9(1), 1–8. https://doi.org/10.1186/s13561-019-0227-9
- Elek, P., Takács, E., Merész, G., & Kaló, Z. (2017). Implication of external price referencing and parallel trade on pharmaceutical expenditure: Indirect evidence from lower-income European countries. Health Policy and Planning, 32(3), 349–358. https://doi.org/10.1093/heapol/czw133
- Espin, J., Rovira, J., & de Labry, A. O. (2011). Working paper 1: External price referencing–review series on pharmaceutical pricing policies and interventions. Geneva: World Health Organization and Health Action International, Andalusian School of Public Health. https://haiweb.org/wp-content/uploads/2015/08/ERP-final-May2011a1.pdf
- Grima, S., Spiteri, J. V., Jakovljevic, M., Camilleri, C., & Buttigieg, S. C. (2018). High out-of-pocket health spending in countries with a Mediterranean connection. Frontiers in Public Health, 6, 145. https://doi.org/10.3389/fpubh.2018.00145
- Hsu, J., Flores, G., Evans, D., Mills, A., & Hanson, K. (2018). Measuring financial protection against catastrophic health expenditures: Methodological challenges for global monitoring. International Journal for Equity in Health, 17(1), 1–13. https://doi.org/10.1186/s12939-018-0749-5
- Jakovljevic, M., Liu, Y., Cerda, A., Simonyan, M., Correia, T., Mariita, R. M., Kumara, A., Garcia, L., Krstic, K., Osabohien, R., Toan, T. R., Adhikari, C., Chuc, N., Khatri, R. B., Chattu, V., Wang, L., Wijeratne, T., Kouassi, E., Khan, H. N., & Varjacic, M. (2021). The Global South political economy of health financing and spending landscape – History and presence. Journal of Medical Economics, 24(sup 1), 25–33. https://doi.org/10.1080/13696998.2021.2007691
- Jakovljevic, M., Sugahara, T., Timofeyev, Y., & Rancic, N. (2020). Predictors of (in)efficiencies of healthcare expenditure among the leading asian economies - comparison of OECD and Non-OECD Nations. Risk Management and Healthcare Policy, 13, 2261–2280.https://doi.org/10.2147/RMHP.S266386
- Kawalec, P., Tesar, T., Vostalova, L., Draganic, P., Manova, M., Savova, A., Petrova, G., Rugaja, Z., Männik, A., Sowada, C., Pilc, A., Harsanyi, A., Inotai, A., Turcu-Stiolica, A., Gulbinovič, J., & Pilc, A. (2017). Pharmaceutical regulation in Central and Eastern European countries: A current review. Frontiers in Pharmacology, 8, 892. https://doi.org/10.3389/fphar.2017.00892
- Koch, S. F., Setshegetso, N., & Hotchkiss, D. (2020). Catastrophic health expenditures arising from out-of-pocket payments: Evidence from South African income and expenditure surveys. PloS One, 15(8), e0237217. https://doi.org/10.1371/journal.pone.0237217
- Lee, J. E., Shin, H. I., Do, Y. K., & Yang, E. J. (2016). Catastrophic health expenditures for households with disabled members: Evidence from the Korean health panel. Journal of Korean Medical Science, 31(3), 336. https://doi.org/10.3346/jkms.2016.31.3.336
- Mahumud, R. A., Sarker, A. R., Sultana, M., Islam, Z., Khan, J., & Morton, A. (2017). Distribution and determinants of out-of-pocket healthcare expenditures in Bangladesh. Journal of Preventive Medicine and Public Health, 50(2), 91. https://doi.org/10.3961/jpmph.16.089
- Orazbayev, S. K. (2013). On the issue of state regulation of prices for medicines. Bulletin of KazNPU, 150(2), 35–43. https://bulletin-pedagogy.kaznpu.kz/index.php/ped/issue/archive/2
- Pallegedara, A., & Grimm, M. (2018). Have out of pocket health care payments risen under free health care policy? The case of Sri Lanka. The International Journal of Health Planning and Management, 33(3), e781–e797. https://doi.org/10.1002/hpm.2535
- Persson, U., & Jönsson, B. (2016). The end of the international reference pricing system? Applied Health Economics and Health Policy, 14(1), 1–8. https://doi.org/10.1007/s40258-015-0182-5
- Pierre, A., & Jusot, F. (2017). The likely effects of employer-mandated complementary health insurance on health coverage in France. Health Policy, 121(3), 321–328. https://doi.org/10.1016/j.healthpol.2016.12.004
- Rémuzat, C., Urbinati, D., Mzoughi, O., El Hammi, E., Belgaied, W., & Toumi, M. (2015). Overview of external reference pricing systems in Europe. Journal of Market Access &. Health Policy, 3(1), 27675. https://doi.org/10.3402/jmahp.v3.27675
- Robinson, J. C., Panteli, D., & Ex, P. (2019). Reference pricing in Germany: Implications for US pharmaceutical purchasing. Issue Brief (Commonw Fund), 2019, 1–8. https://doi.org/10.26099/5xrf-wb19
- Ruggeri, K., & Nolte, E. (2013). Pharmaceutical pricing: The use of external reference pricing. Rand Health Quarterly, 3(2). https://rand.org/pubs/research_reports/RR240.html
- Salari, P., Di Giorgio, L., Ilinca, S., & Chuma, J. (2019). The catastrophic and impoverishing effects of out-of- pocket healthcare payments in Kenya, 2018. BMJ Global Health, 4(6), e001809. https://doi.org/10.1136/bmjgh-2019-001809
- Sriram, S., & Khan, M. M. (2020). Effect of health insurance program for the poor on out-of-pocket inpatient care cost in India: Evidence from a nationally representative cross-sectional survey. BMC Health Services Research, 20(1), 1–21. https://doi.org/10.1186/s12913-020-05692-7
- Stargardt, T., & Schreyögg, J. (2006). Impact of cross-reference pricing on pharmaceutical prices. Applied Health Economics and Health Policy, 5(4), 235–247. https://doi.org/10.2165/00148365-200605040-00005
- Tirgil, A., Dickens, W. T., & Atun, R. (2019). Effects of expanding a non-contributory health insurance scheme on out-of-pocket healthcare spending by the poor in Turkey. BMJ Global Health, 4(4), e001540. https://doi.org/10.1136/bmjgh-2019-001540
- Van Doorslaer, E., O’Donnell, O., Rannan-Eliya, R. P., Somanathan, A., Adhikari, S. R., Garg, C. C., Harbianto, D., Herrin, A. N., Huq, M. N., Ibragimova, S., & Zhao, Y. (2006). Effect of payments for health care on poverty estimates in 11 countries in Asia: An analysis of household survey data. The Lancet, 368(9544), 1357–1364. https://doi.org/10.1016/S0140-6736(06)69560-3
- Vandoros, S., & Stargardt, T. (2013). Reforms in the Greek pharmaceutical market during the financial crisis. Health Policy, 109(1), 1–6. https://doi.org/10.1016/j.healthpol.2012.08.016
- Vogler, S., Zimmermann, N., & Haasis, M. A. (2019). PPRI Report 2018-Pharmaceutical pricing and reimbursement policies in 47 PPRI network member countries. WHO Collaborating Centre for Pricing and Reimbursement Policies.
- World Health Organization. Global Health Expenditure Database. Retrieved from January 9, 2021, https://apps.who.int/nha/database
- Yfantopoulos, J. (2008). Pharmaceutical pricing and reimbursement reforms in Greece. The European Journal of Health Economics, 9(1), 87–97. https://doi.org/10.1007/s10198-007-0061-6
- Zagidullina, G. N., & Omirbaeva, B. S. (2019). Analysis of private spending on healthcare in Kazakhstan and proposals for their reduction. Policy Brief, Nur-Sultan: Republican Center for Health Development.
