
Abstract
Background: The diode laser was utilized in soft tissue incision of oral surgery based on the photothermic effect. The contradiction between the ablation efficiency and the thermal damage has always been in diode laser surgery, due to low absorption of its radiation in the near infrared region by biological tissues. Fiber-optic thermal converters (FOTCs) were used to improve efficiency for diode laser surgery. The purpose of this study was to determine the photothermic effect by the temperature and residual laser energy on film FOTCs.
Methods: The film FOTC was made by a distal end of optical fiber impacting on paper. The external surface of the converter is covered by a film contained amorphous carbon. The diode laser with 810 nm worked at the different rated power of 1.0 W, 1.5 W, 2.0 W, 3.0 W, 4.0 W, 5.0 W, 6.0 W, 7.0 W, 8.0 W in continuous wave (CW)and pulse mode. The temperature of the distal end of optical fiber was recorded and the power of the residual laser energy from the film FOTC was measured synchronously. The temperature, residual power and the output power were analyzed by linear or exponential regression model and Pearson correlations analysis.
Results: The residual power has good linearity versus output power in CW and pulse modes (R2 = 0.963, P < 0.01 for both). The temperature on film FOTCs increases exponentially with adjusted R2 = 0.959 in continuous wave mode, while in pulsed mode with adjusted R2 = 0.934. The temperature was elevated up to about 210 °C and eventually to be a stable state. Film FOTCs centralized approximately 50% of laser energy on the fiber tip both in CW and pulsed mode while limiting the ability of the laser light to interact directly with target tissue.
Conclusions: Film FOTCs can concentrate part of laser energy transferred to heat on distal end of optical fiber, which have the feasibility of improving efficiency and reducing thermal damage of deep tissue.
Introduction
The diode laser has garnered numerous reports and applications in soft tissue surgery [Citation1–4]. The photothermic conversion of energy can carry out soft tissue incisions and excisions. Diode laser application in soft tissue surgery was found beneficial effect for clinical observations. The diode laser has excellent performance in intraoperative and postoperative due to the sufficient cutting abilities, the good coagulation effect and the extremely small zone of thermal necrosis to surrounding tissues [Citation5]. Diode laser with wavelengths ranging from 810 to 980 nm in a continuous or pulsed mode was used as a possible modality for soft tissue surgery. It has been proven as an alternative solution to conventional electro-surgery and scalpel, according to economic and ergonomic consideration in comparison to other devices [Citation6]. They can be used in a continuous or pulsed mode of operation through contact or noncontact application on tissues according to the clinical approach and treatment method [Citation7]. In the noncontact mode, light of Nd:YAG (λ = 1064 nm) and diode (λ = 830 nm or 940 nm) lasers produces coagulation zones within the depth of the target tissue [Citation8–10]. Actually a close contact to the tissue is difficult to be avoided during the laser surgery, and contact treatment might provide for a precise and effective tissue reduction in a bloodless way because of its high ablation and coagulation capabilities [Citation11].
Diode laser radiation is widely used for contact surgery. However, it always took surgeons much time in clinic to excise soft tissue with the diode laser, due to low absorption of its radiation in the near infrared region by biological tissues [Citation12–14]. Surgeons had to enhance the output power of the diode lasers, but the risk of thermal damage increases substantially. Diode laser radiation by a distal end containing an photothermal converter is a way to improve the efficiency of cutting or ablating soft tissue and has less collateral thermal injury, this type of tissue-cutting is called hot tip surgery [Citation15]. The technique (‘hot tip’) to heat a metal probe by laser radiation was used for arterial recanalization [Citation16] and laser angioplasty [Citation17,Citation18] since the early 1980 s. The earliest publication of metallic tips on the end of quartz fiber was described for pulmonary carcinoma treatment [Citation19]. Contact surgery with optically driven hot-tip fiber accessories can enhance surgical precision and reduce collateral thermal injury when cutting or ablating soft tissue [Citation20]. ‘Black’ ball-shaped fiber tips were proved safe and effective in a neuro-endoscopic procedures [Citation21].
In Verdaasdonck et al.’s study, a special laser catheter was developed with an atraumatic ball-tip which was pretreated with a layer of carbon particles absorbing 90% of the laser energy. In recent years, Belikov and Skripnik [Citation15,Citation22–25] had worked on some pioneering researches of fiber-optic thermal converter. FOTCs contain microbubbles or carbon film that transfer the incident laser beam to heat to improve heat efficiency in laser surgery. The thermal and optical modelling and properties of different types (film and volumetric) thermo-optical converters were confirmed in Ref. [Citation23,Citation24]. The volumetric FOTC absorbed almost energy and convert to higher temperature than film FOTC on the tip. It is seen that the higher temperature a converter has, the more efficient it has in destroying soft biological tissue.
However, the thin-film FOTC has very high efficiency and is convenient during diode laser surgery. From the surgeons’ feedback, excising the soft tissue had tidy wound, little carbonization area and thermal damage by using a thin-film FOTC that the temperature didn’t have to be too hot. Temperature of fiber tips and power of residual radiation are vital parameters for physicians to carry on surgery. In this work, we conducted a study of photothermal effect of the film FOTC. A film converter is created by 810 nm diode laser radiation on paper. A carbonized film adhered to the distal end of the optical fiber absorbs light that leads to photothermic effect, which heats the distal end. A fraction of incident laser still radiates. Photothermic effect is determined by the temperature at the distal end of the fiber and residual power of laser radiation. We tried to explore the temperature on the distal end of fiber and the photothermic efficiency.
Materials and methods
The diode laser device (Pilot, CAO Group, Inc., USA) with a wavelength of λ = (810 ± 10) nm was used in this study. The laser radiation was delivered via bare-ended quartz fibers in two modes: continuous wave (CW) and pulsed mode. The diode laser device carried a fiber management system with patent retractable fiber box. The fiber core diameter was 320 ± 5 μm. The prepared laser power monitor (SOLO2, Power & Energy Monitor, GENTEC-EO) was used for monitoring residual power from the fiber tip. Infrared thermometer (FLIR i7, USA) was selected to measure the temperature of the distal end, which can automatically measure the highest temperature, store images and data with 100 × 100 resolutions and <0.1 °C sensitivity.
The film FOTC was made as follow: a distal end of optical fiber at low output power of 0.5 W was impacted on the articulating paper vertically; the distal fiber end face was in contact with the surface of the paper. The distal end of optical fiber combusts fiercely in air, generating light and heat energy, until burned through the paper. The extremity of the optical fiber was observed to be blackened. The external surface of the converter is covered by a film contained amorphous carbon [Citation22,Citation26]. shows a film fiber-optic thermal converter was heated by 810 nm laser at low output power of 1 W.
Figure 1. The heat of a film FOTC at laser power of 1 W.
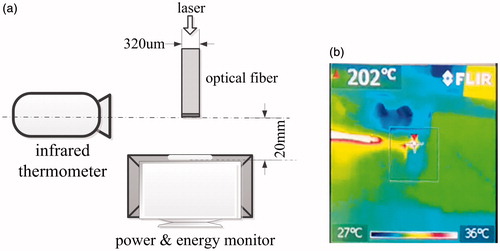
To obtain more reproducible measurements, the distal end of optical fiber was cut and kept bare before each of the determination. The fiber was kept horizontally with 20 mm from the laser power monitor (). In the meantime, the temperature of the distal end of optical fiber was measured and record by the infrared thermometer (). The data of temperature and residual power were acquired eventually. Additionally, common laser safety instructions were followed carefully during the laser procedure. All investigators wore medical masks (0.1 micron) and laser safety glasses. The ambient temperature was kept about 28 °C during the experiments.
Figure 2. Scheme of the experimental measurement for the infrared thermometer and laser power monitor.
The rated power was at a series of 1.0 W, 1.5 W, 2.0 W, 3.0 W, 4.0 W, 5.0 W, 6.0 W, 7.0 W, 8.0 W in CW and pulsed mode. Every emission lasted for 20 seconds. A temperature value and a value of residual power were acquired every second simultaneously. At the previous stage, carbon particles on the surface burn fiercely and then microbubbles are gradually formed and distributed on the converter surface. So, the data was rising and was unstable for about 3–5 s. In the researches of Belikov and Skrypnik [Citation23,Citation25], their figures also reflects a unstable stage. After removing the data from unstable stages, we got about 15 valid values of the temperature and residual power. The values were averaged and the mean values were regarded as the results corresponding to the output power. The experiment was repeated for three times. To highlight the FFOTC effect, a control experiment with a ‘clear tip’ was conducted as a contrasting group. The diode laser worked at the different rated power of 1.0 W, 1.5 W, 2.0 W, 3.0 W, 4.0 W, 5.0 W, 6.0 W, 7.0 W, 8.0 W in CW. Every emission in different power lasted for 20 seconds. Residual power was record and the temperature of the distal end was measured simultaneously.
Results
shows the residual power and temperature of the control group and film FOTC effect with CW and pulsed mode, versus the output power sequence of 1.0 W, 1.5 W, 2.0 W, 3.0 W, 4.0 W, 5.0 W, 6.0 W, 7.0 W, 8.0 W, which are presented as mean ± standard deviation (SD). All data were analyzed by using PC software SPSS 14.0 and Origin v8.0. The temperature, residual power and the output power were analyzed by linear or exponential regression model and Pearson correlations analysis. The adjusted R-square is the evaluation criteria of linear regression. All data were displayed in diagrams showing mean values and the standard deviations (x¯±s) for the measurements.
The linear fitting curves of temperature and power with a clear tip in control group were illustrated in . The curves in have good linearity (R2 = 0.995), suggesting that the residual power has a good linear response to output power in CW. Without a film FOTC, the residual power is equals the output power from the laser device theoretically. Whereas, the temperature had a poor linear response to output power (R2 = 0.638), so we use Pearson correlations analysis to evaluate the relation between temperature and the output power. Results indicated a strong correlation with Pearson χ2 = 0.824 > 0.8 (P < 0.01). There was an upward trend, in which temperature rising on the distal end of optical fiber clearly, displayed in . shows some abnormal data that when the output power increases on the output power of 2.0 W and 5.0 W, the temperature of a tip decreases instead. In this abnormality, the experimental error is considered which the rough cross section may absorb little laser energy and lead to temperature increasing. Theoretically, there is no photothermic effect in a clear tip of optical fiber, so that the temperature does not increase. A pen for fiber cutting used in oral clinical keep each cutting consistent hardly. The irregular section on the distal of the fiber absorbed slight laser energy that led to uncertainly rising of the temperature.
Figure 3. Linear response of the residual power (a) and temperature (b) to output power with a clear tip.
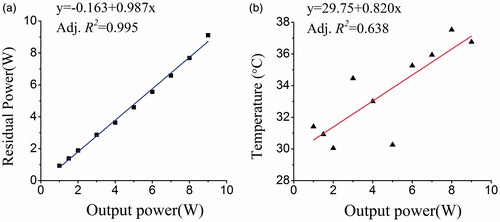
Table 1. Residual power and temperature of a clear tip and film FOTC with CW and pulsed mode.
and showed the change of residual power and temperature along with the output power in pulsed and CW modes. The output and residual power agree with each other, both with the adjusted R-square of 0.963 in two modes, indicated in and . P values were <0.01 and they can be considered linear correlation significant.
Figure 4. In pulsed mode, the linear fitting of the residual power (a); exponential fitting of the temperature (b).
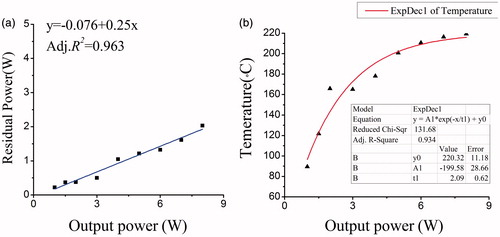
Figure 5. In CW, the linear fitting of the residual power (a); line chart and exponential fitting of the temperature (b).
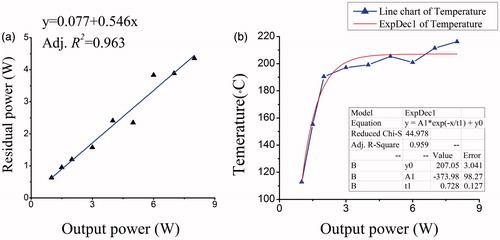
The conversion efficiency of thin-film FOTC equals to one minus the ratio coefficient of residual power to actual power. The actual output power in pulsed mode is half than rated power because of the square-wave pulse from the laser device with the frequency of 10 Hz and the duration of 0.05 s. showed the linear fitting coefficient was 0.25. The efficiency in pulsed mode is 50%. The conversion efficiency of thin-film FOTC in CW mode is 45.4%. Obviously, a film FOTC takes approximately half power to convert to heat however it is in CW or pulsed mode.
The temperature on thin-film FOTC increases considerably with the rise of the output power, rather than linear variation. It raised slowly as the power increased both in CW and pulsed modes. The exponential regression was used for modelling the temperature-power relation in continuous wave mode, with adjusted R2 = 0.959, while in pulsed mode with adjusted R2 = 0.934 (shown in and ). In the exponential regression model of CW mode, the temperature is reached up to maximum value 207 °C and eventually to be a stable state. The temperature was elevated up to 200 °C after the output power of 4 W and changes wavily in CW mode. In pulsed mode, the temperature was elevated up to maximum value 215 °C and eventually to be a stable state.
The adj. R-square in CW was higher than in pulsed mode, but the model is not very perfect. From the raw data, the maximum value is 216.24 ± 16.42 °C. Every time the same power and duration time were controlled, it is difficult to quantify the carbon film and microbubbles to produce the film FOTC. The standard deviation of the temperature is a considerable factor. In the tendency of the model, the temperature of the thin-film FOTC raised up slowly to the maximum value and kept stable at last. According to law of conservation of energy, the photothermic energy transferring to light and heat is scattered and lost in air, and eventually the temperature is balanced.
Discussion
Laser irradiation can generate biological damage in tissue through the laser-tissue interaction mechanisms [Citation27]. The potential damage depends on the optical absorption energy of the soft tissue, laser wavelength, beam size, selected power and pulsed duration. The thermal effect on tissue depends on the degree of temperature rise and the corresponding reaction of the interstitial and intracellular water [Citation28]. When the tissue containing water is heated to a temperature of 100 °C, vaporization of the interstitial and intracellular water occurs and the target tissue is ablated [Citation29] and transfers minimal heat to the adjacent tissue [Citation30]. When the degree of tissue temperature is elevated to 200 °C, dehydration is complete and the tissue carbonizes. The surface carbonized layer can continue to absorb the incident light of all wavelengths, becoming a heat sink. Hence, collateral thermal damage can spread rapidly and cause tissue necrosis [Citation31]. In soft-tissue laser surgery, the control of temperature plays a crucial role for surgeons. It is better to keep the photothermal effect of laser irradiation between vaporization and carbonization (from 100 °C to 200 °C). Excision of soft tissue begins with the phenomenon of vaporization, whereas the tissue carbonization prevents the target tissue from ablating, and reduces the efficiency of cutting or ablating soft tissue.
It could assume that collaborative work to accomplish incision of soft tissue both converter temperature and laser tissue photothermic interaction. In contact mode, the tissue is ablated owing to collaborative photothermal both heat on tip and residual emergent beam. The target tissue is firstly heated to a carbonized temperature rapidly by residual energy, and then the film FOTC heats the carbonization zone until disintegration. It can avoid the carbonization zone absorbs the energy of emergent beam. Laser surgery with a thin-film FOTC centralizes laser energy on the fiber tip while limiting the ability of the laser light to interact directly with target tissue.
In the article, the photothermal converter was proposed for solving the low surgical efficiency by means of concentrating the laser energy on the distal end of the optical fiber. Photothermic effect is determined by the temperature at the distal end of the fiber and residual power of laser radiation. The relationship between the temperature of fiber tips and power of residual radiation was studied on film FOTC for the first time. Belikov’s and Skrypnik’s work has completed the photothermal and structural modelling of volumetric fiber-optic thermal converter. The film FOTC was deserved more attention because of the clinical application feasibility.
Hot tip surgery in vitro by diode laser resulted in collateral damage widths about 2.7 times lower than those obtained after treatment with the clear tip [Citation32,Citation33]. The thermo-optical converter can produce vast amounts of heat on the distal end of the fiber promptly but more research is needed to explore the appropriate temperature in surgery. Temperature of fiber tips and power of residual radiation are vital parameters for physicians to carry on surgery. A mathematic model needs to be developed to describe the relation between the temperature and absorbed power on a film FOTC. Further research is needed to explore a safe and quantizable technique to manufacture a film FOTC.
Acknowledgements
This work was supported by National Natural Science Foundation of China (Grant No. 81602800). The authors thank other dentists for providing us a lot of help and advice, who are from Department of Dentistry, Peking Union Medical College Hospital.
Disclosure statement
No potential conflict of interest was disclosed.
References
- Desiate A, Cantore S, Tullo D, et al. 980 nm diode lasers in oral and facial practice: current state of the science and art. Int J Med Sci. 2009;6:358–364.
- Christensen GJ. Soft-tissue cutting with laser versus electrosurgery. J Am Dent Assoc. 2008;139:981–984.
- Lai M, Mu L, Cai K, et al. Apparatus and method for diode-pumped laser ablation of soft tissue. US patent; 2008.
- Pandurić DG, Bago I, Zore IF, et al. Application of diode laser in oral and maxillofacial surgery. In: Motamedi MH, editor. A textbook of advanced oral and maxillofacial surgery. Vienna: InTech; 2013.
- Romanos G, Nentwig G-H. Diode laser (980 nm) in oral and maxillofacial surgical procedures: clinical observations based on clinical applications. J Clin Laser Med Sur. 1999;17:193–197.
- Deppe H, Horch H-H. Laser applications in oral surgery and implant dentistry. Lasers Med Sci. 2007;22:217–221.
- Azma E, Safavi N. Diode laser application in soft tissue oral surgery. J Lasers Med Sci. 2013;4:206
- Janda P, Sroka R, Betz CS, et al. Comparison of laser induced effects on hyperplastic inferior nasal turbinates by means of scanning electron microscopy. Lasers Surg Med. 2002;30:31–39.
- Janda P, Sroka R, Tauber S, et al. Diode laser treatment of hyperplastic inferior nasal turbinates. Lasers Surg Med. 2000;27:129–139.
- Lippert B, Werner J. Nd: YAG laser light-induced reduction of the nasal turbinates. Laryngo-Rhino-Otol. 1996;75:523–528.
- Janda P, Sroka R, Mundweil B, et al. Comparison of thermal tissue effects induced by contact application of fiber guided laser systems. Lasers Surg Med. 2003;33:93–101.
- Vogel A, Venugopalan V. Mechanisms of pulsed laser ablation of biological tissues. Chem Rev. 2003;103:577–644.
- Bashkatov AN, Genina EA, Kochubey VI, et al. Optical properties of human skin, subcutaneous and mucous tissues in the wavelength range from 400 to 2000 nm. J Phys D: Appl Phys. 2005;38:2543.
- Bashkatov AN, Genina EA, Tuchin VV. Optical properties of skin, subcutaneous and muscle tissue: a review. J Innov Opt Health Sci. 2011;04:9–38.
- Skripnik A. Opto-thermal fiber converter of laser radiation. J Instrument Eng. 2013;9:37–42.
- Abela GS, Fenech A, Crea F, et al. Hot tip: another method of laser vascular recanalization. Lasers Surg Med. 1985;5:327–335.
- Rosenthal E, Montarello JK, Palmer T, et al. Coronary artery thermal damage during percutaneous hot tip laser-assisted angioplasty. Am J Cardiol. 1989;64:116–120.
- Verdaasdonk RM, Borst C, Boulanger LH, et al. Laser angioplasty with a metal laser probe (‘hot tip’): probe temperature in blood. Laser Med Sci. 1987;2:153–158.
- Lee G, Rubinson R, Chan MC, et al. Dissolution of pulmonary carcinoma via argon-laser bronchoscopy. First clinical use of fiberoptic metal cautery cap heated by laser radiation. Chest J. 1984;85:708–709.
- Manni J. Surgical diode lasers. J Clin Laser Med Surg. 1992;10:377–380.
- Verdaasdonck RM, Vandertop P, Ansink W, et al. editors. Laser-assisted neuroendoscopy using Nd: YAG and diode contact laser with black fiber tips. Proc. SPIE; 1997.
- Skripnik A. Fiber optoacoustic converter of laser radiation. J Instrument Eng. 2015;5:385–392.
- Belikov AV, Skrypnik AV, Kurnyshev VY, editors. Modeling of structure and properties of thermo-optical converters for laser surgery. Saratov Fall Meeting 2015; International Society for Optics and Photonics; 2016.
- Belikov AV, Skrypnik AV, Kurnyshev VY, et al. Experimental and theoretical study of the heating dynamics of carbon-containing optothermal fibre converters for laser surgery. Quantum Electron. 2016;46:534.
- Belikov AV, Skrypnik AV, Kurnyshev VY, editors. Thermal and optical modeling of blackened tips for diode laser surgery. SPIE Photonics Europe; International Society for Optics and Photonics; 2016.
- Mahtani P. Optical and structural characterization of amorphous carbon films [thesis]. Department of Electrical and Computer Engineering University of Toronto; 2010.
- Parker S. Lasers and soft tissue: ‘loose’ soft tissue surgery. Br Dent J. 2007;202:185–191.
- Coluzzi DJ. Fundamentals of lasers in dentistry: basic science, tissue interaction, and instrumentation. J Laser Dent. 2008;16:4–10.
- McKenzie A. Physics of thermal processes in laser-tissue interaction. Phys Med Biol. 1990;35:1175
- Rechmann P, Goldin DS, Hennig T, editors. Er: YAG lasers in dentistry: an overview. BiOS‘98 International Biomedical Optics Symposium; International Society for Optics and Photonics; 1998.
- Miserendino LJLG, Miserendino CA. Laser interaction with biologic tissues. Chapter 3. In: Miserendino LJ, Pick RM, editors. Laser in dentistry, Chicago (IL): Quintessence Publishing Co., Inc; 1995.
- Belikov AV, Skrypnik AV, Shatilova KV. Comparison of diode laser in soft tissue surgery using continuous wave and pulsed modes in vitro. Front Optoelectron. 2015;8:212–219.
- Kulikov K. Laser interaction with biological material. Biological & Medical Physics Biomedical Engineering; New York: Springer; 2014.