
Abstract
Background
Though some studies have reported navigated high tibial osteotomy (HTO) is a useful procedure to correct knee deformity. There is still great controversy whether navigated HTO can achieve better accuracy of limb alignment and greater clinical outcomes. Current meta-analysis was conducted to investigate whether better radiographic outcomes and clinical outcomes could be acquired in navigated HTO compared with the conventional procedure.
Method
We conducted a literature search in the electronic databases, including Medline, Embase, the Cochrane Library, and Web of Science. We identified studies published before August 2020. We also checked the references of the related articles for any relevant studies. We strictly followed the Preferred Reporting Items for Systematics reviews and Meta-Analysis (PRISMA) guidelines in this review. This research was performed using Review Manager 5.4 software.
Results
Fourteen articles were included, involving 1399 knees. Our meta-analysis indicated that patients undergoing navigated HTO had significantly better outcomes in outliers of aimed limb alignment (RD=−0.24, 95% CI: =−0.34 to −0.13, p < 0.01), outliers of aimed tibial posterior slope (TPS) (RD=−0.41, 95% CI: −0.51 to −0.30, p < 0.01), Range of Motion (ROM) (MD = 6.37, 95%CI: 0.83–11.91, p = 0.02), and American knee society knee score (AKS knee score) (MD = 3.88, 95%CI: 1.37–6.39, p = 0.002). No significant differences were found in Lysholm score (MD = 1.30, 95%CI: −0.31 to 2.90, p = 0.11), American knee society function score (AKS function score) (RD = 1.42, 95%CI: −0.15 to 2.99, p = 0.08), complications (RD=−0.01, 95% CI: = −0.05 to 0.04, p = 0.77), delayed union (RD=−0.01, 95% CI: = −0.02 to 0.03, p = 0.59), and reoperation (RD = 0, 95% CI: −0.09 to 0.10, p = 0.98) between the two groups. The operation time in the navigated group was 15.46 min longer than in the conventional group.
Conclusion
Navigated HTO provided more accurate and reproducible radiographic outcomes in the correction of the malalignment than conventional techniques, and there is no difference in the risk of complications compared with conventional HTO. However, it is unclear whether navigation HTO can achieve better clinical results. More randomized controlled trials (RCTs) with high quality, large sample size, and sufficient follow-up period are required.
Background
Since the 1960s, high tibial osteotomy (HTO) was used for the treatment of unicompartmental osteoarthritis of the knee [Citation1–3]. Despite the great progression of total knee arthroplasty (TKA) or the revival of unicompartmental knee arthroplasty (UKA), HTO is a more moderate method for young and active patients [Citation4,Citation5]. The accuracy of alignment is essential for the successful long-term clinical outcomes. Under- or over-correction after HTO may lead to complications and quick to failure [Citation6]. Failure to achieve aimed alignment has been reported as a remarkable reason for unsatisfactory clinical results, which are described as outliers [Citation7].
Computer navigated system has been introduced in the HTO to reduce the risk of outliers [Citation8]. Some studies have reported the navigated group improves the accuracy of alignment compared with the conventional group [Citation2,Citation7,Citation9]. However, whether the navigated system could achieve better correction of alignment and better clinical outcomes than conventional technology remains controversial. By summarizing controlled studies comparing navigated HTO with conventional technology, some systematic reviews and meta-analyses have concluded better radiographic outcomes could be acquired in the navigated system [Citation10–12]. But given the increased number of studies in the past few years [Citation2,Citation13], there is a need to evaluate these evidences to determine a better effective strategy in terms of accuracy of radiographic outcomes, functional results, complications, and surgery time. Therefore, our meta-analysis was performed to clarify whether the navigated system could show more accuracy of alignment and more benefits in clinical outcomes.
Methods
Statistical heterogeneity was assessed using the value of p and I2. If p was >0.1 and I2 was <50%, the fixed-effects model was used; otherwise, the random-effects model was used to do the analysis. Random-effects models were utilized to reduce heterogeneity. If the heterogeneity of a parameter was over 85%, the meta-analysis was not performed. The results of continuous data were applied to the mean difference with 95% confidence interval (CI). For dichotomous data, the risk difference (RD) was calculated using the Mantel–Haenszal method, mean difference (MD) and standardized mean difference (SMD) were considered statistically significant at the p < 0.05 level. Data analysis was carried out by using Review Manager 5.4. Sensitivity analysis was performed to assess the results through exclusion of eligible studies once time.
Literature search
A literature search was conducted to search studies which made a comparison between conventional and navigated technique in the HTO. The searched terms were followings: ‘osteotomy’, ‘Tibia*’, ‘High’, ‘Navigation’, ‘Computer-assisted’. Embase, Medline, Web of Science, Cochrane databases were searched to retrieve related studies updated on August 2020.
Inclusion and exclusion criteria
To be included in our analysis, the study had to follow inclusion criteria belowings:
(1) studies compared the clinical or radiographic outcomes in patients who underwent navigated HTO and conventional HTO; (2) clinical or radiographic outcomes were not limited to pool; (3) published studies in English were eligible. Studies were excluded: (1) conference, review, abstract, case report, sawbones or cadaver knees, non-comparable studies (2) studies reported with insufficient data (3) duplicate publication, (4) studies not published in English.
Data extraction
The following data were independently extracted from each of the included studies by two investigators (YQ and WQ). They are surgeons with rich surgical experience and statistical knowledge. The outcomes of our research including outliers of aimed limb alignment; outliers of aimed tibial posterior slope (TPS); Lysholm score; America knee society knee score (AKS score); Range Of Motion (ROM); complications (hardware removal, delayed union, wound hematoma, infection, osteoarthritis progression requiring conversion to TKA and et al.); delayed union; reoperation (hardware removal, osteoarthritis progression requiring conversion to TKA, nonunion requiring a revision, and et al.) and surgical time (minutes); Lysholm score is widely used to evaluate the knee joint, including functional perception and function level [Citation14]. AKSS has two parts: AKS knee score and AKS function score [Citation15,Citation16]. The AKS knee score includes pain, mobility, and stability. AKS function score assesses the ability to walk and go up and down stairs. When disagreement existed, it was resolved by consulting another investigator (XK).
Quality assessment
The quality of the non-RCTs studies was assessed according to the Downs and Black [Citation17] and the Newcastle-Ottawa Scale (NOS) [Citation18] quality assessment method. A total NOS score was 9* and if the NOS score was over 6*, it would be considered as higher quality research. A higher score was recognized as better quality research. The 12-item scale was used to assess the quality of the RCTs [Citation19]. Each item was scored ‘Yes’, ‘Unclear’, or ‘No’. If a trial with a score of more than 7 ‘Yes’ was considered high quality, more than 4 but no more than 7 was considered moderate quality, and no more than 4 was considered low quality. Any different opinions were resolved by a third reviewer (WJ).
Results
Study selection
By scanning the titles and abstracts, 24 articles that met the inclusion criteria were reviewed for full-text screening. After full texts were assessed for eligibility, some articles were rejected because they only reported the outcomes of navigated group [Citation6,Citation20], performed on sawbones or cadaver knees [Citation21–24], data had already been reported elsewhere in partly [Citation25,Citation26], and reported with insufficient data [Citation27,Citation28]. Finally, a total number of 14 eligible articles were described [Citation1,Citation2,Citation4,Citation7–9,Citation13,Citation29–35]. The characteristics of including studies in the meta-analysis were shown in and ; there were 781 knees in the navigated group, and 618 knees in the conventional group. The selection process was illustrated in .
Figure 1. Flow chart of the study selection procedure.
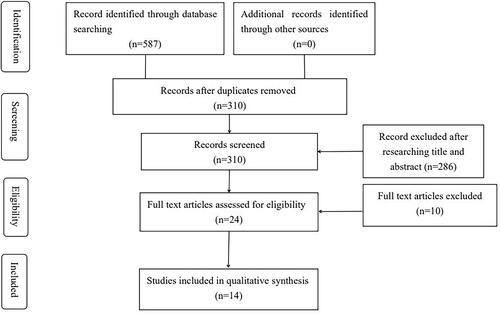
Table 1. The characteristics of included studies(a) in the meta-analysis.
Table 2. The characteristics of included studies(b) in the meta-analysis.
Quality of the included studies
Our research consisted of 11 non-RCTs [Citation1,Citation2,Citation4,Citation7,Citation9,Citation13,Citation29,Citation30,Citation32–34] and 3 RCTs [Citation8,Citation31,Citation35]. All included studies were over 15 in terms of Downs and Blacks score and had scored ≥ 6* in NOS. The quality of non-RCTs studies was shown in . The value of weighted kappa for the agreement on these studies between reviewers was excellent (Κ = 0.73). All studies were high quality according to the outcomes of 12-item scale [Citation8,Citation31,Citation35]. The randomization methods were explicitly introduced in 3 studies. Randomization allocation was concealed adequately in 2 studies [Citation8,Citation35]. None of RCTs provided the information of double blinding. None of them reported a binding of outcome assessment. The quality of RCTs was shown in .
Table 3. Non-RCTs studies quality.
Table 4. RCTs studies quality.
Outliers of aimed limb alignment
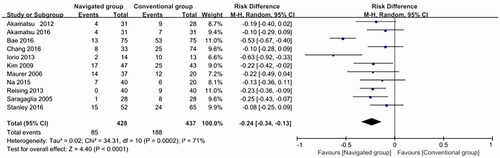
Eleven studies reported the outliers of aimed limb alignment [Citation1,Citation7–9,Citation13,Citation29–34]. There were 85 of 428 patients (19.86%) in the navigated group and 188 of 437 patients (43.02%) in the conventional group. Significant heterogeneity was detected (p = 0.0002; I2 = 71%), so the random-effects model was performed. The pooled result revealed that the navigated group significantly reduced the rate of outliers of limb alignment compared with the conventional group (RD=−0.24, 95%CI: = −0.34 to −0.13, p < 0.01. ).
Figure 2. Forest plot diagram showed the risk difference in outliers of aimed limb alignment between navigated group and conventional group.
Outliers of aimed TPS
Two articles reported the outcomes of outliers of aimed TPS [Citation8,Citation13]. There were 4 of 108 patients (3.77%) in the navigated group and 47 of 106 patients (44.34%) in the conventional group. No significant heterogeneity was detected between the studies (p = 0.83; I2=0); therefore, the fixed-effects model was used to do analysis. The pooled results showed that the navigated group had a significantly better outcome in the rate of outliers of tibial alignment (RD=−0.41, 95%CI: −0.51 to −0.30, p < 0.01; ).
Figure 3. Forest plot diagram showed the risk difference in outliers of aimed TPS between navigated group and conventional group.

Lysholm score
Four articles reported the Lysholm score [Citation4,Citation8,Citation29,Citation32]. No significant heterogeneity was detected between the studies (p = 0.24; I2=29%); therefore, the fixed-effects model was used to do analysis. The pooled results demonstrated that no significant difference was found in the rate of pain between the two groups (MD = 1.30, 95%CI: −0.31 to 2.90, p = 0.11; ).
Figure 4. Forest plot diagram showed the mean difference in Lysholm score between navigated group and conventional group.

AKSS
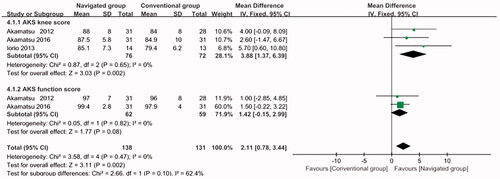
Owing to the AKSS including AKS knee score and AKS function score, the data of AKSS were grouped by AKS knee score and AKS function score pooling to do analysis. Three studies reported AKS knee score [Citation8,Citation29,Citation31] and two studies reported AKS function score [Citation8,Citation29]. There was no significant heterogeneity in AKS knee score (p = 0.65; I2 = 0%), AKS function score (p = 0.82; I2=0%) and total (p = 0.47; I2 = 0%); therefore, the fixed-effects model was used. The final outcomes manifested that significant difference was found between the two groups in AKS knee score (MD = 3.88, 95%CI: 1.37 to 6.39, p = 0.002; ) and total (MD = 2.11, 95%CI: 0.78 to 3.44, p = 0.002; ) and no significant difference was found between the two groups in AKS function score (RD = 1.42, 95%CI: −0.15 to 2.99, p = 0.08; ).
Figure 5. Forest plot diagram showed the AKSS between navigated group and conventional group.
ROM
Two studies compared the ROM [Citation8,Citation29]. The data of them were pooled to do analysis. There was no significant heterogeneity between the studies (p = 0.67; I2=0%); therefore, the fixed-effects model was used. It showed the navigated group had a significantly better outcome in ROM (MD = 6.37, 95%CI: 0.83 to 11.91, p = 0.02; )
Figure 6. Forest plot diagram showed the mean difference in ROM between navigated group and conventional group.

Total complications
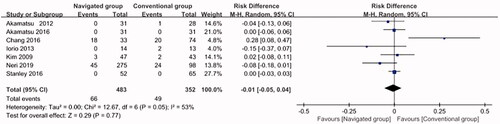
Seven studies reported the event of complications [Citation1,Citation2,Citation8,Citation29–32]. There were 66 of 483 patients (13.66%) in the navigated group and 49 of 352 patients (13.92%) in the conventional group. Substantial heterogeneity was detected (p = 0.29; I2=53%), so the random-effects model was performed. The results demonstrated that no significant difference was found in the rate of complications (RD=−0.01, 95%CI: = −0.05 to 0.04, p = 0.77; ).
Figure 7. Forest plot diagram showed the risk difference of total complications between navigated group and conventional group.
Delayed union
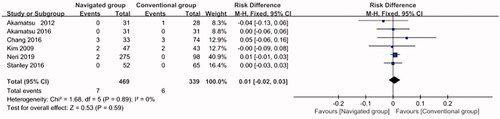
Six studies reported the event of delayed union [Citation1,Citation2,Citation8,Citation29,Citation30,Citation32]. There were 7 of 469 patients (1.49%) in the navigated group and 6 of 339 patients (1.77%) in the conventional group. No significant heterogeneity was detected (p = 0.89; I2=0%), so the fixed-effects model was performed. The results demonstrated that no significant difference was found in the rate of delayed union (RD = 0.01, 95% CI: = −0.02 to 0.03, p = 0.59; ).
Figure 8. Forest plot diagram showed the risk difference of delayed union between navigated group and conventional group.
Reoperation
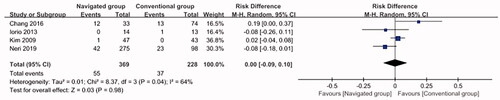
Four articles reported the reoperation. There were 55 of 369 patients (14.91%) in the navigated group and 37 of 228 patients (16.23%) in the conventional group. Substantial heterogeneity was detected between the studies (p = 0.04; I2=64%); therefore, the random-effects model was used to do analysis. The pooled results demonstrated that no significant difference was found in the rate of reoperation between the two groups (RD = 0, 95% CI: −0.09 to 0.10, p = 0.98; ).
Figure 9. Forest plot diagram showed the risk difference of reoperation between navigated group and conventional group.
Surgical time (minutes)
Operation time was reported in seven studies [Citation2,Citation7,Citation8,Citation29,Citation30,Citation32,Citation35]. All of included studies were reported longer surgical time was observed in navigated group, and the navigated group was 15.46 min longer than in the conventional group. The heterogeneity was over 85% (I2=95%); therefore, the overall effects of this parameter were not performed.
Sensitivity analysis
One study was individually deleted each time to observe its influence on the pooled MD or RD. The results showed that no study could substantially affect the pooled MD or RD in the present meta-analysis.
Discussion
Our meta-analysis had demonstrated that the use of navigated HTO was significantly better in the aimed alignment, aimed TPS, AKS knee score, and ROM. But no significant difference was found in Lysholm score, AKS function score, total complications, delayed union, reoperation, and revision. In addition, the navigated group was 15.46 min longer than in the conventional group. The success of HTO is dependent on the accuracy of mechanical leg axis [Citation4]. But there is a controversy about the ideal aimed limb alignment. Some surgeons suggest a neutral correction or slight over-corrections of the joint while other surgeons suggest under-corrections [Citation7,Citation15,Citation28,Citation36,Citation37]. Due to this situation, we compared the outliers of aimed limb alignment and aimed TPS. In our study, we found that the outliers of aimed limb alignment and the outliers of aimed TPS in the navigation group were significantly lower than those in the conventional group. In the included literature, 13 of the 14 studies reported the navigated group had significantly better radiological results than the conventional group. Only Stanley et al. concluded the navigated system provided limited improvement of radiographic correction [Citation1]. Nevertheless, the study was limited by the use of different implants to stabilize the osteotomy and the osteotomy gap is filled with a set of heterogeneous bone substitutes. In addition, Lützner et al. found the navigated HTO had better correction of mechanical leg axis than the conventional HTO in a cadaver study [Citation22]. Saragaglia et al. also reported that the navigated osteotomy provided reliable and accurate deformity correction for osteoarthritis patients with knee valgus, with an average follow-up of 50.9 months [Citation28].
Regarding clinical outcomes, our study demonstrated significant differences in AKS knee score and ROM. No significant difference was found in Lysholm score and AKS function score. It is a consensus that reliable and accurate deformity correction leads to excellent clinical outcomes. Therefore, patients in the navigated group can be expected to achieve better functional results in the long term. In a study with a medium-term follow-up, 22 of the 23 patients who underwent computer-assisted osteotomy were satisfied or very satisfied with the results [Citation28]. Ribeiro et al. reported the navigated had significantly better Lysholm scores than the conventional group [Citation4]. Nonetheless, Neri et al. found no statistically significant differences in International Knee Documentation Committee (IKDC) and the Knee injury and Osteoarthritis Outcome Scores (KOOS), and the Western Ontario and McMaster Universities (WOMAC) [Citation2]. The clinical benefits of navigated system remain unclear. Further clinical follow-up and high quality RCTs are required to discuss ideal alignment and better clinical outcomes [Citation7,Citation31,Citation32].
Although the navigated system has potentially accurate and reproducible gain in the correction of the malalignment, the longer operative time has been a major criticism of the navigated HTO. In our meta-analysis, the mean operative time in navigated group was 15.46 min longer than in the conventional group. But the overall effect of operative time was not performed owing to the high heterogeneity. Two additional scars from the stab incisions for the rigid bodies, fasten position transmitters to the limb, registrar anatomic landmarks, and technical difficulties associated with calibrating the system contributed to longer operative time [Citation9,Citation30]. Despite the longer operation time in the navigated group, our study found there were no differences between the two groups in terms of complications (hardware removal, delayed union, wound hematoma, infection, osteoarthritis progression requiring conversion to TKA and et al.), delayed union, and reoperation (hardware removal, osteoarthritis progression requiring conversion to TKA, nonunion requiring a revision, and et al.).
The key aspects for future research
(1) Further clinical follow-up and high-quality RCTs are needed. (2) Surgeons should use the same plates to stable the osteotomies and the same bone substitutes to fill the osteotomy gap. (3) Considering limb rotation, computed tomography (CT) evaluation would be required. (4) The length of hospital days and socioeconomic cost-effectiveness of the navigated system are desirable. (5) We should compare the navigated HTO and the novel techniques, such as computer-assisted double-level osteotomy and patient-specific 3D-printed guides.
Several limitations should be considered
(1) There were only three RCTs in our study and some included studies were of the low-level evidence, which may affect the accuracy of the pooled results. (2) In this meta-analysis, the outcomes of outliers of aimed limb alignment, total complications, and reoperation are of high heterogeneity. The different of plate, radiographic parameters, navigated-assisted systems, surgical techniques, and radiographic measuring methods were considered as the reasons. But we cannot perform subgroup analysis of these factors due to a lack of data. (3) Few studies had sufficient sample size and postoperative follow-up time, which was the main reason for limiting us to obtaining more rigorous and convincing outcomes. (4) Among the included studies in our study, most were conducted by experienced surgeons. Hence, the result of this study cannot be generalized to every surgeon. (5) Publication bias may exist.
Conclusions
Navigated HTO provided more accurate and reproducible radiographic outcomes in the correction of the malalignment than conventional techniques, and there is no difference in the risk of complications compared with conventional HTO. However, it is unclear whether navigation HTO can achieve better clinical results. More randomized controlled trials (RCTs) with high quality, large sample size and sufficient follow-up period are required.
Author contributions
YQ and XK conceived of the design of the study. WQ and SJ participated in the literature search, study selection, data extraction and quality assessment. FC, ST, WX, WW, and SY participated in the design of the study and performed the statistical analysis. XK finished the manuscript. All authors read and approved the final manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Stanley JC, Robinson KG, Devitt BM, et al. Computer assisted alignment of opening wedge high tibial osteotomy provides limited improvement of radiographic outcomes compared to flouroscopic alignment. Knee. 2016;23(2):63–294.
- Neri T, Myat D, Parker D. The use of navigation in osteotomies around the knee. Clin Sports Med. 2019;38(3):451–469.
- Van Genechten W, Van Tilborg W, Van den Bempt M, et al. Feasibility and 3D planning of a novel patient-specific instrumentation technique in medial opening-wedge high tibial osteotomy. The Journal of Knee Surgery. 2021:34(14);1560–1569.
- Ribeiro CH, Severino NR, Fucs P. Opening wedge high tibial osteotomy: navigation system compared to the conventional technique in a controlled clinical study. Int Orthop. 2014;38(8):1627–1631.
- Saragaglia D, Sigwalt L, Rubens-Duval B, et al. Concept of combined femoral and tibial osteotomies. J Knee Surg. 2017;30(8):756–763.
- Lee DK, Wang JH, Won Y, et al. Preoperative latent medial laxity and correction angle are crucial factors for overcorrection in medial open-wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2020;28(5):1411–1418.
- Na YG, Eom SH, Kim SJ, et al. The use of navigation in medial opening wedge high tibial osteotomy can improve tibial slope maintenance and reduce radiation exposure. Int Orthop. 2016;40(3):499–507.
- Akamatsu Y, Kobayashi H, Kusayama Y, et al. Comparative study of opening-wedge high tibial osteotomy with and without a combined computed tomography-based and image-free navigation system. Arthroscopy. 2016;32(10):2072–2081.
- Maurer F, Wassmer G. High tibial osteotomy: does navigation improve results? Orthopedics. 2006;29(10 Suppl):S130–S132.
- Nha KW, Shin YS, Kwon HM, et al. Navigated versus conventional technique in high tibial osteotomy: a meta-analysis focusing on weight bearing effect. Knee Surg Relat Res. 2019;31(2):81–102.
- Wu ZP, Zhang P, Bai JZ, et al. Comparison of navigated and conventional high tibial osteotomy for the treatment of osteoarthritic knees with varus deformity: a meta-analysis. Int J Surg. 2018;55:211–219.
- Kim HJ, Yoon JR, Choi GW, et al. Imageless navigation versus conventional open wedge high tibial osteotomy: a meta-analysis of comparative studies. Knee Surg Relat Res. 2016;28(1):16–26.
- Bae DK, Ko YW, Kim SJ, et al. Computer-assisted navigation decreases the change in the tibial posterior slope angle after closed-wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2016;24(11):3433–3440.
- Gong J, Li Q, Wei M, et al. Effect of Tongluozhitong prescription-assisted intra-articular injection of sodium hyaluronate on VAS score and knee Lysholm score in patients with knee osteoarthritis. Evid Based Complement Alternat Med. 2021;2021:3210494.
- Saragaglia D, Chedal-Bornu B, Rouchy RC, et al. Role of computer-assisted surgery in osteotomies around the knee. Knee Surg Sports Traumatol Arthrosc. 2016;24(11):3387–3395.
- Reddy KI, Johnston LR, Wang W, et al. Does the oxford knee score complement, concur, or contradict the American Knee Society Score? J Arthroplast. 2011;26(5):714–720.
- Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–384.
- Stang A. Critical evaluation of the Newcastle-Ottawa Scale for the assessment of the quality of nonrandomized studies in Meta-analyses. Eur J Epidemiol. 2010;25(9):603–605.
- Furlan AD, Pennick V, Bombardier C, Editorial Board, Cochrane Back Review Group, et al. 2009 Updated method guidelines for systematic reviews in the Cochrane back review group. Spine. 2009;34(18):1929–1941.
- Prymka M, Hassenpflug J. High tibial osteotomy with a kinematic navigation system. Tech Orthopaed. 2003;18(2):209–215.
- Panzica M, Westphal R, Citak M, et al. Intraoperative computer-assisted prediction of intraarticular contact pressures in the knee during high tibial osteotomy. Int J Med Robot Comput Assist Surg. 2019;15(2):e1972.
- Lützner J, Gross AF, Günther KP, et al. Precision of navigated and conventional open-wedge high tibial osteotomy in a cadaver study. Eur J Med Res. 2010;15(3):117–120.
- Hankemeier S, Hufner T, Wang G, et al. Navigated open-wedge high tibial osteotomy: advantages and disadvantages compared to the conventional technique in a cadaver study. Knee Surg Sports Traumatol Arthrosc. 2006;14(10):917–921.
- Keppler P, Gebhard N, Grutzner PA, et al. Computer aided high tibial open wedge osteotomy. Inj Int J Care Injured. 2004;35(1):68–78.
- Bae DK, Song SJ, Kim KI, et al. Mid-term survival analysis of closed wedge high tibial osteotomy: a comparative study of computer-assisted and conventional techniques. Knee. 2016;23(2):283–288.
- Bae DK, Song SJ, Yoon KH. Closed-wedge high tibial osteotomy using computer-assisted surgery compared to the conventional technique. J Bone Joint Surg. 2009;91-B(9):1164–1171.
- Tsuji M, Akamatsu Y, Kobayashi H, et al. Joint line convergence angle predicts outliers of coronal alignment in navigated open-wedge high tibial osteotomy. Arch Orthop Trauma Surg. 2020;140(6):707–715.
- Saragaglia D, Chedal-Bornu B. Computer-assisted osteotomy for valgus knees: medium-term results of 29 cases. Orthop Traumatol Surg Res. 2014;100(5):527–530.
- Akamatsu Y, Mitsugi N, Mochida Y, et al. Navigated opening wedge high tibial osteotomy improves intraoperative correction angle compared with conventional method. Knee Surg Sports Traumatol Arthrosc. 2012;20(3):586–593.
- Chang J, Scallon G, Beckert M, et al. Comparing the accuracy of high tibial osteotomies between computer navigation and conventional methods. Comput Assist Surg. 2017;22(1):1–8.
- Iorio R, Pagnottelli M, Vadalà A, et al. Open-wedge high tibial osteotomy: comparison between manual and computer-assisted techniques. Knee Surg Sports Traumatol Arthrosc. 2013;21(1):113–119.
- Kim SJ, Koh YG, Chun YM, et al. Medial opening wedge high-tibial osteotomy using a kinematic navigation system versus a conventional method: a 1-year retrospective, comparative study. Knee Surg Sports Traumatol Arthrosc. 2009;17(2):128–134.
- Reising K, Strohm PC, Hauschild O, et al. Computer-assisted navigation for the intraoperative assessment of lower limb alignment in high tibial osteotomy can avoid outliers compared with the conventional technique. Knee Surg Sports Traumatol Arthrosc. 2013;21(1):181–188.
- Saragaglia D, Roberts J. Navigated osteotomies around the knee in 170 patients with osteoarthritis secondary to genu varum. Orthopedics. 2005;28(10):S1269–S1274.
- Schroter S, Ihle C, Elson DW, et al. Surgical accuracy in high tibial osteotomy: coronal equivalence of computer navigation and gap measurement. Knee Surg Sports Traumatol Arthrosc. 2016;24(11):3410–3417.
- Zarrouk A, Bouzidi R, Karray B, et al. Distal femoral varus osteotomy outcome: is associated femoropatellar osteoarthritis consequential? Orthop Traumatol Surg Res. 2010;96(6):632–636.
- Marin Morales LA, Gomez Navalon LA, Zorrilla Ribot P, et al. Treatment of osteoarthritis of the knee with valgus deformity by means of varus osteotomy. Acta Orthop Belg. 2000;66(3):272–278.