
Abstract
Background
Navigation brought about a tremendous improvement in functional endoscopic sinus surgery (FESS). When upgraded accordingly, FESS becomes navigated endoscopic sinus surgery (NESS). Indications for intraoperative use of navigation can be broadened to almost any FESS case. NESS in advanced sinus surgery is currently still not used routinely and requires systematic practice guidelines.
Purpose
The purpose of this paper is to report on commonly identified landmarks while performing advanced NESS according to evidence-based medicine (EBM) principles.
Material and methods
This review paper has been assembled following PRISMA guidelines. A PubMed and Scopus (EMBASE) search on anatomical landmarks in functional endoscopic and navigated sinus surgery resulted in 47 results. Of these, only 14 (29.8%) contained original data, constituting the synthesis of best-quality available evidence.
Results
Anatomical landmarks are considered to be the most important points of orientation for optimal use of navigation systems during FESS surgery. The most commonly identified significant landmarks are as follows: (1) Maxillary sinus ostium; (2) Orbital wall; (3) Frontal recess; (4) Skull base; (5) Ground lamella; (6) Fovea posterior; (7) Sphenoid sinus ostium. Conclusions: Establishing common landmarks are essential in performing NESS. This is true for advanced and novice surgeons alike and offers a possibility to use navigation systems systematically, taking advantage of all the benefits of endoscopic navigated surgery.
1. Introduction
The advent of functional endoscopic sinus surgery (FESS) may be attributed to professor Messerklinger’s book, published in 1978 and titled ‘Endoscopy of the Nose’, describing the basic principles of functional endoscopic sinus surgery [Citation1]. Since then, FESS has become a widespread procedure all over the world, and the most commonly performed surgical procedure in rhinology [Citation2]. In some countries, it is even the most frequent surgical procedure in otorhinolaryngology and head and neck surgery [Citation3]. During the past two decades, navigation systems have evolved immensely in both technological details and usefulness. Since vital structures are intimately associated with sinus surgery and hidden from direct visualization by mucusa and bone, navigation has garnered considerable interest among otolaryngologists [Citation3,Citation4]. Indications for intraoperative use of navigation can be broadened to almost any FESS case. NESS in advanced sinus surgery is currently still not used routinely and requires systematic practice guidelines. A position statement regarding intra-operative use of computer-aided surgery has been formulated by the American Rhinologic Society and American Academy of Otolaryngology and Head and Neck Surgery, suggesting its use in revision sinus surgery, distorted sinus anatomy of development, extensive sino-nasal polyposis, and benign or malignant neoplasms, pathology involving the frontal, posterior ethmoid, and sphenoid sinuses, disease abutting the skull base, orbit, optic nerve or carotid artery, CSF rhinorrhea or conditions where there is a skull base defect [Citation4]. Sinus surgeons require a very strong understanding of anatomy and spatial orientation at all times during surgery, which is difficult when dealing with anatomy that develops in a stochastic fashion. Using navigated systems allows for accurate localization in anatomically complex areas by gaining more data on orientation through CT coordinate frames than direct visualization alone while enabling surgeons to track their instruments inside the patient. However, all navigated systems suffer from tracking errors >1 mm, which may be a source of significant intraoperative orientation bias if used blindly, without confident orientation using endoscopically visible reliable anatomical landmarks [Citation5]. Using a surgical algorithm for orientation would be helpful for both young surgeons and their teachers to shorten their learning curve and provide a common practice to aid during surgery [Citation6]. Unfortunately, very few such algorithms have been proposed, and consensus on commonly identified landmarks that are to be identified during FESS or NESS is yet to be achieved [Citation6].
The purpose of this paper is to identify the most commonly reported landmarks to aid in performing advanced NESS according to evidence-based medicine (EBM) principles.
2. Material and methods
This review paper has been assembled following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A cross-referenced PubMed and Scopus (EMBASE) search was performed and relevant data were extracted accordingly. Initially, searching was performed using the following keywords: functional endoscopic sinus surgery, navigated endoscopic sinus surgery, and landmarks, resulting in 47 results. The keywords were combined using the Boolean operator AND. Of these, only 14 (29.8%) contained original data concerning endoscopic surgery landmarks, constituting the synthesis of best-quality available evidence. A landmark was considered to be a sinonasal anatomical structure providing the surgeon with a common reference point in 3-dimensional space while viewing a 2-dimensional screen.
We included papers that correlated using landmarks, imaging studies, and surgical anatomy papers with other relevant criteria, like outcomes, histopathology, endoscopy. Exclusion criteria were: full text not available (three records), papers concerning other topics (30). Thus, 14 records were included in this review ().
Table 1. Papers discussing surgical accuracy and landmarks in FESS and NESS.
3. Results
This review is concerned with a clinical question of whether common landmarks may be consistently identified while performing navigated endoscopic sinus surgery. It is of great clinical importance for otolaryngologists and radiologists alike, especially considering the impact on associated outcomes and surgeons’ training curves [Citation3–6].
3.1. Landmarks currently in practice
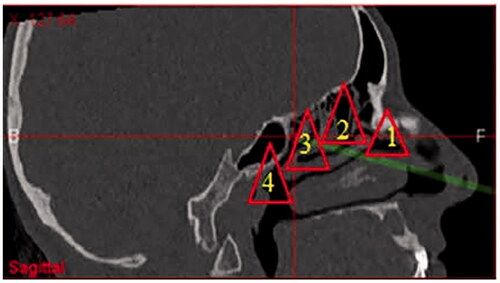
One previous algorithm for NESS suggested identifying 28 landmarks that should be recognized while performing basic FESS [Citation6]. This principle required highlighting landmark groups using a navigation system. The major landmark groups were the nasal vestibule, ostiomeatal complex, anterior ethmoid, posterior ethmoid, and sphenoid. Each landmark group was described as a triangular pyramid, consisting of at least four reference points. The most common anatomical areas identified in published literature concerning increasing surgical precision and safety while performing initial and revision endoscopic sinus surgery are the following: 1—ostiomeatal complex (OMC), 2—anterior ethmoid, 3—posterior ethmoid, and 4—sphenoid (). Navigated orientation was designed to precede any surgical intervention, and in this way improve the learning curve of surgeons while using the navigation system routinely and systematically [Citation6].
Figure 1. Four navigational units: (1) OMC unit; (2) Anterior ethmoid unit; (3) Posterior ethmoid unit; and (4) Sphenoidal unit.
3.2. Newly identified landmarks for navigated surgery
After reviewing published literature identifying landmarks that must be marked during NESS surgery, seven common landmarks may be extrapolated (). These landmarks are crucial in using the navigation system while performing basic FESS [Citation4]. Landmarks that have been shown as most commonly identified are located in all four previously described navigational units and reiterated by several papers [Citation4–11]. The landmarks are as follows: (1) maxillary sinus ostium; (2) orbital wall; (3) frontal recess; (4) skull base; (5) ground lamella; (6) fovea posterior; (7) sphenoid sinus ostium (). Since these landmarks are consistently reported in all 14 studies analyzed, and no comparable data exist on their registration accuracy, they were extrapolated based on their anatomical and surgical implications.
Figure 2. Seven reliable landmarks in NESS: (1) Maxillary sinus ostium; (2) Any point on the orbital wall; (3) Frontal recess; (4) Any point on the skull base; (5) Ground lamella; (6) Fovea posterior; and (7) Sphenoid sinus ostium.
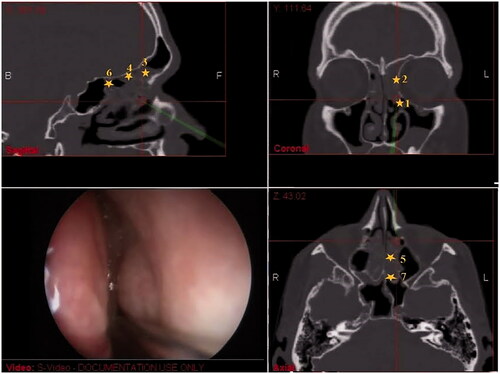
Figure 3. A 3D CT reconstruction highlighting the seven landmarks.
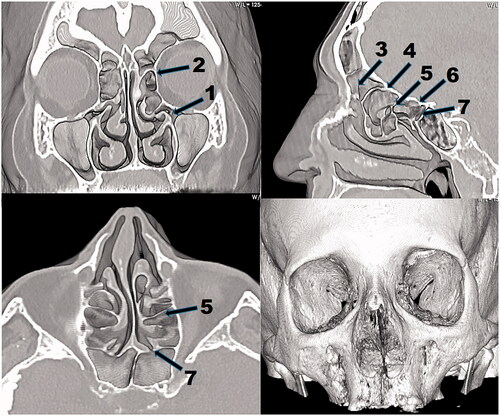
Table 2. A list of seven reliable landmarks in NESS.
4. Discussion
The current recommendations of the American Academy of ORL-HNS, based on expert consensus of opinion and evidence-based literature list examples in which navigation may be appropriate with a clear recommendation that intraoperative use of navigation may be beneficial in any FESS case apart from anterior ethmoidectomy [Citation4,Citation12]. Randomized controlled trials comparing FESS and NESS are hindered by the projected sample size of such a study and lack of clinical equipoise [Citation13–15]. Nevertheless, there are studies that show that navigation influenced accuracy, efficiency, complication rate, the final outcome for the patients, and task workload [Citation3,Citation11,Citation13]. A recent systematic review and meta-analysis indicated that the use of navigation resulted in decreased major and total complications compared to ESS performed without this tool. A meta-analysis of 14 source studies demonstrated a statistically significant reduction in the relative risk (RR) of major (RR = 0.48, 95% confidence interval [CI] 0.28, 0.82) and total complications (RR = 0.66, 95% CI0.47, 0.94) when NESS was used compared to FESS without the use of navigation [Citation16]. Using navigation clearly helps surgeons improve their training and education but it does not replace proper training and ability to maintain accurate orientation in complex cases [Citation5,Citation14,Citation17,Citation18].
With a significant increase in patients requiring revision surgery, NESS may especially be highlighted as beneficial for both the surgeon and the patient [Citation10,Citation19]. In many revision surgeries, and especially in malignant tumor endoscopic resection cases, anatomic landmarks are often obscured or absent; thus, a set of consistent landmarks (unchanged despite prior surgery) should be used to navigate the endoscopic sinus surgery [Citation10].
There is no consensus on reliable landmarks, and only a handful of studies listed those that may be identified under both direct visualization and on available CT scans during navigated surgery, ensuring precise orientation at all times during surgery [Citation20–26]. After reviewing available literature, it was clear that several anatomical reference points in 3-dimensional space while viewing a 2-dimensional screen were identified as the most frequent points of reference. They are the most reliable orientation points that can be identified by combined identification through endoscopy and CT images during navigated surgery, especially if some of them are obscured or missing during direct visualization only.
Any anatomical landmark may be identified in ordinary anatomical circumstances by the surgeon using image guidance alone with an absolute position error of 0.21 mm and a mean absolute orientation error of 2.8° compared to ground truth, as evidenced by studies verifying positional accuracy. In reality, registration accuracy studies have investigated existing navigation systems during real surgeries, but only able to claim accuracy of 1.28 ± 1:09 mm, hardly enough to claim adequate surgical accuracy based on CT-guided landmark identification alone [Citation5]. No data in the literature exist on registration accuracy in actual clinical use with sinus surgery landmarks, but Krings et al. report that image-guided FESS procedures can also have an increased rate of complications due to overconfidence and reliance on navigation when maneuvering in an anatomically complex area [Citation27].
However, when coupled with the surgeon's anatomical knowledge and spatial orientation ability, the capability of accurate landmark identification during actual surgery becomes much more dependable [Citation5,Citation28]. For instance, the fenestration rate for the sphenoid sinus in revision FESS without image-guided surgery (IGS) was significantly lower than that in revision FESS with IGS (p = .004). It showed that IGS was a beneficial procedure for opening the sphenoid sinus in the revision cases [Citation10].
Three of the seven proposed landmarks are natural ostia of maxillary, frontal, and sphenoidal sinuses since FESS is originally oriented toward addressing pathology caused by obstructed ostia [Citation13,Citation14]. Locating the ostia ahead of other landmarks instantly improves the surgeon’s orientation. In patients with distorted anatomy and severe pathology, especially revision cases, finding the natural ostium may not be possible. The safest location to enter the maxillary sinus is through the posterior fontanel just above the posterior third of the inferior turbinate. The nasolacrimal convexity identification prevents injury of the nasolacrimal duct and the posterior maxillary sinus wall may be used as a guide to assess the depth of the sphenoid sinus [Citation20,Citation22]. One of the most demanding parts of FESS surgery is locating the frontal recess and approaching the frontal sinus. Surgical training emphasizes a cellular organization of the sinuses, with lamellas separating the specific sinus cells. However, the ethmoid anatomy is central to the difficulty of consistent orientation within the ethmoid cells. Recent advances in imaging have eroded the belief that the uncinate process and ethmoid bulla are separate entities, but rather show that the two appear to fuze superiorly forming a consistent landmark medial to which the frontal sinus drains in 77% of cases. The uncinate process and ethmoidal bulla fuze forming a genu-like structure in the anterior ethmoid. This consistent anatomic feature can be used as a landmark in the anterior ethmoid and frontal recess surgery [Citation24]. Identification of the point of entry into the floor of the frontal sinus when drilling is plagued by the variability of distance from the posterior table of the frontal sinus. Image-guided surgery has been shown to increase accuracy in locating the floor of the frontal sinus, especially when sinonasal and olfactory fossa pathology may distort anatomy [Citation24,Citation25]. Landmark 5—the ground lamella is very important as a frontier between anterior and posterior ethmoidal cells. Identification of this landmark enables the surgeon to proceed further toward the posterior ethmoids. Once the lamina papyracea is identified, the dissection can proceed through the supero-posterior ethmoid cells up to the fovea ethmoidalis. Landmark 6—the fovea posterior is important to be highlighted as it is the last ethmoidal space before entering the endocranium [Citation21,Citation22]. The landmark 2—orbital wall, and landmark 4—a point on the skull base are designated to identify the most critical structures in our operating field [Citation23,Citation26]. These landmarks may be identified by observing any specific point of these anatomical structures. During surgery, they may be highlighted several times in different parts of their anatomical structures. While other landmarks like the middle turbinate could be distorted by pathology or removed by previous surgery, the orbital wall is seldom affected. In endoscopic surgery, the only relevant outer landmark is the eyeball, and it is used only indirectly, through identifying orbital content after external pressure on the orbit (bulb-press test) [Citation29]. Visualization of the orbital wall and floor gives a reliable account of the lamina papyracea, while also preventing injury to the carotid artery, the optic nerve, orbital muscles, anterior ethmoid artery, and skull base. The distances from the orbital floor and the carotid artery, optic nerve, and ethmoid arteries are constant and the orbital floor is a landmark of safe entry into the sphenoid when all other anatomic features have been distorted [Citation22,Citation29]. By failing to identify these landmarks, the surgeon risks severe complications [Citation28,Citation30]. The sphenoid sinus ostium is a common landmark in limiting the dissection in relation to the superior skull base and lateral lamina papyracea boundaries. After the sphenoid sinus is reached, planum sphenoidale and the sphenoid lateral wall will represent the superior and lateral limits of dissection.
The commonly identified landmarks listed in the paper are designated in natural logical order, starting from the anterior part of the nasal cavity up to the skull base and the sphenoid sinus. While performing FESS surgery, they should always be approached one by one, standardizing the procedure and safeguarding the vital surrounding structures.
The limitations of these landmarks are evident by the absence of existing surgical guidelines since the level of evidence of reported studies has been low [Citation30]. The absence of review papers is due to the fact that this is a very novel field of image-guided surgery, and papers on landmarks during ESS or NESS to date have been scarce. There are numerous issues in selecting any number of landmarks intended to improve image-guided sinus surgery. Low frequency of major complications and the absence of comprehensive analyses of landmarks’ identification make the definitive selection of landmarks difficult. Studies reporting on anatomical landmarks have significant selection bias and study design flaws including outcome analysis, completeness of surgery, and cost-utility. The labeling of any anatomical landmark as reliable implies high registration accuracy and should consider distribution, shape characteristics, accessibility, and safety of landmark, which were validated by analyzing a low number of available studies. The authors endeavored to identify the most likely candidates that correspond to a practical surgical protocol and would complement surgery, rather than complicate it.
5. Conclusion
Using navigation systems is not experimental or investigational. Navigation systems serve to aid the endoscopic sinus surgeon. To be capable to fully appreciate its usefulness in complicated cases, identifying common landmarks could improve surgical orientation in a highly complex anatomical setting. They are orientation points that can be identified by combined identification through endoscopy and CT images during navigated surgery, especially if some of them are obscured or missing during direct visualization only.
Ethical approval
This study was approved by the University Hospital Center Sestre Milosrdnice, Zagreb, bioethical board adhering to the Ethical Principles for Medical Research Involving Human Subjects, adopted by the 18th World Medical Assembly, Helsinki, Finland, June 1964, and as amended most recently by the 64th World Medical Assembly, Fortaleza, Brazil, October 2013.
Disclosure statement
The authors have no conflict of interest to disclose. The authors received no funding from private or public institutions for the preparation of this manuscript. All authors should have read the final version of the paper and agreed with it.
References
- Stammberger H, Posawetz W. Functional endoscopic sinus surgery. Concept, indications and results of the Messerklinger technique. Eur Arch Otorhinolaryngol. 1990;247(2):63–76.
- Palmer JN, Kennedy DW. Historical perspective on image-guided sinus surgery. Otolaryngol Clin North Am. 2005;38(3):419–428.
- Justice JM, Orlandi RR. An update on attitudes and use of image guided surgery. Int Forum Allergy Rhinol. 2012;2(2):155–159.
- American Rhinologic Society. Criteria for image guided surgery [cited 2021 Feb 28]. Available from: https://www.american-rhinologic.org/index.php?option=com_content&view=article&id=35:criteria-for-image-guided-surgery&catid=26:position-statements&Itemid=197
- Leonard S, Sinha A, Reiter A, et al. Evaluation and stability analysis of video-based navigation system for functional endoscopic sinus surgery on in vivo clinical data. IEEE Trans Med Imaging. 2018;37(10):2185–2195.
- Baudoin T, Grgić MV, Zadravec D, et al. Algorithm for navigated ESS. Rhinology. 2013;51(4):335–342.
- Bewick J, Egro FM, Masterson L, et al. Anatomic findings in revision endoscopic sinus surgery: case series and review of contributory factors. Allergy Rhinol. 2016;7(3):151–157.
- Ali MJ, Nayak JV, Vaezeafshar R, et al. Anatomic relationship of nasolacrimal duct and major lateral wall landmarks: cadaveric study with surgical implications. Int Forum Allergy Rhinol. 2014;4(8):684–688.
- Joshi AA, Shah KD, Bradoo RA. Radiological correlation between the anterior ethmoidal artery and the supraorbital ethmoid cell. Indian J Otolaryngol Head Neck Surg. 2010;62(3):299–303.
- Levine CG, Casiano RR. Revision functional endoscopic sinus surgery. Otolaryngol Clin North Am. 2017;50(1):143–164.
- Jiang RS, Liang KL. Image-guided sphenoidotomy in revision functional endoscopic sinus surgery. Allergy Rhinol. 2014;3:116–119.
- American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS). Position statement: intra-operative use of computer aided surgery [updated 2009 Nov 17; cited 2016 Aug 14]. Available from: http://www.entnet.org/content/intra-operative-use-computer-aided-surgery
- Oakley GM, Barham HP, Harvey RJ. Utility of image-guidance in frontal sinus surgery. Otolaryngol Clin North Am. 2016;49(4):975–988.
- Dixon BJ, Chan H, Daly MJ, Qiu J, et al. Three-dimensional virtual navigation versus conventional image guidance: a randomized controlled trial. Laryngoscope. 2016;126(7):1510–1515.
- Koulechov K, Strauss G, Dietz A, et al. FESS control: realization and evaluation of navigated control for functional endoscopic sinus surgery. Comput Aided Surg. 2006;11(3):147–159.
- Beswick DM, Ramakrishnan VR. The utility of image guidance in endoscopic sinus surgery: a narrative review. JAMA Otolaryngol Head Neck Surg. 2020;146(3):286–290.
- Dalgorf DM, Sacks R, Wormald P-J, et al. Image-guided surgery influences perioperative morbidity from endoscopic sinus surgery: a systematic review and meta-analysis. Otolaryngol Head Neck Surg. 2013;149(1):17–29.
- Citardi MJ, Batra PS. Intraoperative surgical navigation for endoscopic sinus surgery: rationale and indications. Curr Opin Otolaryngol Head Neck Surg. 2007;15(1):23–27.
- Dixon BJ, Chan H, Daly MJ, Vescan AD, et al. The effect of augmented real-time image guidance on task workload during endoscopic sinus surgery. Int Forum Allergy Rhinol. 2012;2(5):405–410.
- Hilger AW, Ingels K, Joosten F. Sagittal computerized tomography reconstruction of the lateral nasal wall for functional endoscopic sinus surgery. Clin Otolaryngol Allied Sci. 1999;24(6):527–530.
- Ahmadian A, Fathi Kazerooni A, Mohagheghi S, et al. A region-based anatomical landmark configuration for sinus surgery using image guided navigation system: a phantom-study. J Craniomaxillofac Surg. 2014;42(6):816–824.
- Dedhia RD, Hsieh TY, Rubalcava Y, et al. Posterior maxillary sinus wall: a landmark for identifying the sphenoid sinus ostium. Ann Otol Rhinol Laryngol. 2019;128(3):215–219.
- Jolly K, Kontogiannis T, Pankhania M, et al. Use of the medial canthal point (MCP) as a reliable anatomical landmark to the frontal sinus. Laryngoscope Investig Otolaryngol. 2020;5(5):791–795.
- Bolger WE, Stammberger H, Ishii M, et al. The anterior ethmoidal genu: a newly appreciated anatomic landmark for endoscopic sinus surgery. Clin Anat. 2019;32(4):534–540.
- Walgama ES, Thamboo A, Tangbumrungtham N, et al. The horizon sign and frontal bar: two topographic landmarks to confirm endoscopic frontal sinusotomy. Otolaryngol Head Neck Surg. 2019;160(4):740–743.
- Abdullah B, Chuen CS, Husain S, et al. Is orbital floor a reliable and useful surgical landmark in endoscopic endonasal surgery? A systematic review. BMC Ear Nose Throat Disord. 2018;18(1):11.
- Krings JG, Kallogjeri D, Wineland A, et al. Complications of primary and revision functional endoscopic sinus surgery for chronic rhinosinusitis. Laryngoscope. 2014;124(4):838–845.
- Labruzzo SV, Aygun N, Zinreich SJ. Imaging of the paranasal sinuses: mitigation, identification, and workup of functional endoscopic surgery complications. Otolaryngol Clin North Am. 2015;48(5):805–815.
- Maharshak I, Hoang JK, Bhatti MT. Complications of vision loss and ophthalmoplegia during endoscopic sinus surgery. Clin Ophthalmol. 2013;7:573–580.
- Strauss G, Koulechov K, Röttger S, et al. Evaluation of a navigation system for ENT with surgical efficiency criteria. Laryngoscope. 2006;116(4):564–572.