
Abstract
Oval window atresia is often accompanied by malpositioned facial nerve, when inferiorly located facial nerve occupies the expected site of oval window, the ossicular chain reconstruction will always be abandoned. We report the case of a 12-year-old boy with one-side middle ear deformity and hearing loss. Under surgical exploration, the tympanic segment of facial nerve occupied the entire atresia plate, we created a hole on the bony basal turn of the cochlear immediately above the round window, a hand modeled titanium stapes prosthesis was used between the handle of malleus and cochleostomy opening. The audiogram showed an average hearing improvement of 36 dBHL three months later postoperatively. For the case with oval window atresia and inferiorly located facial nerve, cochleostomy could be an effective alternative fenestration site for ossicular chain reconstruction. The prosthesis shaping is always needed for better sound conduction.
Introduction
Congenital absence of the oval window (CAOW), a rare condition that causes conductive hearing loss [Citation1]. CAOW is often accompanied by malformed stapes and malpositioned facial nerve [Citation1]. Reconstructive surgery includes 2 major parts. First, the ossicular chain is restored with prostheses. Second, vestibulotomy is carried out to connect the ossicular chain with the inner ear. In most cases, tympanic segment of the facial nerve is slightly inferiorly located and covers small upper part of the expected position of the oval window, vestibulotomy could still be carried out on the vestibular atresia plate. When the facial nerve occupies the entire oval window, the ossicular chain reconstruction will always be abandoned. We report the use of a new fenestration site of cochleostomy for this situation and get good clinical result.
Case report
A 12-year-old boy was referred to us with 6-year history of hearing loss in the right ear. Hearing in the left ear was intact. Language skill and social development were normal. He reported no tinnitus, vertigo, or facial paralysis. There was no history of ear trauma or infection.
A physical workup revealed no craniofacial malformation, normal pinna, external auditory canal and tympanic membrane. Rinne test was negative on the right side. Weber test showed lateralization towards to the right. The tympanogram was the Ad type. Stapes reflex was absent on the right side. Tubomanometry test score was 10, indicating normal eustachian tube function. Audiogram revealed mean 50 dB air-bone gap (ABG). Upon high-resolution CT, the oval window was atresic, and the facial nerve was overlaying the vestibula with the stapes absent.
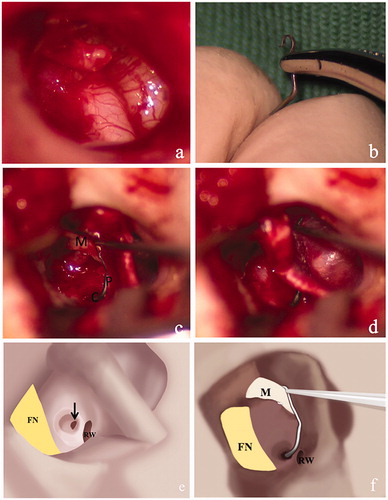
Under surgical exploration, the malleus was normal, the stapes was absent, the long process of the incus was significantly shorter than normal. Oval window was absent, and the tympanic segment of facial nerve occupied the entire atresia plate. Fallopian canal of the tympanic segment was completely dehiscent (Figure ). The incus was removed, then, the tympanic membrane was separated from the handle of malleus. A bur hole was created on the bony basal turn of the cochlear immediately above the round window using a microdrill at very low speed. A titanium stapes prosthesis (Spiggle & Theis; 0.4 mm X 7.00 mm) was modeled (Figure ) with two curves, and secured between the handle of malleus and cochleostomy opening (Figure ). The cochleostomy site was sealed by pieces of fat around the prosthesis. After replacing the tympano-meatal flap, the incision was closed.
Figure 1. The facial nerve occupied the atresia plate and part of the promontory (a, e) with dehiscence. The titanium stapes prothesss was shaped with two curves in different planes (b, f). The prothesis connected the scale tympani opening and the manubrium of malleus (c, f). The connection of the chain with 45° hook (d). I: incus; M: malleus; P: prothesis; C: cochleostomy; FN: facial nerve; RW: round window; TM: tympanic membrane. Black arrow: cochleostomy on the lateral wall of basal scala tympani.
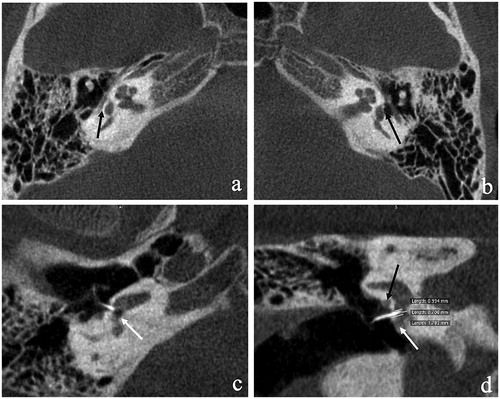
Examination with cone-beam CT 1 month later showed proper position of the stapes prosthesis and intact facial nerve (Figure ). The prosthesis entered the scala tympani along the superior margin of the round window (Figure ), with 0.994-mm protrusion into the inner ear. The end of prosthesis was 0.706 mm from the medial wall of the inner ear.
Figure 2. Cone-bean CT at 1 month after surgery. Axial section showing the absence of oval window (black arrow) with the facial nerve occupying the vestibular area in the affected side (a) vs. the normal oval window in the unaffected side (black arrow) (b). The stapes prothesis was inserted into the scala tympani along the superior margin of the round window (c) and the white arrow showed the round window niche. From the coronal image section, the length of protrusion was scaled (d).
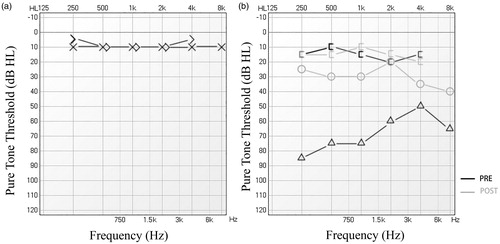
Three months later, an audiogram showed 13.75 dB ABG (50 dB prior to surgery; Figure ). Bone conduction threshold was not affected.
Figure 3. Audiogram at 3 months after surgery. Unaffected side (a). Hearing improvement in the affected side (b). black lines: prior to surgery. Grey lines: after surgery.
Discussion
The index patient in this case had type IV ab1 according to the Cremers classification [Citation1,Citation2]. Cases with normal hearing in the contralateral side could be managed with more conservative treatments, including hearing aids, osseointegrated auditory implant and vibrant sound bridge. Due to the extent of the anomalies, and particularly the malpositioning of the facial nerve, surgical reconstruction carries considerable risks. Oval window drill-out (OWD) procedure, first reported by Hough [Citation3] and Pou’s [Citation4], is the standard procedure for oval window atresia without malpositioning of the facial nerve. In a case series by Alarcon and Jahrsdoerfer [Citation5], OWD was aborted in 4 out of 17 cases (23.5%) after the middle ear exploration, 2 due to inferiorly located facial nerve, 1 due to over-angled and insecure prosthesis, and 1 due to close proximity of the basal turn to the planned fenestration site.
In the current case, the facial nerve was inferiorly located and occupied the expected site of the oval window, without bony fallopian canal for the tympanic segment. In a similar case, Hasegawa successfully reconstructed the ossicular chain using a fenestration of the scala vestibuli by drilling the site anterior to the oval window and below the facial nerve. A straight Teflon piston modified by reducing the circular portion (0.6 mm in diameter and 4.0 mm in length) [Citation6] was used between the new window and the malleus. In our case, we made the window immediately above the round window, so the staight piston is unsuitable beause of the angle; also, the preferred length of the Piston was different .Al-Mazrou and the colleagues [Citation7] reported three cases of labyrinthotomy under the facial nerve and achieved good long-term functional recovery; the straight prosthesis with 4.5 mm in length was used between incus and the new window in all these three cases because of the intact malleus and incus, no specific fenestration site was mentioned in the article. Liu and colleagues [Citation8] reported ossicular chain reconstruction with TORP (the total ossicular replacement prosthesis) using a scala tympani drill-out technique in 3 patients, and achieved >25dB hearing improvement in 2 patients. In our case, we drilled at the scala tympani and curved the Piston to suit to the reconstruction between the malleus and the new window.
In the current case, the fenestration was made immediately above the round window, using 1-mm and then 0.6-mm burr to drill the bony wall of the scala tympani and keep the endosteum intact. The stapes prosthesis was shaped with two angles to fit into the space between the manubium and the burr hole. At 3 months after surgery, ABG decreased from 50 dBHL to 13.75 dBHL. Bone conductive threshold was not affected, indicating minimal injury.
Conclusions
For the case with oval window atresia and inferiorly located facial nerve, when vestibular fenestration are not available, cochleostomy could be an effective alternative fenestration site for ossicular chain reconstruction. The procedure is safe with mediculous drilling and shaping the prosthesis is always needed for better sound conduction.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Teunissen EB, Cremers WR. Classification of congenital middle ear anomalies. Report on 144 ears. Ann Otol Rhinol Laryngol. 1993;102:606–612.
- Thomeer HG, Kunst HP, Cremers CW. Congenital stapes ankylosis associated with another ossicular chain anomaly: surgical results in 30 ears. Arch Otolaryngol Head Neck Surg. 2011;137:935–941.
- Hough JV. Malformations and anatomical variations seen in the middle ear during the operation for mobilization of the stapes. Laryngoscope. 1958;68:1337–1379.
- Pou JW. Congenital absence of the oval window. Report of two cases. Laryngoscope. 1963;73:384–391.
- de Alarcon A, Jahrsdoerfer RA, Kesser BW. Congenital absence of the oval window: diagnosis, surgery, and audiometric outcomes. Otol Neurotol. 2008;29:23–28.
- Hasegawa J, Kawase T, Hidaka H, et al. Surgical treatment for congenital absence of the oval window with facial nerve anomalies. Auris Nasus Larynx. 2012;39:249–255.
- Al-Mazrou KA, Bayazit YA. Labyrinthotomy or vestibulotomy in anatomic and congenital variations of the oval window and facial nerve. ORL J Otorhinolaryngol Relat Spec. 2012;74:320–324.
- Liu Y, Yang F. Scala tympani drill-out technique for oval window atresia with malformed facial nerve: a report of three cases. J Otol. 2015;10:154–158.