
Abstract
Improving surgical training by means of technology assistance is an important challenge that aims to directly impact surgical quality. Surgical training includes the acquisition of two categories of knowledge: declarative knowledge (i.e. ‘knowing what’) and procedural knowledge (i.e. ‘knowing how’). It is essential to acquire both before performing any particular surgery. There are currently many tools for acquiring procedural knowledge, such as simulators. However, few approaches or tools allow a trainer to formalize and record surgical declarative knowledge, and a trainee to have easy access to it. In this paper, we propose an approach for structuring surgical declarative knowledge according to procedural knowledge and based on surgical process modeling. A dedicated software application has been implemented. We evaluated the concept and the software usability on two procedures with different medical populations: endoscopic third ventriculostomy involving 6 neurosurgeons and preparation of a surgical table for craniotomy involving 4 scrub nurses. The results of both studies show that surgical process models could be a well-adapted approach for structuring and visualizing surgical declarative knowledge. The software application was perceived by neurosurgeons and scrub nurses as an innovative tool for managing and presenting surgical knowledge. The preliminary results show that the feasibility of the proposed approach and the acceptability and usability of the corresponding software. Future experiments will study impact of such an approach on knowledge acquisition.
1. Introduction
Learning and training are key to ensuring quality in medicine and surgery. Trainee surgeons have to digest a huge amount of knowledge before being allowed to practice. Such knowledge comes usually from literature, observations in the operating room, and from experts [Citation1]. Such knowledge is mainly divided into two types [Citation2]:
Declarative knowledge which can be characterized as ‘knowing what’, for example, anatomy, physiology, pathology, the identity of particular surgical instruments and their functions, …
Procedural knowledge which can be characterized as ‘knowing how’, that is, how to execute a specific action in a particular situation to reach a specific goal.
Both types of knowledge are essential to acquire before a resident can actually practice, leading to the manta ‘never the first time on a patient’ [Citation3]. Thus, technology assistance in training has been an important challenge for addressing several related issues ranging from patient safety to economic considerations. These include limiting the number of serious adverse events [Citation4], managing the increase of surgical procedures along with the decrease of available trainers, developing of multipurpose operating rooms where the surgical staff has to be trained for different surgical contexts and procedures; and accelerating learning curve on new and emerging surgical devices and practices, such as robotic or computer assisted surgery [Citation5].
Recent work on simulation systems has focus more on imparting procedural knowledge. Simulation systems are generally divided between organic and non-organic systems [Citation5–7]. Organic systems include those that have a physical body on which the trainee practices. This physical body can include animal tissue or synthetic materials mimicking human anatomy (also called bench-top models). Certain high-fidelity tissue models such as live animals, cadavers, and certain high-fidelity synthetic models mimic (almost) the entire relevant anatomy and physiology. Non-organic training systems are based on virtual reality (VR). VR systems often focus on a specific task such as suturing or cutting, and some are coupled with a high fidelity physical models of the patient anatomy, or of the effects of otherwise virtual surgical tools on tissue [Citation8,Citation9].
Surgical declarative knowledge is complex and heterogeneous. It includes general knowledge about concepts involved in surgical procedures, such as anatomy, pathology, and clinical outcomes. It also includes more specific concepts related to the surgical steps, such as which instruments are used, guidelines for perfoming a gesture at a given time, and the sequential order of steps to be performed. Many materials are available to acquire this knowledge such as books, scientific papers, oral experts’ advices, institution instructions, videos, and educational websites. By their very nature, simulation systems also implicitly impart some declarative knowledge, such as the instruments and their function as it is mimicked by the simulator itself. However, the level of this knowledge is limited by the complexity of their design, as they cannot mimic the full complexity of human anatomical and physiological systems and their interaction during surgery, especially outside of the pre-defined boundaries of the simulation.
To the best of our knowledge, there is a lack of formal approaches and corresponding tools for bringing together these heterogeneous and multimodal sources of information to enhance declarative knowledge learning. In this paper, we propose a formal approach to fill this lack via a dedicated software application, Surge Train. The software was adapted for two procedures: endoscopic third ventriculostomy (ETV) and the preparation of a surgical table for craniotomy (PSTC). In this article, the usability, and acceptability of the concept and the corresponding software tool have been evaluated by six neurosurgeons for ETV and four scrub nurses for PSTC.
2. Materials and methods
We propose an approach allowing a trainer to structure the data, and a trainee to learn declarative knowledge. First, the structuration of declarative knowledge is presented. The software application based on this structure is introduced. Finally, two usability studies are presented.
2.1. Structuration of declarative knowledge
Structuration of knowledge is crucial for recording and visualizing concepts associated to a surgical procedure. In this paper, we used Surgical Process Model (SPM) methodology for structuring the knowledge, i.e. to formalize semantic description of surgical procedures as a list of phases, steps, and activities [Citation10,Citation11]. This allows, for the trainer to organize knowledge with respect to phases and steps, and allows for the learner to easily access to the information in a logical, task-oriented, and comprehensive manner. The procedure was modeled as a list of phases, each described via text and including a list of steps. A step included a list of information and a list of multimedia documents illustrating concepts related to this information. Both phase and step names were defined from a SPM which could be a recording of actual procedures either intraoperatively, by observing the medical staff, or postoperatively according to videos of the procedure [Citation12,Citation13]. For each step, according to their purpose within the surgical procedure, knowledge is classified into six different categories: Trajectory (i.e. knowledge related to accessing the target), Area to be avoided (i.e. knowledge related to the avoidance of critical healthy anatomical areas that need to be preserved during surgery), Target Area (i.e. knowledge related to targeted structure which the main objective of the surgical procedure), Reference Area (i.e. knowledge related to the areas which may help the surgeon to understand where he/she is, such as structures that will be visible on the way to the target), Instrument of interest (i.e. knowledge related to surgical instruments or devices involved in the surgical procedure), or Patient Data (i.e. knowledge related to general patient data and characteristics). Many types of multimedia data can be included in each knowledge category for illustration purposes, as videos, images, textual comments, documents, or web links.
2.2. The software application: surge train
We implemented declarative knowledge learning software based on procedural modeling. The procedure was presented as a sequence of phases placed along a vertical line. These phases were also visualized as a horizontal list at the top of the window and allowed the user to select a phase to fill or observe. Surge Train was composed of two modes: the edit and training modes for the trainer and the learner respectively.
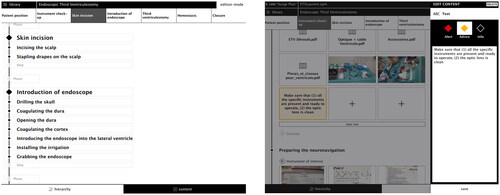
The edit mode was developed for the trainer to describe a procedure. This mode had two views. The hierarchy view allowed to describe the list and order of phases and steps (, left). The content view allowed the expert to add all relevant knowledge associated to the steps according to the different categories with corresponding multimedia documents (, right).
Figure 1. Edit mode for ETV procedure.
The training mode allowed a trainee to access knowledge and corresponding multimedia data, either general or step-specific and structured following the SPM ( and ). This data was easily visualized according to their format: a video can be launched, a picture can be view, and web links can be opened in a web navigator ().
Figure 2. Surgical declarative knowledge assigned to phases and steps of ETV procedure.
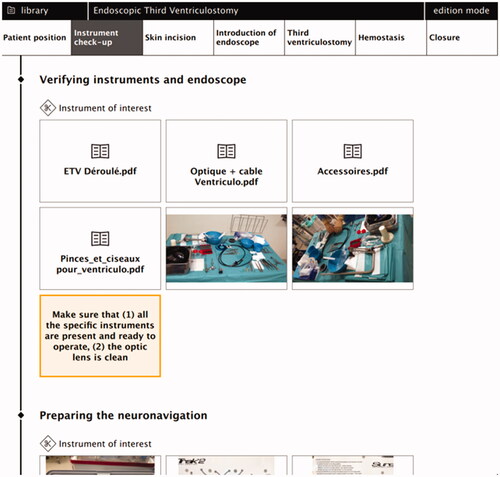
Figure 3. Surgical declarative knowledge assigned to phases and steps in the PSTC procedure.
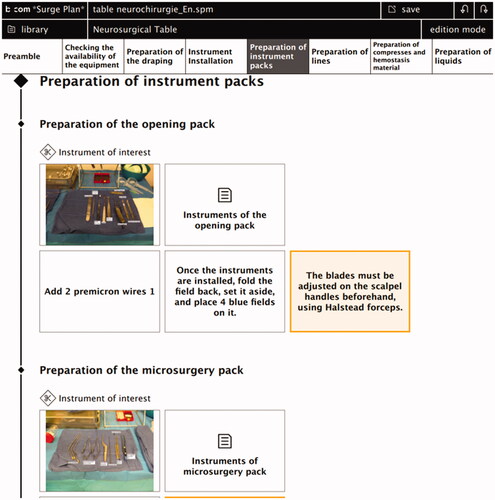
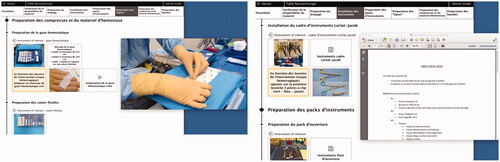
Figure 4. Surgical declarative knowledge assigned to phases and steps of PSTC with multimedia documents opened (video and pdf) in French version.
2.3. Evaluation study
We implemented our approach for two procedures: the endoscopic third ventriculostomy (ETV) and the preparation of a surgical table for craniotomy (PSTC). Firstly, using the edit mode, the ETV procedure was described by an expert neurosurgeon and the PSTC by an expert scrub nurse, both relying on video recording of actual procedures (one for ETV and 2 for PSTC). These videos were used to help experts to structure their knowledge, when particularities as deviations or adverse events occurred, they focused on the description of the standard process. Both experts had no time limits for describing the procedures. Secondly, a total of 10 health care professionals were involved in assessing the usability and acceptability of the training mode: 6 neurosurgeons for ETV and 4 scrub nurses for PSTC which are described in and , respectively.
Table 1. Users profiles for the ETV procedure.
Table 2. Users profiles for the PSTC procedure.
2.3.1. Description of procedures
Endoscopic third ventriculostomy (ETV) is a routine neurosurgical procedure mostly used to treat obstructive hydrocephalus both in children and adults. ETV offers significant advantages over shunts and is considered the gold standard in the management of non-communicating hydrocephalus. Residents in neurosurgery have to learn and master this endoscopic technique as early as possible in their surgical curriculum. ETV is divided into five phases: (1) A burr-hole is performed in the right frontal bone (Kocher’s point); (2) A rigid endoscope is introduced through the right frontal lobe into the right frontal horn of the lateral ventricle; (3) insertion of the endoscope into the third ventricle through the foramen of Monro; (4) perforation of the floor of the third ventricle. This communication between the third ventricle and the subarachnoid cisterns allows the circulation of cerebrospinal fluid trapped in the ventricles to the subarachnoid space. Finally, (5) the endoscope is removed and the skin is closed.
Preparation of a surgical table for craniotomy (PSTC) is a procedure performed by a scrub nurse before a craniotomy. PSTC is divided into seven phases: (1) verification of the equipment ensuring that all materials and devices are available, unexpired, and sterile; (2) dapping of the microscope and the table; (3) Then install the frame of the surgical instrument; (4) preparation of two instrument packs for the opening and the microsurgery sequence, respectively; (5) the scrub nurse prepares the devices such as the drill and the electric scalpel; (6) preparation of compresses and hemostasis equipment; (7) preparation of liquids including local anesthesia and skin disinfection solutions.
2.3.2. Protocol
In order to assess the concept and the software acceptability, and usability, we used the Unified Theory of Acceptance and Use of Technology (UTAUT) and the AttrakDiff surveys. These standard tools are detailed in the next sections.
Test sessions were managed by an ergonomist, each consisting of a single session with a single participant. First, the study and the software are presented to the participant. During this stage, they could ask questions about the software. Then they complete a pre-interaction UTAUT survey. After this survey, the participants use the software with full autonomy, i.e. without any assistance or time constraints. Finally, the participants evaluated the software by completing a post-interaction UTAU survey and the AttrakDiff survey.
2.3.2.1. UTAUT survey
The survey has been defined according to the UTAUT framework formulated by Venkatesh et al. in 2003 [Citation14], and was composed of 26 questions relative to the following dimensions:
Performance expectancy: ‘the degree to which an individual believes that using the system will help him or her to attain gains in job performance’ [Citation14];
Effort expectancy: ‘the degree of ease associated with the use of the system’ [Citation14];
Social influence: ‘the degree to which an individual perceives that important others belies he or she should use the new system’ [Citation14];
Facilitating conditions: ‘the degree to which an individual believes that an organizational and technical infrastructure exists to support the use of the system’ [Citation14];
Behavioral intention: the subjective likelihood that an individual will engage in the behavior in question [Citation15].
This survey was filled in by the participants twice, the pre-iteration survey is used as a baseline to compensate for the different individual technology familiarity and anxiety levels of participants, and the post-interaction survey is used to assess acceptability. Survey answers were given on the Likert scale ranging from 1 (Not agree at all) to 7 (Totally agree) [Citation16].
2.3.2.2. AttrakDiff survey
The AttrakDiff survey, defined by Hassenzahl [Citation17], has been extended in order to measure subjective assessment concerning pragmatic and hedonic qualities, and the attractiveness of the products (i.e. complicated vs. simple, cheap vs. premium, conservative vs. innovative or ugly vs. attractive). Our survey was composed of 28 questions which aimed to evaluate the following product dimensions:
The Pragmatic Quality (PQ) describes the usability of a product and indicates how successfully users are in achieving their goals using the product (a measure of usability);
The Hedonic Quality – Stimulation (HQ-S) indicates to what extent the product can support the stimulation needs by providing interesting and stimulating functions and contents (a measure of utility);
The Hedonic Quality – Identity (HQ-I) indicates to what extent the product allows the user to identify with it (a measure of utility);
The Attractiveness (ATT) describes the global value of the product based on the quality perception (a measure of acceptability).
This survey was filled by users after interaction with Surge Train. Again the survey answers were given on the Likert scale ranging from −3 (highly negative perception) to 3 (highly positive perception) [Citation16].
3. Results
The results provided by the surveys have been summarized below.
3.1. UTAUT survey
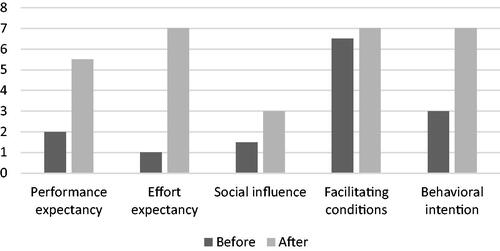
and show the median of answers of the pre- and post-interaction UTAUT surveys for the different dimensions and for the ETV and PSTC procedures, respectively. Overall, the perception participants had about the system were improved through the interaction with the Surge Train software, which highlighted better usability and acceptability than expected by participants before the interaction. This is more significant for the scrub nurses.
Figure 5. Median of UTAUT answers before and after interaction with Surge Train for ETV.
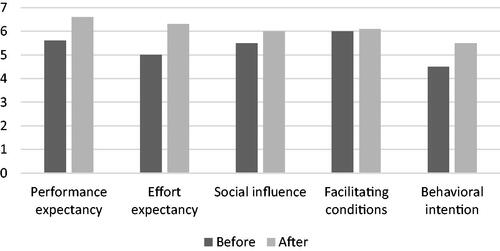
Figure 6. Median of UTAUT answers before and after interaction with Surge Train for PSTC.
3.2. AttrakDiff
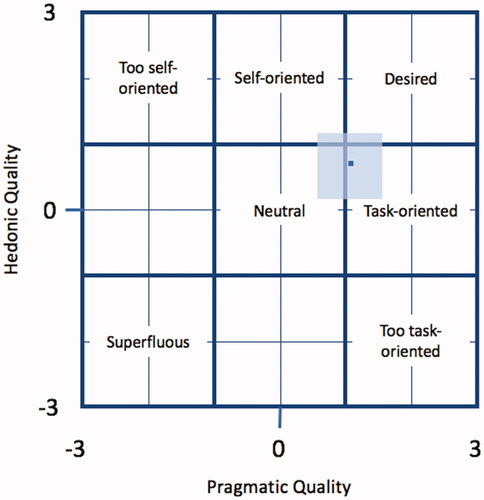
and show the score of the AttrakDiff survey for the ETV and PSTC procedure respectively. In each the horizontal axis corresponds to the value of the pragmatic scale and the vertical axis represents the three hedonic scales. The software was perceived as desired by the surgeon, and task-oriented for the scrub nurses.
Figure 7. AttrakDiff score of ETV.
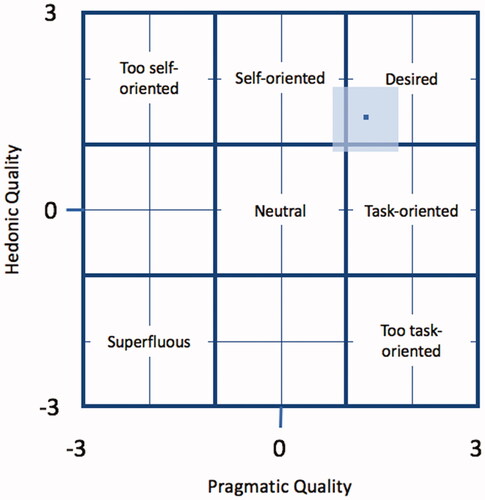
Figure 8. AttrakDiff score of PSTC.
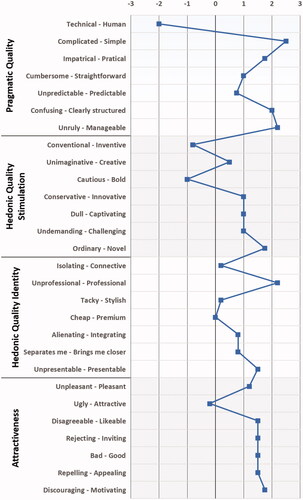
and show the pragmatic and hedonic qualities of all participants. The values near the neutral zone (between 0 and 1) are considered standard, i.e. the product is compliant with its objective, no more, no less. The values outside of this neutral zone should be considered positive (between 1 and 3) or negative (between −3 and −1). shows that the solution was perceived by neurosurgeons as simple, clear, manageable, original, innovative, stimulating, new, professional, presentable, pleasant, nice, and attractive, but also not captivating and boring. shows that the solution was perceived by scrub nurses as simple, practical, structured, manageable, professional, presentable, original, innovative, novel, pleasant, and motivating, but also very technical. Scrub nurses found the software less attractive than the surgeons. Both found it strongly task-oriented, which is the basic purpose of the software.
Figure 9. Average responses from the AttrakDiff survey for ETV.
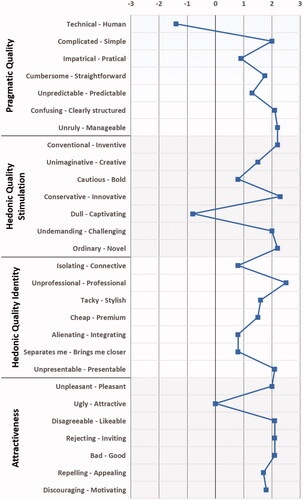
Figure 10. Average responses from the AttrakDiff survey for PSTC.
4. Discussion and conclusion
In this paper, we proposed a tool to assist in the representation and acquisition of declarative knowledge. The usability and acceptability of the approach as well as the software tool were evaluated in the context of a neurosurgical procedure by six neurosurgeons and neurosurgical table preparation by four scrub nurses. Initial results demonstrated the feasibility and interest of this approach and corresponding software.
UTAUT scores demonstrated that all participants had a strongly positive perception of the usefulness of Surge Train. This software was perceived as an easy-to-use tool. In the traditional declarative knowledge process, neurosurgery students and residents have several clinical and scientific papers to read in order to learn said knowledge. However, this knowledge is rarely organized following a procedural structure. Scrub nurses have fewer materials for such purposes. The available ones often have an informal or ad-hoc structure. Surge Train is therefore perceived, by both populations, as an innovative tool allowing them to centralize information previously defined and validated by experts. Before interacting with Surge Train software, UTAUT scores by neurosurgeons had higher values than those from scrub nurses, indicating an a priori higher willingness to use said software. This ma be because neurosurgeons are often more familiar with newer technologies and thus better anticipated the potentiality of the software, whereas tasks for scrub nurses have traditionally been less amenable to computerization, leading to a stronger apprehension.
The answers observed from the AttrakDiff survey indicated that the participants had a positive experience with Surge Train. Results highlighted the Hedonic Quality - Identity (HQ-I), which indicated to what extent the product could allow the user to identify with it, i.e. the capacity of the system to stimulate the user and encourage exploration. This could be explained by the fact that this was a professional tool and therefore exists in a more task-oriented context. The solution has been perceived by both populations as simple, innovative, and professional, but also as not captivating and boring. This was mainly due to the fact that the learner was maybe relatively passive during such learning. Scrub nurses found the software less attractive than the surgeons who found better hedonic quality. For that, improvements are to be made on the presentation and the esthetics of the software, as well as on the stimulation brought to users. This is part of the perspective and will involve a user interface expert.
The number of participants in this study was however limited. More participants need to be included in future studies. However, the advantages have been already clearly highlighted.
Our software application was based on SPMs, more specifically iSPMs (individual Surgical Process Models) [Citation10], i.e. the model of a single procedure. In this study, the trainers described the procedure without taking into account deviations or adverse events which can occur during the procedure. Moreover, the description was made by only one expert for each procedure, so the description represents his/her perception of the procedure. Future works have to take into account the occurring of such events and a multi-experts vision by relying on generic SPMs. A generic SPM (gSPM) is a model of a procedure representing observed variability through different clinical cases [Citation10]. The recruitment of other experts will also allow us to study the acceptability of the software for the editing mode which was not part of the current study.
Finally, to easily share knowledge and corresponding data associated with declarative knowledge, an ontology as OntoSPM [Citation18,Citation19] could be used. Thanks to the semantic reasoning inherent in an ontology, it would be possible to ensure the standardization of vocabulary and the semantics, facilitating the communication of more complex declarative knowledge between the software and the user as well as amongst users.
In conclusion, these results have shown that the concept and the software application allow for the structuring of surgical declarative knowledge about specific surgical procedures, and, provides trainees with easy access to it. It could also help the optimization and standardization of declarative knowledge learning. Future work will focus on the evaluation of the added value of Surge Train compared to traditional declarative knowledge learning processes.
Ethical approval
All procedures involving human participants have been approved and performed in accordance with ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Disclosure statement
A. HUAULMÉ, P. JANNIN, B. LABBE, M. GELIN, C. CHESNEAU, J.M. DIVERREZ, L. RIFFAUD, and G. DARDENNE declare that they have no conflict of interest.
References
- Witte TEF. Requirements for efficient robotic surgery training [Master thesis]. University of Twente; 2015.
- Van Merriënboer JJG. Training complex cognitive skills: a four-component instructional design model for technical training. Englewood Cliffs (NJ): Educational Technology Publications; 1997.
- Arora S, Aggarwal R, Sirimanna P, et al. Mental practice enhances surgical technical skills: a randomized controlled study. Ann Surg. 2011;253(2):265–270.
- Leape LL, Berwick DM. Five years after to err is human: what have we learned? J Am Med Assoc. 2005;293(19):2384–2390.
- Gallagher AG, O’Sullivan GC. Fundamentals of surgical simulation: principles and practice. New York (NY): Springer; 2012.
- Spruit EN, Band GPH, Hamming JF, et al. Optimal training design for procedural motor skills: a review and application to laparoscopic surgery. Psychol Res. 2014;78(6):878–891.
- Sturm LP, Windsor JA, Cosman PH, et al. A systematic review of skills transfer after surgical simulation training. Ann Surg. 2008;248(2):166–179.
- Larsen CR, Soerensen JL, Grantcharov TP, et al. Effect of virtual reality training on laparoscopic surgery: randomised controlled trial. BMJ. 2009;338(may14 2):b1802–b1802.
- Seymour NE, Gallagher AG, Roman SA, et al. Virtual reality training improves operating room performance results of a randomized, double-blinded study. Ann Surg. 2002;236(4):458–464.
- Lalys F, Jannin P. Surgical process modelling: a review. Int J Comput Assist Radiol Surg. 2014;9(3):495–511.
- Jannin P, Morandi X. Surgical models for computer-assisted neurosurgery. Neuroimage. 2007;37(3):783–791.
- Garraud C, Gibaud B, Penet C, et al. An ontology-based software suite for the analysis of surgical process model. In: Proceedings of Surgetica’2014; Chambery, France. 2014. p. 243–245. https://hal.archives-ouvertes.fr/hal-01100508
- Neumuth T, Jannin P, Strauss G, et al. Validation of knowledge acquisition for surgical process models. J Am Med Inform Assoc. 2009;16(1):72–80.
- Venkatesh V, Morris MG, Davis GB, et al. User acceptance of information technology: toward a unified view. MIS Q Manag Inf Syst. 2003;27(3):425–478.
- Fishbein MA, Ajzen I. Belief, attitude, intention and behaviour: an introduction to theory and research. Reading (MA): Addison-Wesley; 1975.
- Likert R. A technique for the measurement of attitudes. Arch Psychol. 1932;22:5–55. https://psycnet.apa.org/record/1933-01885-001
- Hassenzahl M, Burmester M, Koller F. AttrakDiff: Ein Fragebogen zur Messung wahrgenommener hedonischer und pragmatischer Qualität. Mensch Comput. 2003;187–196. Berichte des German Chapter of the ACM, vol 57. Vieweg+Teubner Verlag. doi:10.1007/978-3-322-80058-9_19
- Gibaud B, Forestier G, Feldmann C, et al. Toward a standard ontology of surgical process models. Int J CARS. 2018:13;1397–1408. doi:10.1007/s11548-018-1824-5.
- Katić D, Julliard C, Wekerle A-L, et al. LapOntoSPM: an ontology for laparoscopic surgeries and its application to surgical phase recognition. Int J Comput Assist Radiol Surg. 2015;10(9):1427–1434.