
Abstract
Two current major research topics concern the incorporation of flexible robotic endoscopy systems developed for natural-orifice translumenal endoscopic surgery (NOTES), primarily for the purpose of remote forceps operation, into endoscopic submucosal dissection (ESD) and other flexible endoscopic treatments and the use of robots for the manipulation of flexible endoscopes themselves with the aim of enabling the remote insertion of colonoscopes, etc. However, there are still many challenges that remain to be addressed; the ideal robotic endoscope has not yet been realized. This article reviews the ongoing developments and our own efforts in the area of flexible robotic endoscopy.
1. Introduction
Flexible endoscopy was originally developed for diagnostic purposes, but various treatment tools and devices have now been developed that permit its use in a wide range of therapeutic procedures. These therapeutic procedures are widely used owing to their low invasiveness and the fact that they can be performed by a single endoscopist in a relatively short time without the requirement for general anesthesia. The appearance of endoscopic submucosal dissection (ESD) as an endoscopic treatment for early gastric cancer, however, has dramatically increased the degree of difficulty and extended the time for a therapeutic procedure, and the limitations of operations using the current flexible endoscopy setup developed for diagnostic purposes are increasingly in evidence.[Citation1–5] Robotic surgery is now coming into use as a platform for natural-orifice transluminal endoscopic surgery (NOTES), and the current research is focused on improving the accuracy of tissue triangulation.[Citation6–10]
Two current major research topics concern the incorporation of flexible robotic endoscopy systems developed for NOTES, primarily for the purpose of remote forceps operation, into ESD and other flexible endoscopic treatments and the use of robots for the manipulation of flexible endoscopes themselves (endoscopic operation) with the aim of enabling the remote insertion of colonoscopes, etc.[Citation11] The authors are currently working in the latter field, but the development of meaningful robotic surgeries for ESD and other difficult flexible endoscopic treatment procedures will require platforms that combine both these areas if their intuitive operation is to become feasible. In this paper, we outline the limitations of flexible endoscopic treatments in ESD and the current status of flexible robotic endoscopy, together with a description of our own work, and we discuss future prospects in this field.
2. Limitations of flexible endoscopic treatment in ESD
Applying traction to or lifting up the luminal side of the mucosal surface in early gastrointestinal cancer is called ‘counter-traction’, and in ESD, the submucosa pulled up and exposed by this counter-traction must be patiently scraped away with an electric scalpel, as if carving with a chisel. Hemostasis is required each time a bleed occurs, and as the curved surface of the gastrointestinal tract cannot be dissected all at once, each time the dissection comes to a dead end, the right level of counter-traction must be reapplied and the angle of insertion of the electric scalpel is adjusted as the operation proceeds. If this is carried out using a single flexible endoscope, five hours or so may pass without the operator even noticing. A number of different treatment instruments and devices have been developed with the aim of resolving the rate-limiting steps in this procedure. Devices developed to provide effective counter-traction include mounted distal hoods,[Citation12] clips with thread,[Citation13–15] and grasping forceps passed through an externally mounted channel,[Citation16–19] but all of these devices have their own disadvantages and limitations. Distal hoods reduce the field of view, clips with thread become less effective in exerting counter-traction as dissection proceeds, and grasping forceps passed through an externally mounted channel can only be adjusted along the axis of the endoscope, and under some circumstances their presence may actually become a handicap.[Citation12–20] A wide range of electric scalpels has also been developed because of their advantage in improving the efficiency of resection, avoiding perforation and enabling extremely precise dissection.[Citation1–5,Citation21–30] The authors have also developed a number of treatment instruments to address these difficulties. Our hood-type ESD knife, a movable arc-shaped knife that attaches to the distal hood and thus enables the insertion of grasping forceps via the forceps channel, has been commercialized as the Kume irrigation cap-knife attachment (Create Medic Co., Ltd., Yokohama, Japan), but although it improves the efficiency of resection, it can only be used for lesions in certain locations, and since it is also difficult to control the depth of dissection, it is not widely used.[Citation31,Citation32] In ESD, using the principle of blunt dissection with a highly viscous substance, local injection of a highly viscous substance causes the spontaneous dissection of the submucosa, and we thought that, if the surrounding area were resected following such a local injection, then ESD would be complete, providing a revolutionary new method.[Citation33] However, although this method was successfully used in animal experiments on mini-pigs,[Citation34] its clinical application foundered due to problems with hemostasis.
A wide variety of treatment instruments and devices has been developed for use in ESD and other difficult endoscopic treatments, but these have been developed for the current flexible endoscopy platform, which was designed for diagnostic purposes, and their limitations are obvious.
3. Flexible robotic endoscopy with remote forceps operation
Most robotic endoscopy systems with remote forceps operation comprise flexible endoscopes with two arms mounted at the tip that can be used in the same way as both hands, and the aim is to enable these two arms to be used to achieve appropriate tissue triangulation and perform elemental procedures such as grasping, traction, incision, resection and hemostasis in an intuitive fashion. Some actual examples are described in the following sections.
3.1. Master and slave transluminal endoscopic robot (MASTER)
The National University of Singapore has played a central role in developing the MASTER.[Citation35–38] This is the only robot to be used to carry out the actual clinical dissection of ESD, which has been performed on five patients. Four of the lesions were located in the antrum and one in the greater curvature of the corpus, and their mean diameter was 2.2 cm (range 1.5–3 cm). The mean operating time was 39.2 minutes (range 26–68 minutes).[Citation39] Robotic forceps with seven degrees of freedom are fitted to two Olympus GIF-2T240 forceps channels, and these are operated remotely by a full-time operator using a dedicated master device electronically driven by an actuator, while another operator manipulates the endoscope itself in the normal way. However, the only procedure for which the MASTER has yet been used is the dissection of the submucosa, with marking and surrounding incision being performed with a regular endoscope, and in all five cases it was necessary to switch among three different endoscopes.
3.2. Anubiscope®
The Anubiscope® is a platform jointly developed by the Research Institute against Digestive Cancer and Karl Storz (Tuttlingen, Germany), with two arms fitted to the tip of an endoscope.[Citation40] Its feature is that the tip takes the form of a streamlined capsule when the endoscope is inserted into the gastrointestinal tract, with the central part opened up by splitting into two parts only after the endoscope has been advanced into the tract to enable the two arms stored inside it to be operated. In terms of industrial design, this is a beautiful platform. It has been successfully used for colorectal ESD in animals,[Citation41] and a case study of its clinical use for gall bladder extraction by transvaginal NOTES has been reported.[Citation42]
3.3. ENDOSAMURAI™
The ENDOSAMURAI™ (), developed by Olympus Medical Systems (Tokyo, Japan), is a platform with two arms fitted to the tip of an endoscope that includes forceps channels in addition to the endoscope itself and its two arms, meaning that, if necessary, three different sets of forceps can be used replaceably at the same time. Like the MASTER, it requires a minimum of two people to perform a procedure, one operator who manipulates the two arms full-time and another endoscopist to carry out conventional operation of the endoscope itself. Its manual operation means that it becomes harder to operate when the inserted part of the endoscope curves, and the fact that it is overall somewhat larger in size than the MASTER also affects the precision with which it can be operated, but it does have the advantage of making it possible to switch forceps. However, it was originally developed for use in NOTES, and although it has undergone improvement in the years that have elapsed since its first appearance, its clinical is yet to be reported, with reports only describing its ease of operability during laparoscopy compared with the conventional forceps [Citation43] and validation of its use for endoscopic full-thickness dissection by animal experiments.[Citation44]
Figure 1. (a) The system of the ENDOSAMURAI™ (by courtesy of Olympus Medical Systems, Tokyo, Japan). (b) The insertion part of the ENDOSAMURAI™ (by courtesy of Olympus Medical Systems, Tokyo, Japan).

3.4. The direct drive endoscopic system (DDES)
The DDES is a platform developed by Boston Scientific Systems (Natick, MA) that comprises two arms fitted to the tip of an overtube, and since a regular endoscope is inserted through this tube, it has the advantage that the movements of the arms are not synchronized with that of the endoscope.[Citation45] It requires a minimum of two people to perform a procedure, one operator who manipulates the two arms full-time and another endoscopist to carry out conventional operation of the endoscope itself. The forceps on the two arms may be selected from several different types, including grasping and scissor forceps, but what is revolutionary about this platform is that it also enables suturing with a needle carrier.[Citation46]
3.5. Others
The Cobra system is a platform fitted with three arms, but since it does not permit forceps to be changed, it must be withdrawn and reinserted, similarly to the DDES.[Citation47] The ViaCath system is a flexible shaft forceps system with seven degrees of freedom with two shafts running through an overtube that was developed for use in laparoscopic surgery.[Citation9]
4. Flexible robotic endoscopy platforms for assisted endoscope operation
The robotic platforms in this area have chiefly been developed to assist with the operations involved in colonoscope insertion. They mainly comprise robotic platforms that incorporate inchworm-like movements or techniques adapted from small intestine balloon endoscopy into the insertion procedure, but this type can only be used for intestinal operations. However, other types that are not based on these techniques but permit free insertion into the large intestine have the potential for use in upper gastrointestinal endoscopy or laparoscopy, and we have also developed a flexible robotic endoscopy platform of this type.
4.1. Flexible robotic endoscopy platforms that incorporate inchworm-like movements or techniques from small intestine balloon endoscopy into the insertion procedure
The Aeroscope is a colonoscopic platform developed by GI View (Ramat Gan, Israel) that is inserted while an airtight space is created by means of the computer-controlled inflation of proximal and distal balloons, although the insertion of the scope itself is a manual operation.[Citation48–50] Endotics is a dedicated colonoscopic platform developed by Era ENDOSCOPY S.R.L (Peccioli, Italy) that enables insertion via an inchworm-like mechanism entailing the repeated anchoring and release of the scope through suction of the colorectal mucosa. Both of these platforms are already in clinical use, but they are yet to match the track record of conventional endoscopes.[Citation51] Other such systems include the Invendiscope (Invendo Medical GmbH, Germany) [Citation52,Citation53] and the Neoguide (Intuitive Surgical, Sunnyvale, CA).[Citation54]
4.2. The endoscopic operation robot (EOR)
To enable endoscopic treatment to be carried out robotically, in addition to the flexible robotic endoscopy platforms with remote forceps operation described in the further section, it will also be necessary to enable the robotic performance of operations such as bringing the instruments into close proximity with the treatment target and adjusting the angle of advance, which cannot be managed by means of access to the treatment site and forceps operation alone. Robotic operation only of the forceps, leaving manipulation of the scope itself dependent on conventional manual operation, places restrictions on the development of this field, and we have therefore developed the EOR with the initial aim of enabling all scope operations to be performed remotely.
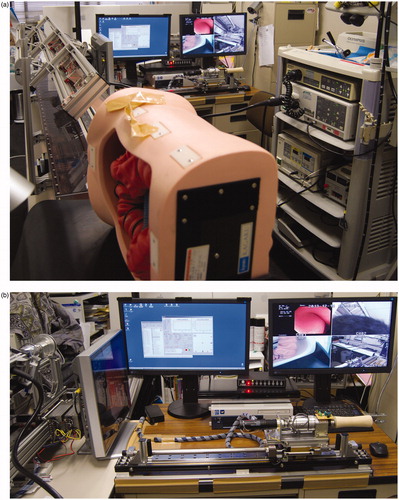
As shown in , Version 1 consists of five units: a main unit with a conventional flexible endoscope attached (a), an operating device (b), an air feed and suction adjuster (c), a conventional light source (d) and a suction device (e). The operating unit (b) is equipped with a monitor and two joysticks, with the right joystick used to operate the vertical and horizontal angle knobs of the scope and the left joystick to manipulate the rotation and advance/withdrawal of the scope, while three foot switches are used to control the air feed/intake and lens irrigation, creating a flexible endoscopic remotely operated robotic platform capable of the completely remote operation of a flexible endoscope.[Citation55,Citation56] Version 2 () resolved two problems related to the transmission of torque, and since in Version 1, the drive system was attached directly to the endoscope, and it did not include a safety mechanism for its removal and conventional operation in the event of an emergency, Version 2 was fitted with a mechanism for its attachment and removal, permitting the easy attachment and removal of a conventional endoscope.[Citation57] Version 3 () was developed as a master–slave robot incorporating two-way force feedback to allow the operator to feel the responsiveness of the scope during insertion, enabling all the operations of a flexible endoscope to be performed with one hand. In a colonoscope insertion training model, the mean time for insertion as far as the cecum was 1 minute 58 seconds, and the platform provided the intuitive sense of insertion required for clinical use.[Citation58]
Figure 2. The EOR version 1.
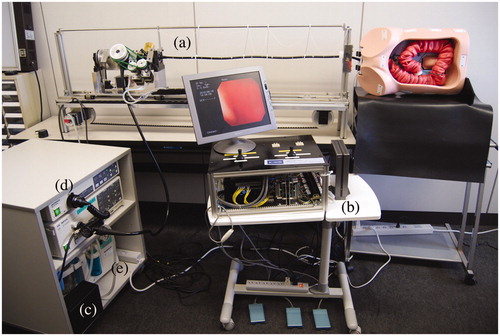
Figure 3. The EOR version 2.
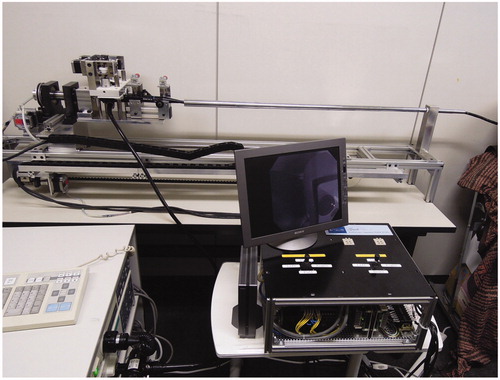
Figure 4. (a) The system of the EOR version 3. (b) The master device of the EOR version 3.
5. Future prospects
Editorial review of the EOR ver. 3 appeared in ‘Endoscopy’.[Citation59] The editorial made three points to which we would like to respond with our current thoughts. First, it was stated that the slave unit is too large. However, there are two difficulties in reducing the size (e.g. by adopting a system to wind the long insertion portion on a drum) of EOR ver. 3, which is used in conjunction with existing flexible endoscopes: (1) When inserting existing colonoscopes, avoidance of loop formation as much as possible while maintaining the axis makes insertion smoother and reduces patient discomfort. Having no excessive bending in the scope being inserted is important for maintaining this manipulability. This is especially important in the EOR, which senses bidirectional force with the aim of maximum elimination of force aspects other than scope manipulation. (2) In haptic sensation, it is also easy to pick up simultaneous surrounding vibrations or other forces; thus, the system needs to have adequate rigidity and weight. This makes heaviness and bulkiness, a problem that is difficult to avoid. A commercial flexible endoscope that has been pulled straight has to be mounted in the EOR, and the bulkiness is to some extent unavoidable. Second, switching off the circuit because of manipulation restrictions due to the 60 cm length of the master unit was suggested to be a drawback. However, this was because the master manipulation distance and the slave manipulation distance were set 1 to 1. If the motion scale is changed, for example to 1 to 2, the slave travel distance can be changed to 120 cm. The setting was made with the thought that, with the operator in a sitting position, the limit to manipulation of the master unit is about 60 cm. Third, the authors stated that use of a device such as the Novint Falcon haptic device on the existing master unit could help simplify the unit and reduce the cost.[Citation60] We tried using something similar, the commercial Phantom, but the force [N] and rotational torque [Nm] during manipulation were excessive. Moreover, even assuming that manipulations are within the range limit in the specifications, these existing master units are useful in that haptic feedback can be felt. We think that the greatest significance of remote flexible endoscope manipulations is in the intuitiveness of the manipulations, and that a unique master unit configuration is needed to achieve this intuitiveness. With the EOR, it is assumed that an existing flexible endoscope will be attached; if a new, EOR-dedicated scope is developed, several of these problems will be resolved. For now, we are putting all of our efforts into achieving the target performance for the EOR, after which we would like to work on bringing the cost down and making it more compact, which are crucial points for its general use. The da Vinci (Intuitive Surgical, Sunnyvale, CA) has been widely adopted as a robotic treatment system despite its high cost for three reasons. These are: (a) filtering functions that eliminate physiological tremor of the operator’s hands; (b) motion scaling functions that enable very precise treatment; and (c) three-dimensional (3D) imaging on 3D monitors. These distinctive functions provide an ease of operation that cannot be exceeded even by the operator’s effort and improvement, permitting surgery to be carried out with unprecedented precision.[Citation61] For a flexible endoscopic robotic system to be widely used, it must therefore provide a similar level of superiority commensurate with its cost to that of the da Vinci.
Flexible robotic endoscopy platforms currently fall far short of the da Vinci. Their clinical use does not provide results superior to those of conventional treatment, and animal experiments only illustrate the types of procedures favorable to the device concerned. The lesions for which ESD was performed with the MASTER were at sites and of sizes that could be dealt with during the time normally taken by an endoscopist accustomed to performing ESD, and they were easy lesions that could be treated completely with very little difficulty. If a robotic system is no more than comparable with current procedures, it offers no advantages. They will have to demonstrate their superiority by enabling large lesions, which would normally require hours to remove under high tension and entail the risk of perforation or other mishap, to be dealt with completely in a short time under the right level of tension by means of intuitive, easy operation requiring no training. Unless they also possess the versatility to be adapted for use in treatment procedures that will become more widely performed in the future, such as therapeutic pancreatobiliary endoscopy and endoscopic full-thickness resection, single-port laparoscopic surgery and NOTES, their cost may also be prohibitive.
Many issues remain before intuitive, highly precise operation can be achieved.[Citation7,Citation11] If the precision of forceps arm operation is to be improved, the joints must be given more degrees of freedom, but this will make the master device more complicated and come at the expense of intuitive operation. The length of each arm, the positions of its joints, the distance reached by each arm and the operating field to which it can be deployed all have major effects on how intuitive and easily operated the system is. Its operability will be impeded if the arms are either too long or too short, or if the operating field is too wide or too narrow. It must be able to treat any lesion, of whatever size and in whatever location. To maintain the precision with which the forceps arms can be operated, the area of deployment of a single arm by itself is limited, and it must also be possible for the operation of the endoscope itself to be synchronized. As the fundamental limitation of current endoscopic treatment is that everything has to be synchronized with the operation of a single endoscope, excessive synchronization is putting the cart before the horse. Many other issues also remain to be overcome, such as studies of the materials required to achieve this and their durability, the tracking ability of cameras for visual confirmation of the operating field, and the necessity or otherwise of 3D conversion. The right direction to pursue is to resolve these issues and restore procedures that are of low invasiveness and can be performed by a single endoscopist in a relatively short time without the requirement for general anesthesia. The key to achieving this will lie in developing ‘‘intuitive’’ robotic systems that reflect the sense of scope operation developed by endoscopists over many years.
Disclosure statement
Author has no conflict of interest.
Funding
This work was supported by Grant-in-Aid for Scientific Research [MEXT KAKENHI: 23500573 and 263500554] and Grant of the Princess Takamatsu Cancer Research Fund [13-24505].
References
- Muto M, Miyamoto S, Hosokawa A, et al. Endoscopic mucosal resection in the stomach using the insulated tip needle knife. Endoscopy. 2005;37:178–182.
- Oka S, Tanaka S, Kaneko I, et al. Advantage of endoscopic submucosal dissection compared with EMR for early gastric cancer. Gastrointest Endosc. 2006;64:877–883.
- Ono H, Kondo H, Gotoda T, et al. Endoscopic mucosal resection for treatment of early gastric cancer. Gut. 2001;48:225–229.
- Kume K. Endoscopic mucosal resection and endoscopic submucosal dissection for early gastric cancer: current and original devices. World J Gastrointest Endosc. 2009;1:21–31.
- Kume K. Endoscopic therapy for early gastric cancer: standard techniques and recent advances in ESD. World J Gastroenterol. 2014;20:6425–6432.
- Swanstrom LL. NOTES: platform development for a paradigm shift in flexible endoscopy. Gastroenterology. 2011;140:1150–1154.
- Arkenbout EA, Henselmans PW, Jelínek F, et al. A state of the art review and categorization of multi-branched instruments for NOTES and SILS. Surg Endosc. 2015;29:1281–1296.
- Shalkh SN, Thompson CC. Natural orifice translumenal surgery: flexible platform review. World J Gastrointest Surg. 2010;2:210–216.
- Yeung BP, Gourlay T. A technical review of flexible endoscopic multitasking platforms. Int J Surg. 2012;10:345–354.
- Kiblbansky D, Rothstein RI. Robotics in endoscopy. Curr Opin Gastroenterol. 2012;28:477–482.
- Yeung BP, Chiu PW. Application of robotics in gastrointestinal endoscopy: a review. World J Gastroenterol. 2016;22:1811–1825.
- Yamamoto H, Kawata H, Sunada K, et al. Successful en-bloc resection of large superficial tumors in the stomach and colon using sodium hyaluronate and small-caliber-tip transparent hood. Endoscopy. 2003;35:690–694.
- Jeon WJ, You IY, Chae HB, et al. A new technique for gastric endoscopic submucosal dissection: peroral traction-assisted endoscopic submucosal dissection. Gastrointest Endosc. 2009; 69:29–33.
- Ota M, Nakamura T, Hayashi K, et al. Usefulness of clip traction in the early phase of esophageal endoscopic submucosal dissection. Dig Endosc. 2012;24:315–318.
- Li CH, Chen PJ, Chu HC, et al. Endoscopic submucosal dissection with the pulley method for early-stage gastric cancer (with video). Gastrointest Endosc. 2011;73:163–167.
- Yanagida N. Endoscopic submucosal dissection (two-point fixed ESD) for early esophageal cancer. Dig Endosc. 2009;21:176–179.
- Motohashi O. Two-point fixed endoscopic submucosal dissection in rectal tumor (with video). Gastrointest Endosc. 2011;74:1132–1136.
- Okamoto K, Okamura S, Muguruma N, et al. Endoscopic submucosal dissection for early gastric cancer using a cross-counter technique. Surg Endosc. 2012;26:3676–3681.
- Teoh AY, Chiu PW, Hon SF, et al. Ex vivo comparative study using the Endolifter® as a traction device for enhancing submucosal visualization during endoscopic submucosal dissection. Surg Endosc. 2013;27:1422–1427.
- I Imaeda H, Hosoe N, Kashiwagi K, et al. Advanced endoscopic submucosal dissection with traction. World J Gastrointest Endosc. 2014;6:286–295.
- Hirao M, Masuda K, Asanuma T, et al. Endoscopic resection of early gastric cancer and other tumors with local injection of hypertonic saline-epinephrine. Gastrointest Endosc. 1988;34:264–269.
- Ohkuwa M, Hosokawa K, Boku N, et al. New endoscopic treatment for intramucosal gastric tumors using an insulated-tip diathermic knife. Endoscopy. 2001;33:221–226.
- Miyamoto S, Muto M, Hamamoto Y, et al. A new technique for endoscopic mucosal resection with an insulated-tip electrosurgical knife improves the completeness of resection of intramucosal gastric neoplasms. Gastrointest Endosc. 2002;55:576–581.
- Gotoda T. A large endoscopic resection by endoscopic submucosal dissection procedure for early gastric cancer. Clin Gastroenterol Hepatol. 2005;3:S71–S73.
- Oyama T, Tomori A, Hotta K, et al. Endoscopic submucosal dissection of early esophageal cancer. Clin Gastroenterol Hepatol. 2005;3:S67–S70.
- Yahagi N, Fujishiro M, Kakushima N, et al. Endoscopic submucosal dissection for early gastric cancer using the tip of an electro-surgical snare (thin type). Dig Endosc. 2004;16:34–38.
- Toyonaga T, Nishino E, Dozaiku T, et al. Management to prevent bleeding during endoscopic submucosal dissection using the flush knife for gastric tumor. Dig Endosc. 2007;19:S14–S18.
- Kawahara Y, Takenaka R, Okada H. Risk management to prevent perforation during endoscopic submucosal dissection. Dig Endosc. 2007;19:S9–S13.
- Akahoshi K, Akahane H, Murata A, et al. Endoscopic submucosal dissection using a novel grasping type scissors forceps. Endoscopy. 2007;39:1103–1105.
- Honma K, Otaki Y, Sugawara M, et al. Efficacy of novel SB knife Jr examined in a multicenter study on colorectal endoscopic submucosal dissection. Dig Endosc. 2012;24:117–120.
- Kume K, Yamasaki M, Kanda K, et al. Endoscopic submucosal dissection using a novel irrigation hood-knife. Endoscopy. 2005;37:1030–1031.
- Kume K, Yamasaki M, Kanda K, et al. Grasping-forceps-assisted endoscopic submucosal dissection using a novel irrigation cap-knife for large superficial early gastric cancer. Endoscopy. 2007;39:566–569.
- Yamasaki M, Kume K, Kanda K, et al. A new method of endoscopic submucosal dissection using submucosal injection of jelly. Endoscopy. 2005;37:1156–1157.
- Yamasaki M, Kume K, Yoshikawa I, et al. A novel method of endoscopic submucosal dissection with blunt abrasion by submucosal injection of sodium carboxymethylcellulose: an animal preliminary study. Gastrointest Endosc. 2006;64:958–965.
- Ho KY, Phee SJ, Shabbir A, et al. Endoscopic submucosal dissection of gastric lesions by using a Master and Slave Transluminal Endoscopic Robot (MASTER). Gastrointest Endosc. 2010;72:593–599.
- Wang Z, Phee SJ, Lomanto D, et al. Endoscopic submucosal dissection of gastric lesions by using a master and slave transluminal endoscopic robot: an animal survival study. Endoscopy. 2012;44:690–694.
- Chiu PW, Phee SJ, Wang Z, et al. Feasibility of full-thickness gastric resection using master and slave transluminal endoscopic robot and closure by Overstitch: a preclinical study. Surg Endosc. 2014;28:319–324.
- Lomanto D, Wijerathne S, Ho LK, et al. Flexible endoscopic robot. Minim Invasive Ther Allied Technol. 2015;24:37–44.
- Phee SJ, Reddy N, Chiu PW, et al. Robot-assisted endoscopic submucosal dissection is effective in treating patients with early-stage gastric neoplasia. Clin Gastroenterol Hepatol. 2012;10:1117–1121.
- Dallemagne B, Mareacaux J. The ANUBISTM project. Minim Invasive Ther Allied Technol. 2010;19:257–261.
- Diana M, Chung H, Liu KH, et al. Endoluminal surgical triangulation: overcoming challenges of colonic endoscopic submucosal dissections using a novel flexible endoscopic surgical platform: feasibility study in a porcine model. Surg Endosc. 2013;27:4130–4135.
- Perretta S, Dallemagne B, Barry B, et al. The ANUBISCOPE® flexible platform ready for prime time: description of the first clinical case. Surg Endosc. 2013;27:2630
- Spaun GO, Zheng B, Swanstrom LL. A multitasking platform for natural orifice translumenal endoscopic surgery (NOTES): a benchtop comparison of a new device for flexible endoscopic surgery and a standard dual-channel endoscope. Surg Endosc. 2009;23:2720–2727.
- Ikeda K, Sumiyama K, Tajiri H, et al. Evaluation of a new multitasking platform for endoscopic full-thickness resection. Gastrointest Endosc. 2011;73:117–122.
- Spaun GO, Zheng B, Martinec DV, et al. Bimanual coordination in natural orifice transluminal endoscopic surgery: comparing the conventional dual-channel endoscope, the R-Scope, and a novel direct-drive system. Gastrointest Endosc. 2009;69:39–45.
- Thompson CC, Ryou M, Soper NJ, et al. Evaluation of a manually driven, multitasking platform for complex endoluminal and natural orifice transluminal endoscopic surgery applications (with video). Gastrointest Endosc. 2009;70:121–125.
- Bardao SJ, Swanstrom L. Development of advanced endoscopes for natural orifice transluminal endoscopic surgery (NOTES). Minim Invasive Ther Allied Techol. 2006;15:378–383.
- Vucelic B, Rex D, Pulanic R, et al. The aer-o-scope: proof of concept of a pneumatic, skill-independent, self-propelling, self-navigating colonoscope. Gastroenterology. 2006;130:672–677.
- Pfeffer J, Grinshpon R, Rex D, et al. The Aer-O-Scope: proof of the concept of a pneumatic, skill-independent, self-propelling, self-navigating colonoscope in a pig model. Endoscopy. 2006;38:144–148.
- Arber N, Grinshpon R, Pfeffer J, et al. Proof-of-concept study of the Aer-O-Scope omnidirectional colonoscopic viewing system in ex vivo and in vivo porcine models. Endoscopy. 2007;39:412–417.
- Tumino E, Sacco R, Bertini M, et al. Endotics system vs colonoscopy for the detection of polyps. World J Gastroenterol. 2010;16:5452–5456.
- Rösch T, Adler A, Pohl H, et al. A motor-driven single-use colonoscope controlled with a hand-held device: a feasibility study in volunteers. Gastrointest Endosc. 2008;67:1139–1146.
- Groth S, Rex DK, Rösch T, et al. High cecal intubation rates with a new computer-assisted colonoscope: a feasibility study. Am J Gastroenterol. 2011;106:1075–1080.
- Eickhoff A, van Dam J, Jakobs R, et al. Computer-assisted colonoscopy (the NeoGuide Endoscopy System): results of the first human clinical trial (‘PACE study’). Am J Gastroenterol. 2007;102:261–266.
- Kume K, Kuroki T, Sugihara T, et al. Development of a novel endoscopic manipulation system: the endoscopic operation robot. World J Gastrointest Endosc. 2011;3:145–150.
- Kume K, Kuroki T, Shingai M, et al. Endoscopic submucosal dissection using the endoscopic operation robot. Endoscopy. 2012;44:E399–E400.
- Kume K, Kuroki T, Shingai M. Development of a novel endoscopic manipulation system: the endoscopic operation robot ver. 2. Hepatogastroenterology. 2015;62:843–845.
- Kume K, Sakai N, Goto T. Development of a novel endoscopic manipulation system: the endoscopic operation robot ver. 3. Endoscopy. 2015;47:815–819.
- Li Z, Chiu PW. Will the robot take over endoscopy? Endoscopy. 2015;47:773–774.
- Li Z, Feiling J, Ren H, et al. A novel teleoperated flexible robot targeted for minimally invasive surgery. Engineering. 2015;1:74–79.
- Weissman JS, Zinner M. Comparative effectiveness research on robotic surgery. JAMA. 2013;309:721–722.