
Abstract
BACKGROUND: Chronic hypercapnic respiratory failure is common in advanced chronic obstructive pulmonary disease (COPD) and it is associated with adverse outcomes such as repeat hospitalization and death. Long-term non-invasive ventilation (NIV) has been used with uncertain efficacy in this condition, but recent clinical trials suggest possible survival benefit and reduced hospitalization under specific circumstances with this therapy.
METHODS: The purpose of this guideline update is to assess current evidence regarding long-term NIV in the treatment of chronic hypercapnic respiratory failure specifically related to advanced COPD. A representative multidisciplinary panel of expert clinicians undertook a formal clinical practice guideline development process. Four key clinical questions were defined according to the Patient/problem, Intervention, Comparison, Outcome (PICO) approach. The panel performed a systematic literature review, assessed and graded the relevant evidence and made evidence-based recommendations.
RESULTS: There is supportive evidence for the use of long-term NIV to improve survival in patients with stable COPD with significant chronic hypercapnic respiratory failure. The use of this therapy may also lead to reduced hospital readmission rates when applied to patients who were recently hospitalized for an acute hypercapnic exacerbation and in whom the elevated partial pressure of carbon dioxide in arterial blood (PaCO2) persists 2 to 4 weeks after the index hospitalization. Studies demonstrating benefit of long-term NIV targeted very selected patient populations and used very specific methodology, both of which are likely key elements for NIV success.
Although there is no evidence from clinical trials directly comparing high-intensity versus low-intensity NIV, most successful clinical trials have used the former ventilation strategy. Therefore, when opting for long-term NIV in patients with COPD and chronic hypercapnic respiratory failure, we suggest using high-intensity ventilation (sufficient inspiratory pressures to meaningfully reduce PaCO2). We found no evidence to support the use of volume-assured pressure ventilation over standard pressure preset ventilation, which is currently the preferred mode.
CONCLUSIONS: This 2021 guideline update represents an important shift from the previous recommendation against the use of long-term NIV in most patients with COPD and chronic hypercapnia, toward its suggested use. Based on the reported survival and hospital readmission rate benefits, we suggest long-term NIV in highly selected patients with COPD and chronic hypercapnic respiratory failure along with the use of specific and closely monitored ventilatory strategies.
RÉSUMÉ
CONTEXTE: L’insuffisance respiratoire hypercapnique chronique est courante dans la maladie pulmonaire obstructive chronique (MPOC) avancée et elle est associée à des résultats indésirables tels que des hospitalisations répétées et même la mort. La ventilation non invasive à long terme (VNI) a été utilisée avec une efficacité incertaine pour ce problème de santé, mais des essais cliniques récents indiquent un avantage possible en matière de survie et une hospitalisation réduite dans des circonstances précises avec ce traitement.
MÉTHODES: Le but de cette mise à jour des lignes directrices est d’évaluer les données probantes actuelles concernant la VNI à long terme dans le traitement de l’insuffisance respiratoire hypercapnique chronique spécifiquement liée à la MPOC avancée. Un groupe multidisciplinaire représentatif de cliniciens experts a entrepris un processus d’élaboration de lignes directrices de pratique clinique. Quatre questions cliniques clés ont été définies selon l’approche Patient / problème, Intervention, Comparaison, Résultat (PICO). Le comité a effectué une revue systématique de la littérature, évalué et noté les données probantes pertinentes et formulé des recommandations fondées sur des données probantes.
RÉSULTATS: Il existe des données probantes à l’appui de l’utilisation de la VNI à long terme pour améliorer la survie chez les patients atteints de MPOC stable avec une insuffisance respiratoire hypercapnique chronique significative. L’utilisation de ce traitement peut également conduire à une réduction des taux de réadmission à l’hôpital lorsqu’elle est appliquée à des patients récemment hospitalisés pour une exacerbation hypercapnique aiguë et chez lesquels la pression partielle élevée de dioxyde de carbone dans le sang artériel (PaCO2) persiste deux à quatre semaines après l’hospitalisation de référence. Les études démontrant les avantages de la VNI à long terme ont ciblé des populations de patients très sélectionnées et ont utilisé une méthodologie très précise, qui sont probablement des éléments clés du succès de la VNI.
Bien qu’il n’y ait aucune donnée probante provenant d’essais cliniques comparant directement la VNI de haute intensité et de faible intensité, la plupart des essais cliniques réussis ont utilisé l’ancienne stratégie de ventilation. Par conséquent, lorsque la VNI à long terme est retenue pour traiter les patients atteints de MPOC et d’insuffisance respiratoire hypercapnique chronique, nous suggérons d’utiliser une ventilation à haute intensité (pressions inspiratoires suffisantes pour réduire significativement la PaCO2). Nous n’avons trouvé aucune donnée probante pour soutenir l’utilisation de la ventilation à pression à volume garanti par rapport à la ventilation à pression prédéfinie standard, qui est actuellement le mode préféré.
CONCLUSIONS: Cette mise à jour des lignes directrices 2021 représente un changement important par rapport à la recommandation précédente contre l’utilisation de la VNI à long terme chez la plupart des patients atteints de MPOC et d’hypercapnie chronique, vers son utilisation suggérée. Sur la base des avantages rapportés en termes de survie et de taux de réadmission à l’hôpital, nous suggérons une VNI à long terme chez des patients hautement sélectionnés atteints de MPOC et d’insuffisance respiratoire hypercapnique chronique, ainsi que l’utilisation de stratégies ventilatoires particulières et étroitement surveillées.
Introduction
Chronic hypercapnic respiratory failure is a devastating consequence of severe chronic obstructive pulmonary disease (COPD).Citation1,Citation2 Chronic hypercapnia in COPD generally indicates advanced disease with limited survival, carrying a 1-year mortality rate of 17-30%.Citation3–7 The course of chronic hypercapnic respiratory failure is often characterized by bouts of acute-on-chronic respiratory failure that require repeated hospital admissions,Citation3,Citation4,Citation6–8 often in an intensive care unit. The in-hospital mortality in 1016 patients admitted with COPD exacerbations and hypercapnic respiratory failure (partial pressure of carbon dioxide in arterial blood [PaCO2] ≥ 50 mm Hg) was 11%; corresponding rates after 180 days and 2 years were 33% and 49%, respectively.Citation9 Hospital readmission is also a common occurrence after an index hospitalization for COPD. Data from the United States suggest that approximately 20% of patients with COPD are readmitted within 30 days; COPD was the most common reason for these readmissions while respiratory failure was present in 12%.Citation10
In addition to standard COPD care, long-term non-invasive ventilation (NIV) had been proposed several years ago as an attempt to alter the clinical course of patients with COPD and chronic hypercapnic respiratory failure. In contrast to acute hypercapnic respiratory failure due to an acute COPD exacerbation in which NIV has become standard of care,Citation11 the benefit of using long-term NIV to treat chronic hypercapnic respiratory failure in COPD has been inconsistent among studies. As a result, in many countries including Canada, this treatment is generally not provided in the latter context. This is in sharp contrast with many European countries where chronic hypercapnic respiratory failure associated with COPD is one of the most frequent indications for the initiation of long-term NIV.Citation12–14
Since the 2011 publication of the Canadian Thoracic Society (CTS) Clinical Practice Guideline (CPG) for home NIV,Citation15 important clinical trials have revealed new information necessitating an update to the current recommendations for NIV in COPD. This revised CPG deals specifically with chronic hypercapnic respiratory failure due to advanced COPD as opposed to other possible confounding conditions such as sleep apnea or obesity-related hypoventilation. Likewise, it does not address the treatment of acute respiratory failure in COPD.
The rationale for use of long-term NIV in patients with COPD and chronic hypercapnic respiratory failure is based on its presumed physiological efficacy to improve sleep time and efficiency,Citation16 restore respiratory muscle function by alleviating work of breathing and thereby providing rest,Citation17,Citation18 as well as reduce gas trapping and improve airway mechanics.Citation19 While this is acknowledged, the current CPG update is focused on the ability of long-term NIV to impact physiological and clinical outcomes such as blood gases, dyspnea, hospital readmission and mortality. We also reviewed the current literature regarding the choice of specific ventilatory parameter settings to deliver long-term NIV in patients with COPD and chronic hypercapnic respiratory failure.
Objectives
The primary objective of this CTS CPG is to provide updated clinical recommendations on the use of long-term NIV to treat chronic hypercapnic respiratory failure in COPD.
A secondary objective is to provide expert guidance for optimizing the use of long-term NIV to treat chronic hypercapnic respiratory failure in COPD, using an evidence-based approach and expert-informed clinical opinion.
Target patient population
The update applies to patients with severe COPD (forced expiratory volume in 1 s (FEV1) < 50% predicted) resulting in chronic hypercapnic respiratory failure who may be considered candidates for long-term NIV. Two target groups will be considered: those with severe COPD and hypercapnia who are stable, and those with persistent hypercapnia following a severe COPD exacerbation that required NIV in the acute setting.
Target users
The present CPG is intended for use by the health care teams that care for individuals with advanced COPD. Specifically, specialist physicians (respirologists and internists, and intensive care specialists), and other health care professionals (eg, respiratory therapists, nurses, physiotherapists) who are currently involved in the care for patients with advanced COPD, particularly those working in respiratory home care services. This document should also be useful to patients and patient advocates. Finally, health care decision-makers may also use this CPG in policy processes to inform decisions regarding the funding of devices and long-term NIV programs.
Differences from prior guideline published in 2011
This CPG represents an update from an earlier version published in 2011 by CTS.Citation15 In this update, we have performed a systematic review of the literature on the use of NIV to treat chronic hypercapnic respiratory failure in COPD. Major changes from the prior CPG include the following:
Based on this and prior literature, we provide updated clinical recommendations regarding the use of NIV to treat chronic hypercapnic respiratory failure in COPD, which are substantially different than the 2011 recommendations.
We have also reviewed evidence regarding the use of high-intensity versus low-intensity NIV and of other mechanical ventilation strategies in this situation.
We do not address the issue of chronic hypercapnia in COPD when potentially related to concomitant sleep apnea or obesity-related hypoventilation.
Methodology
Guideline panel composition
The CTS Home Mechanical Ventilation (HMV) guideline panel is interprofessional and is comprised of HMV clinicians and health care professionals with content expertise. The panel was co-chaired by (MK/FM) and included 7 adult respirologists, 1 physiatrist specializing in neuro-rehabilitation and 1 registered respiratory therapist. All author conflicts of interests are posted on the CTS website.
The CPG was developed in accordance with the CTS guideline development process (https://cts-sct.ca/guideline-library/methodology/). The panel used the AGREE II checklist to guide the development of the CPG.Citation20 Details of the search strategy, flow of citations and articles and the inclusion and exclusion criteria are outlined in Appendix 1.
Formulation of key clinical questions
The PICO method was used taking into consideration the Patient group or groups that should be addressed, the Intervention or interventions that should be examined, the Comparison groups that should be part of the studies of the various interventions and the Outcome or outcomes of interest. The panel developed PICO questions for 2 main categories: 1) assessment of benefit of long-term NIV in patients with a) stable severe COPD (FEV1 < 50% predicted), and b) patients with severe COPD recovering from an acute hypercapnic exacerbation; and 2) determination of optimal modes and settings of long-term NIV in COPD. A priori, through a consensus, the panel identified the following outcomes, which would take priority in guideline decision-making, and, therefore, in the GRADE evidence table: PICO 1 a) and b) (dyspnea, health-related quality of life (HRQoL), physiologic measures (PaCO2), hospitalization and survival); PICO 2 and 3 (dyspnea, HRQoL and physiologic measures). These were prioritized based on the panel’s opinion on the importance to patients and their impact on patient quality of life. Data on other outcomes (health care utilization) were also collected and considered, but not prioritized in recommendation generation due to lack of evidence.
Literature search and screening of abstracts
An initial literature search was conducted from June 1, 2010 to August 31, 2018 using MEDLINE (OVID), Embase (OVID), OVID Medline Epub Ahead of Print, In-Process & Other Non-Indexed Citations and the Cochrane Library; and selected relevant manuscripts included with publication dates up to November 2020. Articles from the previous CPG are referenced in this review. The title and abstracts of each article as well as the full text articles were scrutinized by 2 panel members (FM/MK-PICO 1a,1b, 2 and 3) to decide whether each article was relevant. Where there was a difference of opinion, the panel members endeavored to reach consensus. When a consensus was reached on the list of relevant abstracts, copies of the articles of all relevant and possibly relevant articles were obtained and reviewed by 2 panel members. Details of the flow of citations and articles and study inclusion and exclusion criteria are detailed in Appendix 1.
Study selection criteria
We included only RCTs for further review and inclusion. Other study designs and studies published in a language other than English were excluded. Each abstract and full text article was assessed by 2 reviewers (MK/FM) to determine if they were eligible (Appendix 1).
Risk of bias and critical appraisal of identified studies
Two panel members per area of focus were assigned to critically appraise and assess studies for risk of bias: PICO 1a, 1 b, 2, 3 (MK/FM). The Cochrane Risk of Bias ToolCitation21 for RCTs was used to assess the risk of bias in individual studies. In addition, literature previously identified and used for the previous CPGCitation15 was included for PICO 1a and 1 b. We compiled data from all articles relevant to each PICO question into GRADE evidence tables which are available on the CTS website. These GRADE evidence tables were developed by MK/FM. The entire panel then discussed each PICO question via webinars in March 2020, at which time all evidence tables were reviewed and agreed upon by the whole group.
Grading the evidence and formulation of recommendations
GRADE evidence profilesCitation22 were developed to rate the certainty of evidence for each outcome as high, moderate, low or very low. Evidence originating from RCTs was considered to be high-quality evidence as a starting point, but could be downgraded due to risk of bias. The quality of evidence across studies was assessed for methodological limitations, inconsistency, indirectness, imprecision, and publication bias. If the results were downgraded by 1 or 2 levels (serious or very serious), the lead authors added an explanation.
The panel drafted recommendations for each PICO question by working through the GRADE evidence-to-decision framework.Citation23 This framework considers the quality of evidence, balance of desirable and undesirable effects, patient values and preferences, resource use, health equity, acceptability of an intervention and feasibility of an implementation. Accordingly, the panel established consensus for each recommendation based on the above framework (either conditional/weak, or strong) and a rating of the overall quality of the body of evidence. The recommendations were then vetted by the CTS Canadian Respiratory Guidelines Committee (CRGC) Chair to optimize the language of each recommendation to enhance implementability.Citation24 The recommendation consensus process was completed by electronic survey using a 6-point voting scale, whereby it was defined a priori that a recommendation would only be accepted if each panel member voted for option 1, 2 or 3 (wholeheartedly agree, agree or can support).
For a recommendation to be accepted, it had to be voted on by 75% of the eligible panel members and achieve ratings of 1, 2 or 3 by 80% of the voting panelists. No panel member was excluded from voting. In the event of a failure to reach 80% of votes with ratings of 1, 2 or 3, another period of discussion ensued, whereby dissenting opinions were heard and considered. The recommendation was revised and followed by a second round of voting by electronic survey using a 3-point scale, for which acceptance of a recommendation required a 80% of panelists to choose option 1 (Agree) or 2 (Can Support). Throughout this process, all recommendations achieved acceptance, with no recommendation requiring a second round of voting.
Implications of strong and conditional recommendations Citation 25 , Citation 26
The implications of a strong recommendation are:
For patients—most people in your situation would want the recommended course of action and only a small proportion would not; request discussion if the intervention is not offered
For clinicians—most patients should receive the recommended course of action
For policy makers—the recommendation can be adopted as a policy in most situations
The implications of a weak/conditional recommendation are:
For patients—most people in your situation would want the recommended course of action, but many would not
For clinicians—you should recognize that different choices will be appropriate for different patients and that you must help each patient to arrive at a management decision consistent with her or his values and preferences
For policy makers—policy making will require substantial debate and involvement of many stakeholders
We included clinical remarks with PICO clinical questions and recommendations, in an effort to complement recommendations with practical clinical advice. Some of these remarks are not based on strong evidence, but represent the consensus opinions of panel members, based on their expertise.
Good practice points are included in association with each clinical question and are intended to offer additional clinical advice to help the target user apply recommendations to clinical practice. Some of these good practice points may not have an evidence base but are nevertheless viewed as good clinical practice by the expert panel. All good practice points were derived by consensus, based on the clinical experience of the guideline panel members.
Applicability/Implementability
Recommendations were formulated with the aim of being clear and actionable by clinicians within the user group, in accordance with best principles for guideline language and format.Citation24 Notwithstanding recent advances in knowledge with the publication of important RCTs on long-term NIV in patients with severe COPD and chronic hypercapnic respiratory failure, scientific evidence remains limited and recommendations are weak/conditional. The recommendations are accompanied by extensive comments through the various sections to help users, such as clinicians, policy makers and other stakeholders, understand the basis for the recommendations and apply them judiciously. These guidelines target a very specific patient population and a therapy requiring highly specialized expertise and resources. The Future Research Needs section describes limitations and gaps in the current literature with respect to applicability and implementation in the Canadian setting. Resource implications are also considered.
Review and approval process
In accordance with the CTS Guideline Production Methodology, before completion, the CTS independently invited formal review of the guideline by 1) 2 external (non-CTS) international and 2 internal (CTS) reviewers. One of the internal reviewers performed an AGREE assessment of the CPG. The authors were blinded to the identities of the reviewers. Each expert provided a detailed review and suggestions, and authors responded to these reviews in detail. These reviews were provided to the CTS CRGC for review. Members of the CRGC then completed a review of the CPG and these documents and provided further feedback for consideration by authors. Upon acceptance, the CRGC recommended approval of the CPG to the CTS Executive Committee. All reviews and author responses are posted on the CTS website.
Living guideline/future updates
This CPG will be formally reviewed every 3 years or sooner to determine the need for and nature of any updates, in accordance with the CTS Living Guideline Model. The CTS HMV Clinical Assembly Steering Committee members will also use the continuously updated McMaster Plus database, whereby they will receive alerts when new articles pertaining to these PICO questions are published (starting from the last date of the literature search conducted for this CPG). This will serve to prompt members to consider timely CPG updates with evolving evidence and will facilitate formal literature reviews.
SUMMARY OF RECOMMENDATIONS FOR THE USE OF LONG-TERM NON-INVASIVE VENTILATION IN PATIENTS WITH SEVERE COPD AND HYPERCAPNIC RESPIRATORY FAILURE
Results
Section 1: Assessment of benefit of long-term NIV in patients with COPD and chronic hypercapnic respiratory failure
In this section, outcome prioritization by the panel resulted in ranking dyspnea, HRQoL, PaCO2, hospitalization and survival as most relevant and as having sufficient supporting literature. Two distinct clinical situations are the subject of this updated review of the literature: i) patients with COPD and chronic hypercapnic respiratory failure who are otherwise stable (PICO 1a) and ii) patients with COPD and chronic hypercapnic respiratory failure who are recovering from a recent hospitalization for acute-on-chronic hypercapnic respiratory failure (PICO 1 b).
Clinical remarks
Success (impact on outcomes) of long-term NIV depends on appropriate patient selection and the center’s experience.
Initiation of long-term NIV in patients with COPD and chronic hypercapnic respiratory failure should follow a rigorous and standardized protocol aiming at sustained reduction in daytime PaCO2 and/or nighttime transcutaneous CO2 (ptCO2).
Close follow-up and optimization of ventilator settings is required to ensure efficacy and continued treatment adherence. The panel recommends a target of a minimum of 5 hours/day of NIV use.
The decision to initiate and maintain long-term NIV should take into account patient preference, given the potential burden to the patient and implications with respect to health care resource utilization.
Review of evidence by outcomes
1. Dyspnea
We identified 8 RCTs that evaluated change in dyspnea in patients with severe COPD and chronic hypercapnia who were treated with usual care alone or with long-term NIV.Citation3,Citation4,Citation27–32 This outcome was measured with the Medical Research Council (MRC) and modified MRC (mMRC) scales, Transitional Dyspnea Index (TDI), Chronic Respiratory Questionnaire (CRQ) dyspnea subscale, dyspnea scale of Mahler and Borg scale. Results tended to be inconsistent among studies, as well as within studies, depending on the time point of data collection and type of outcome measure used to quantify dyspnea. Nevertheless, 4 of the 8 studies found improvement in dyspnea in at least 1 scale and at least at 1 or more time points.Citation3,Citation4,Citation27,28 Various ventilation strategies and levels of inspiratory positive airway pressure (IPAP) were used but this did not appear to influence dyspnea relief. For example, studies using relatively low IPAP found improved MRC,Citation3,Citation4 as did one with higher mean IPAP levels.Citation28 Conversely, Márquez-Martín et al. found no significant improvement in mMRC with nocturnal NIV in addition to exercise training,Citation30 with IPAP titrated up to 20 cmH2O. Zhou et al., in the largest RCT assessing dyspnea, also found no significant benefit on this outcome, as measured by TDI, with long-term NIV using maximal tolerated IPAP (mean of 17.8 cmH2O).Citation32 Hence, although there is some indication that nocturnal long-term NIV can alleviate dyspnea, results are inconsistent across studies. Studies were generally of limited sample size, used various measures with heterogeneous results, and were inherently prone to bias, as dyspnea is a subjective outcome and patients were not blinded to treatment (in most cases). Therefore, the quality of evidence was determined to be very low.
2. HRQoL
This outcome was measured in 10 studiesCitation4–6,Citation16,Citation27–30,Citation32,Citation33 using the CRQ, St. George’s Respiratory Questionnaire (SGRQ), Maugeri Foundation Respiratory Failure Questionnaire (MRF-28), Short Form Health Survey (SF-36), COPD Assessment Test (CAT) or Severe Respiratory Insufficiency (SRI) Questionnaire. Improvement in HRQoL with long-term NIV compared to control was found in 6 studies for at least 1 measuring tool including SGRQ,Citation5,Citation16,Citation33 MRF-28,Citation4,Citation28 and CRQ.Citation29 With the exception of Garrod et al.,Citation29 participants in these studies were hypercapnic at baseline. Kohnlein et al.,Citation5 who used high-intensity NIV, had the largest number of participants and a follow-up of 1 year, found an improvement in SGRQ and SRI, but no significant difference in SF-36 with long-term NIV compared to control. Three studies found no significant difference in HRQoL measures with follow-ups ranging from 12 weeks to 6 months.Citation27,Citation30,Citation32 Bhatt et al. randomized 30 patients with PaCO2 <52mmHg and used standard NIV settings (15/5 cmH2O) for 6 months. They found no significant benefit of long-term NIV on the CRQ, except the Mastery domain, which was correlated with average nightly duration of NIV use.Citation27 Zhou et al. used maximal tolerated IPAP (mean of 17.8 cmH2O) in a 3-month study of 115 hypercapnic patients.Citation32 There was a non-significant improvement in CAT with long-term NIV with no between-treatment differences in SRI scores. A shorter study where nocturnal NIV was added to a rehabilitation program found no additional benefit of NIV on CRQ despite improvement in PaCO2.Citation30 McEvoy et al. enrolled 144 participants who were followed for 1 year and found deterioration in subscales of the SF-36, and no significant change in SGRQ,Citation6 using modest NIV pressures. Overall, results are inconsistent and may depend on the outcome measuring tool used, as well as patient characteristics (eg, less benefit in non-hypercapnic patients), NIV parameters and center’s experience with long-term NIV. Data quality was rated very low because of lack of blinding and inconsistency and imprecision from limited sample sizes in most studies.
3. Daytime PaCO2
Blood gases were assessed in 13 studiesCitation3–6,Citation16,Citation27–34 and PaCO2 was found to be improved in 5.Citation5,Citation16,Citation28,Citation30,Citation32 In 4 of those studies, the mean IPAP level was at least 17.8 cmH2O, and 1 study did not provide the final mean IPAP (though it was titrated up to 20 cmH2O, as tolerated).Citation30 The studies without improvement in PaCO2 generally used lower pressures and/or included non-hypercapnic patients.Citation3,Citation27,Citation31 These data suggest that PaCO2 can be reduced in patients with COPD and chronic hypercapnia using long-term NIV with sufficient inspiratory pressures. Although there does not appear to be a clear relationship between PaCO2 reduction and improvement in dyspnea or quality of life, immediate and sustained reduction in PaCO2 is an important therapeutic objective because it is a marker of the clinical response to long-term NIV,Citation5,Citation35 although not in all studies.Citation6 Data quality was considered moderate because PaCO2 is an objective measurement and blinding was not considered as critical for this outcome, but there was inconsistency between studies.
4. Hospitalization
This outcome was measured in 5 studiesCitation3–6,Citation28 and none found a benefit of NIV. Casanova et al. included participants with or without hypercapnia and followed them for 1 year. This study had a modest sample size and used low IPAP settings.Citation3 Clini et al. included hypercapnic patients and also used low IPAP settings. They found a non-significant reduction in hospital and ICU admissions over a 2-year period.Citation4 Similarly, McEvoy et al. used low IPAP pressures in their mildly hypercapnic group and found no significant difference in hospitalizations over 1 year.Citation6 Duiverman et al. compared NIV added to a rehabilitation program vs. the program alone and found no difference in rate of exacerbations or hospitalizations.Citation28 Mean IPAP was fairly high but baseline hypercapnia relatively mild. Kohnlein et al. reported that long-term NIV did not significantly reduce unplanned hospital admissions compared to usual care.Citation5 Hence, in stable patients with COPD with or without hypercapnia, there was no evidence that hospitalizations can be significantly reduced with long-term NIV compared to controls. Potential sources of bias include: heterogeneity in patient characteristics and NIV strategies, no descriptions of decision-making or criteria for hospitalizations. Finally, hospitalizations were not the primary outcome in any of the studies. Importantly none of these studies was adequately powered to detect between-treatment group changes in hospitalization, creating marked imprecision. Therefore, the quality of evidence for this outcome was rated as very low.
5. Survival
There were 4 studies that evaluated the effect of long-term NIV on survival in patients with stable COPD. Casanova et al. (12-month follow-up) and Clini et al. (2-year follow-up) found no significant effect on survival.Citation3,Citation4 Both studies used modest IPAP pressures and, were not powered adequately to detect a difference in survival. Hypercapnia was not an inclusion criterion in the Casanova study. Conversely, McEvoy et al. (median follow-up of 28.5 months) used a larger sample and found improved survival with NIV despite using relatively low IPAP pressures and reporting negative impact of long-term NIV on HRQoL.Citation6 Kohnlein et al. had the largest sample size and used high IPAP pressures.Citation5 They found a marked survival benefit in those using NIV over a 12-month period. Participants in the Clini, McEvoy et al. and Kohnlein et al. studies were hypercapnic, with the highest mean PaCO2 in Kohnlein et al.Citation4–6 Established long-term oxygen therapy (LTOT) was also an inclusion criterion in the Clini and McEvoy et al. studies but not Kohnlein et al.Citation4–6 The data were found to be inconsistent and imprecise, and the overall quality of data was deemed low. However, mortality is an outcome with little potential for bias. Recommendations considered that in the 2 negative studies, statistical power was inadequate for this outcome and these studies were attributed lower value. Conversely, mortality was the primary outcome in the positive studies, thus giving them greater weight.
Expert panel discussion of additional considerations and clinical judgment of risk versus benefit
The panel discussed the threshold PaCO2 that should be used for selecting COPD candidates for long-term NIV. The literature does not provide a clear cut-off below which NIV is ineffective. However, the study showing the greatest benefit of NIV in stable hypercapnic patients included patients with PaCO2 at least 51.9 mmHg and a mean that was much higher, at 58.5 mmHg.Citation5 Moreover, the literature suggests that clinical benefit of NIV is associated with PaCO2 reduction and that patients with higher baseline PaCO2 are most likely to benefit.Citation35 Survival benefit was also noted in the McEvoy et al. study where patients were eligible with a seemingly lower PaCO2 (>46 mmHg), but the actual mean PaCO2 in this study was 53.5 mmHg.Citation6 Hence, the opinion of the panel is that data support long-term NIV only for those chronically hypercapnic patients with COPD with PaCO2 levels ≥ 52 mmHg. Lower levels of hypercapnia may result in ventilating patients who would not benefit from this therapy, causing unnecessary burden to patients and resources utilization. Other expert panels have suggested different thresholds, underlining the inconclusiveness of the literature in this regard.Citation36,Citation37
The panel members generally agreed that NIV should be aimed at reducing PaCO2. The literature suggests PaCO2 reduction is a marker of effectiveness of the treatment. The Kohnlein et al. study targeted PaCO2 reduction by 20% or more, or a value < 48.1 mmHg.Citation5 However, not all studies showing clinical benefit reported improvement in PaCO2.Citation6 Nocturnal ptCO2 has also been used as a marker of NIV effectiveness.Citation7,Citation38 However, safety and tolerability of the NIV parameters must be prioritized. Hence, the panel recommends targeting substantial PaCO2 reduction, but specific targets cannot be recommended at this time.
The panel also discussed the necessity for a minimal daily adherence for benefit of NIV. The mean daily use of NIV in the Kohnlein et al. study was 5.9 hours, and in the McEvoy et al. study it was 4.5 hours.Citation5,Citation6 Prior literature also suggests that patients using NIV more than 5 hours per night derived greater benefit than those using it less than 5 hours.Citation35 Based on the available data, the consensus-based recommended a duration of use per 24-hour period of at least 5 hours. Of note, others have made a similar recommendation.Citation36 Although in the Kohnlein et al. study participants were allowed to use NIV in the daytime, to what degree this was done by participants is not reported.Citation5 Moreover, other trials have not used this strategy. Finally, based on the physiology of breathing in sleep and expected sleep-related hypoventilation in patients with severe COPD and chronic hypercapnia, it is expected that nocturnal NIV would provide the most benefit. No specific recommendation can be made at this time regarding the benefit of daytime use of NIV given insufficient data.
Patient values and preferences
For this recommendation, we placed high value on NIV’s beneficial impact on mortality and HRQoL. We placed low value on NIV’s impact on cost (including resources and expertise required for initiation and titration of NIV), burden of utilization of NIV therapy and adverse effects, although the latter may impact HRQoL, one of the outcomes reviewed.
Details of included studies
summarizes the design and outcomes of the RCTs evaluating NIV in patients with stable severe COPD. summarizes key patient selection criteria and NIV settings. Two studies were designed with survival as the primary outcome and are described in more detail.Citation5,Citation6
Table 1. Results for outcomes in studies of long-term NIV in patients with stable severe COPD.
Table 2. Inclusion criteria and NIV parameters in studies of long-term NIV in patients with stable severe COPD.
The McEvoy et al. study recruited 144 individuals with stable severe COPD, who were on LTOT and had a PaCO2 > 46 mmHg on at least 2 occasions (mean 53.5 mmHg).Citation6 Polysomnography was used to exclude those with more than mild sleep apnea. Participants were randomized to NIV with LTOT or LTOT alone. NIV was initiated during a hospital admission over 3-4 days. Expiratory positive airway pressure (EPAP) was initially set at 3 cmH2O while IPAP was titrated during daytime and nighttime periods, aiming at a level of at least 10 cmH2O above EPAP, to a maximum tolerated. Another polysomnography was then performed to titrate EPAP to abolish snoring and hypopneas/apneas. Mean IPAP was 12.9 cmH2O and mean EPAP was 5.1 cmH2O. Participants were followed for a median 28.5 months in the NIV group. Mean adherence to NIV was 4.5 hours per night. NIV led to improved survival with a borderline significant hazard ratio of 0.63 (95% CI 0.40 to 0.99; p = 0.045, adjusted). No significant between-treatment difference in PaCO2 was detected at follow-up. NIV also failed to normalize sleep architecture. HRQoL as measured by SGRQ was not significantly changed but there was deterioration in several subscales of the SF-36 (poorer general and mental health) and profile of mood states (POMS) (less vigor and more confusion and bewilderment). Hence, the small survival benefit appears to have been at the expense of reduced HRQoL. The relatively low IPAP and suboptimal NIV use, with no reduction in PaCO2, provide potential explanations for these findings.
In the Kohnlein et al. study, 195 participants with stable GOLD stage 4 COPD and PaCO2 > 51.9 mmHg (mean 58.5 mmHg) were randomized to NIV or usual care.Citation5 NIV was initiated during a hospital admission and targeted to reduce baseline PaCO2 by ≥ 20% or to a PaCO2 < 48.1 mmHg. Mean IPAP was 21.6 cmH2O and EPAP 4.8 cmH2O, and back-up rate 16 per minute (69% of patients had back-up rates > 14 per minute). Regular follow-up visits were scheduled at 14 days, and 3, 6, 9, and 12 months after randomization, where patients from both groups were admitted to hospital for optimization of care. Additionally, all patients were contacted by telephone every 4 weeks. Participants were instructed to use NIV at least 6 hours per day, preferably at night but daytime use was accepted. Mean ventilator use was 5.9 hours per day. For the primary outcome of 1-year all-cause mortality, the hazard ratio was 0.24 (95% CI 0.11–0.49; p = 0.0004). Unplanned hospital admissions were rare. PaCO2 and FEV1 improved significantly in the NIV group compared to usual care. HRQoL was measured using SF-36, SGRQ and SRI. Only the SF-36 general health perception subscale, SGRQ total score, and SRI total score were significantly improved with NIV compared to usual care. Hence, this study suggests that NIV targeted at reducing PaCO2 in patients with stable severe COPD may reduce mortality markedly over 1 year. However, the intense follow-up protocol with regular hospital admissions and telephone calls may not be feasible in all jurisdictions outside of a trial.
Good practice points for PICO 1a
The required level of baseline hypercapnia in patients with stable COPD in order to benefit from NIV is not clear. In the McEvoy et al. study, the mean PaCO2 in recruited individuals was 53.5 mmHg.Citation6 In the Kohnlein et al. study, the mean PaCO2 was 58.5 mmHg.Citation5 It appears likely that greater benefit occurs in patients with higher levels of baseline hypercapnia. Hence, the panel recommendation to use 52 mmHg or higher as a cut-off is based on available data and consensus opinion.
The decision to initiate NIV in patients with stable severe COPD should take into consideration patient burden and preference. In the McEvoy et al. study, HRQoL was negatively affected in some domains in the NIV group.Citation6 Other studies have shown improvement or no change in HRQoL. Whether this depends on ventilator settingsCitation39 or other factors is unclear.
Clinical remarks
Appropriate patient selection is a key element of success of long-term NIV (impact on outcomes). Persistent hypercapnia should be documented 2-4 weeks after the acute hypercapnic exacerbation to avoid initiating long-term NIV in patients with transient hypercapnia that resolves with recovery from the exacerbation.
The panel recommends that only patients with persistent daytime PaCO2> 52 mmHg be considered for long-term NIV.
To achieve similar results as in the Murphy et al. trial, similar ventilatory objectives are required. The aim should be to reduce PaCO2 or ptCO2 by “achieving control of nocturnal hypoventilation with a high pressure ventilation strategy and a high back-up rate [14-16 breaths/minute])” (see details in the Review of Evidence by Outcomes section).
Close follow-up and optimization of ventilator settings is required to ensure efficacy and continued treatment adherence. The panel recommends a target of a minimum of 5 hours/day of NIV use.
Review of evidence by outcomes
We identified and assessed 4 studies of long-term NIV in patients with COPD recovering from a hospitalization for acute hypercapnic exacerbation requiring acute NIV treatment that addressed at least one of the outcomes of interest.Citation7,Citation8,Citation40,Citation41
1. Dyspnea
Of the 4 studies of long-term NIV in patients with COPD and chronic hypercapnia who were recovering from a hospitalization for acute hypercapnic exacerbation, dyspnea was only reported by Struik et al.Citation41 They assessed dyspnea using the MRC scale and found no significant difference between long-term NIV and usual care. Another study indicated having measured MRC but we could not find the results.Citation7 Due to the possibility of bias in reporting dyspnea in an unblinded study and very serious imprecision from the limited number of patients assessed, we deemed the quality of the data to be very low for this outcome.
2. HRQoL
We found 2 studies evaluating the effect of long-term NIV on HRQoL in patients with COPD and chronic hypercapnia recovering from a hospitalization for acute hypercapnic exacerbation.Citation7,41 Struik et al. found no significant improvement in the Clinical COPD Questionnaire (CCQ), MRF-28, CRQ or SRI, although there was a trend for improvement in the SRI score.Citation41 Murphy et al. found no significant improvement in SRI, but did find a significant improvement in SGRQ in the NIV group compared to the usual care group at 3 months (but not on subsequent assessments).Citation7 Results may have been impacted by numerous cross-overs from the usual care to the active treatment group (n = 18 of 59 randomized into control group) and insufficient statistical power. Hence, it is unclear if NIV in this context improves HRQoL. The quality of the evidence was affected by inconsistency and imprecision and was determined to be very low.
3. Daytime PaCO2
We identified 4 studies evaluating change in PaCO2 with NIV compared to a control intervention in patients with COPD studied after hospitalization for acute hypercapnic exacerbation.Citation7,Citation8,Citation40,Citation41 In 3 studies, patients who remained hypercapnic after recovery from the index hospitalization were randomized to long-term NIV or usual care alone.Citation7,Citation40,Citation41 One study used continuous positive airway pressure (CPAP) as the control intervention.Citation8 De Backer et al. found significantly improved PaCO2 in the long-term NIV group only, but no between-treatment comparisons were made.Citation40 Cheung et al. found no between-treatment difference in PaCO2 between long-term NIV and CPAP groups after up to 12 months follow-up.Citation8 Struik et al. also found no significant difference when values were measured in similar conditions between baseline and follow-up.Citation41 In both the Cheung et al. and the Struik et al. studies, participants were randomized early, hours following recovery from the acute hypercapnic exacerbation episode.Citation8,Citation41 In those studies, PaCO2 improved similarly in both the long-term NIV and the usual care groups. In Murphy et al., participants were randomized 2 to 4 weeks after the end of the acute event. In that study, the reduction of PaCO2 was larger in the long-term NIV group than in the usual care group at 3 months, but effect was not sustained at 6 or 12 months.Citation7 Results may have been impacted by cross-over of usual care participants into the active treatment group. Murphy et al. measured overnight transcutaneous PaCO2 in a subset of participants.Citation7 Values were significantly reduced in the NIV group compared with the usual care group at 12 months. In summary, it remains unclear if NIV can significantly impact PaCO2 in patients remaining hypercapnic after an acute hypercapnic episode. Because imprecision and inconsistency in the data were significant, the quality of the data was considered low. It seems plausible that waiting at least 2 weeks after the acute event to assess PaCO2 may identify those patients with truly “persistent” hypercapnia which might be correctable with long-term NIV.
4. Hospitalization
This outcome or a composite outcome including hospital readmission was assessed in 3 trials that studied patients started on long-term NIV after an episode of hypercapnic respiratory failure and acute NIV.Citation7,Citation8,Citation41 Cheung et al. randomized participants to NIV (mean IPAP 14.8 cmH2O) or CPAP, 48 hours after weaning off acute NIV.Citation8 They found no between-treatment difference in the composite outcomes of occurrence of acute respiratory failure requiring NIV or intubation or death over the 12 months follow-up. Struik et al. also randomized participants to long-term NIV or usual care as early as 2 days after the recovery from an acute hypercapnic exacerbation (mean IPAP 19 cmH2O) and found no significant improvement in time to hospital readmission over 12 months with long-term NIV.Citation41 Murphy et al. randomized participants to long-term NIV (mean IPAP 24 cmH2O) or usual care 2 to 4 weeks after the acute event.Citation7 The primary outcome in that study was a composite of readmission or death, whose occurrence was significantly reduced in the NIV group compared to usual care. In this study, most events included in the composite outcome were hospitalizations. Moreover, a post-hoc analysis looking specifically at hospital readmissions also found a significant reduction in the long-term NIV group. In the Murphy et al. study, all patients were on LTOT (inclusion criterion), while approximately 15% of participants in Cheung et al. and 70% of completers in Struik et al. were on LTOT. In all studies, bias was a potential issue as the criteria for hospitalization was not specified and blinding of treatment was not possible (except possibly in the Cheung et al. study). There was inconsistency in results between studies which may be attributable to the timing of initiation of NIV after the acute event, participant differences, or ventilator settings. Imprecision was also present due to the relatively limited sample sizes of studies. Overall, the quality of data was deemed very low for this outcome. However, the positive results and specific methodology of the Murphy et al. trial were deemed important and motivated the recommendation despite negative results in Cheung et al. and Struik et al.
5. Survival
Three studies assessed survival, and found no significant difference between long-term NIV and usual care intervention after 1 year of follow-up.Citation7,Citation8,Citation41 Survival was not the primary outcome in any of the 3 studies identified, which were underpowered to detect a difference in this outcome. Murphy et al. found an adjusted hazard ratio of 0.67 in favor of NIV, but this was not statistically significant. Many participants in that study crossed-over early in the study from the usual care to the long-term NIV group after hospital readmission, and this likely affected the 12-month survival outcome. In the Struik et al. study, almost half of randomized individuals dropped out of the study.Citation41 This high drop-out rate likely decreased statistical power to detect a difference in mortality. Moreover, this points to the difficulty in maintaining long-term NIV in patients with severe COPD. We found no studies evaluating effect of long-term NIV on survival as the primary outcome in patients with severe COPD post-acute hypercapnic exacerbation. Imprecision was a major concern with respect to this outcome and data quality was determined to be low.
Expert panel discussion of additional considerations and clinical judgment of risk versus benefit
The panel determined that the same threshold PaCO2 value of ≥ 52 mmHg should be used for the target population for PICO 1 b as for PICO 1a, for clarity, consistency, and to facilitate implementation. The Murphy et al. trial, evaluating patients’ post-acute hypercapnic exacerbation, included participants with mean baseline PaCO2 of 59 mmHg, measured 2-4 weeks after the acute event.Citation7 Though the baseline PaCO2 was similar in the Struik et al. trial,Citation41 participants to this study had PaCO2 measurements immediately after the acute event, and there was a progressive spontaneous improvement in PaCO2 in both the control and NIV groups over the course of the trial. The negative results of the Struik et al.Citation41 trial suggest that patients without marked, truly chronic hypercapnia are unlikely to benefit from long-term NIV.
The panel discussion emphasized the need for sustained adherence to NIV to derive benefit from this therapy. For consistency with PICO 1a, the panel recommends the same adherence target minimum duration of utilization of 5 hours per day.
Patient values and preferences
For this recommendation, we placed high value on NIV’s beneficial impact on delaying hospital readmission. We placed low value on NIV’s impact on cost (including resources and expertise required for initiation and titration of NIV), burden of utilization of NIV therapy and adverse effects, although the latter may impact HRQoL, one of the outcomes reviewed.
Details of included studies
summarizes the design and outcomes of the 4 studies on home NIV in patients with COPD following a severe hypercapnic exacerbation. summarizes key patient selection criteria and NIV settings.
Table 3. Results for outcomes in studies of long-term NIV in patients with COPD post-acute severe hypercapnic exacerbation.
Table 4. Inclusion criteria and NIV parameters in studies of long-term NIV in patients with COPD post-acute severe hypercapnic exacerbation.
One of the largest trials was done by Struik et al.,Citation41 which randomized 201 participants with persisting hypercapnia at least 48 hours after termination of acute ventilatory support to long-term NIV or usual care. Long-term NIV was initiated in the hospital with the aim of maximally supporting respiration and achieving normocapnia. A standard spontaneous/timed pressure support mode was used, starting with IPAP of 14 cmH2O and gradually increasing to a maximal tolerated level. EPAP was increased if auto-positive end-expiratory pressure (PEEP) was detected or when “respiratory muscles were used to trigger the ventilator”. Polysomnography was not used for titration, but overnight capnography was used to confirm efficacy of NIV. Mean + SD settings were IPAP 19.2 ± 3.4 and EPAP 4.8 ± 1.0 cmH2O, respectively, and respiratory rate 15 ± 3 breaths/min. Mean baseline PaCO2 was 58.5 mmHg and FEV1 averaged 26% of predicted. The primary outcome was time to event for the composite outcome of hospital readmission for respiratory cause or death. The drop-out rate was high and similar in both groups with only 108 of the 201 subjects completing the protocol. An intention to treat analysis at 12 months follow-up revealed no between-treatment difference in this outcome or any of the secondary outcomes of survival, number of respiratory hospital readmissions, COPD exacerbations, lung function, HRQoL, mood state, daily activity levels or dyspnea. Notably, hospital readmission rates were lower than expected, at around 57% overall. Moreover, PaCO2 improved after the initial hospitalization in both study groups, with near-normalization at the 3-month follow-up. This raises the possibility that participants in this study may not have been the target group most likely to benefit from long-term NIV because many did not exhibit chronic hypercapnia when in stable condition.
The second largest and most recent trial in post-acute hypercapnic exacerbation patients, the HOT-HMV study,Citation7 opted for a slightly more delayed recruitment after recovery from the acute hypercapnic episode. In this study, 116 participants were randomized 2 to 4 weeks after the acute event to NIV + LTOT or LTOT alone. Participants had a mean baseline PaCO2 of 59 mmHg, FEV1 of 23% of predicted, and all met standard criteria for LTOT. Hence, participants represented a group with more severe COPD than in the Struik et al. study,Citation41 which is also supported by the higher rates of COPD exacerbations and hospital readmissions. The primary outcome was a composite of time to hospital readmission or death within 12 months after randomization. Long-term NIV resulted in a hazard ratio for this composite outcome of 0.49 (95% CI, 0.31-0.77; P 0 = 0.002, adjusted) compared to usual care. There was also a significant delay in time to hospital readmission (median 4.3 months vs. 1.4 months). The primary outcome was met in 50% of participants at 1 month. This study emphasizes the importance of timing and suggests that assessment for home NIV within 2 to 4 weeks of the acute event is likely advisable. COPD exacerbation rate was significantly reduced from a median of 5.1 exacerbations per year in the usual care group to 3.8 exacerbations per year in the long-term NIV group. Mortality was not significantly reduced in the long-term NIV group. It should be noted that 18 of the 59 participants randomized to the usual care group received long-term NIV, most following hospital readmission. This cross-over rate may have prevented detection of a mortality difference over the course of the 12-month follow-up. This may also explain the significant differences in some HRQoL measures and PaCO2 between treatments at 3 months, but not in subsequent assessments. Long-term NIV was initiated during a daytime acclimatization trial, and then titrated under overnight polysomnography with capnography. Initial settings were IPAP 18 cmH2O and EPAP 4 cmH2O. The aim was to reach a target IPAP of ≥ 25 cmH2O. Sleep studies were repeated on consecutive nights if further titration was needed to achieve control of hypoventilation and optimize tolerance. Final median IPAP was 24 cmH2O, EPAP 4 cmH2O and backup rate 14 breaths/min. Median NIV use was 4.7 hours per night at 6 weeks, and increased to 7.6 hours per night at 12 months, but this is based on data from 26 participants only (of 36 evaluated at 12 months). This study demonstrated that in a selected group of patients with severe COPD, using a very specific protocol, NIV may delay re-hospitalization and reduce exacerbation rate.
Good practice points for PICO 1b
Participants in the Murphy et al. trial had PaO2 < 55 mmHg or < 60 mmHg with additional severity characteristics such as cor pulmonale or pulmonary hypertension. In the absence of those features, there are no data to support long-term NIV use to reduce re-hospitalization in patients remaining hypercapnic after an episode of acute respiratory failure. Study population differences likely accounted for the diverging results between the Murphy et al.Citation7 and Struik et al.Citation41 studies.
Future research needs for PICO 1a and PICO 1b
Although we have divided our assessment into patients with COPD who were stable, on the one hand, and those post recent acute hypercapnic exacerbation, on the other hand, some heterogeneity remains within those groups, including baseline PaCO2 levels in the former and timing of NIV initiation in the latter. This leads to unresolved questions regarding the target population most likely to benefit from long-term NIV. Marked survival benefit of NIV occurred in one study that included stable patients with a PaCO2 at least 51.9 mmHg, and significant reductions in PaCO2 at follow-up.Citation5 In another study also reporting a survival benefit of long-term NIV, average PaCO2 levels were 52-54 mmHg.Citation6 Hence, our proposal for a cut-off of PaCO2 of ≥ 52 mmHg below which we do not suggest long-term NIV. Further research is nevertheless needed to clarify which patients with stable COPD are likely to benefit most from long-term NIV. The presence of COPD disease severity markers such as chronic hypoxemia, cor pulmonale and pulmonary hypertension are likely important determinants of the clinical response to long-term NIV, as the trial showing benefit on re-hospitalizations included only patients requiring LTOT. The other trials where this criterion was not applied did not demonstrate benefit of NIV on re-hospitalizations. Another potential risk factor for hospital readmission that could inform patient selection may include persistent use of accessory muscles in sleep.Citation42 This would require a better understanding of the physiology of sleep-disordered breathing in COPD, as well as an assessment of the benefit of applying NIV using this targeting strategy. Timing of initiation of NIV is another element that differed among studies. Early initiation (from 48 h after recovery from an acute hypercapnic exacerbation) did not result in benefit of long-term NIV, possibly due to improvement in PaCO2 irrespective of group and, thus, to the initiation of long-term NIV in patients with COPD who do not exhibit chronic hypercapnia once fully recovered.Citation8,Citation41 Conversely, the trial that randomized patients with persistent hypercapnia 2-4 weeks after exacerbation and cessation of NIV in the acute setting, showed benefits of NIV compared to control,Citation7 supporting the notion that this timeframe is necessary to evaluate hypercapnia and long-term NIV eligibility. Further delays seem unwarranted as many participants were re-hospitalized within 1 month of randomization in that study. Hence, further work will need to be done to confirm and define optimal patient selection criteria for home NIV.
The studies that found a benefit of long-term NIV on hospitalization or survival excluded most obese individuals (BMI > 35 kg/m2 (Citation5,Citation7) or > 40 kg/m2 (Citation6)). Hence, results cannot be extrapolated to individuals with more severe obesity. Such individuals are more likely to have obstructive sleep apnea, and hence, might benefit from CPAP. However, whether CPAP or NIV should be considered in obese patients with COPD and hypercapnia is unknown, though NIV has been shown to be beneficial in this population.Citation43 Benefit of NIV may depend on predominant pathophysiology of hypoventilation, (i.e. upper airway versus lower airway obstruction), and this topic will require further study. In North America, including Canada, obesity rates are higher than in the majority of European countries where the most recent trials were conducted. In Canada, applicability of these CPGs may be restricted to a small subset of patients with severe COPD.
There is no data to inform on the efficacy of long-term NIV in patients who continue to smoke. Current smoking was not an explicit exclusion criterion in recent clinical trials of long-term NIV in COPD.Citation5,Citation7 In a recent study where this was discussed, 12% of the study population was actively smoking.Citation38 The potential implications of current smoking should nevertheless be discussed since many COPD candidates for long-term NIV are also receiving LTOT which is associated with increased risks of fire hazard, burns, and even death.Citation44–46 Considering that continued smoking is associated with poor outcomes in COPD, including repeated exacerbations and hospitalizations, the efficacy and safety (particularly when used with concomitant LTOT) of long-term NIV in this specific population should be addressed.
Health care costs of COPD are high and increasing but to which extent long-term NIV, if adopted to treat chronic hypercapnic respiratory failure in COPD, will impact this is not known.Citation47 Cost-effectiveness of long-term NIV in COPD requires further study. Unpublished analyses based on the Murphy study of patients post-acute exacerbationCitation7 found home NIV to be cost-effective, using both UK- and US-based costs.Citation48,Citation49 Canadian data are not available. Moreover, cost-effectiveness of long-term home NIV in patients with stable severe COPD has not been established.
Further trials are required in the North American and particularly the Canadian setting. In addition, the methodology used for NIV initiation and follow-up in the European trials may not be feasible across Canada. NIV initiation, adaptation and titration typically occurred over several nights in specialized units or polysomnography laboratories. In Canada, specialized NIV units are either non-existent in many jurisdictions or there is very limited accessibility; and sleep laboratories in most provinces have lengthy wait times for polysomnography. Moreover, few centers have broad experience with long-term NIV in COPD, and extensive staff training might be required. This includes choice of interface, and initiation and optimization of device settings (see Section 2) for maximal benefit (PaCO2 reduction and tolerability/adherence).Citation5,Citation7,Citation50 Home initiation of NIV may be an interesting approach.Citation38 The best strategy for follow-up of patients with COPD on long-term NIV has not been determined. In one study, patients were routinely admitted for regularly scheduled reassessments and had monthly calls during the course of the trial.Citation5 This close monitoring with optimization of medical management and other aspects of COPD care may have contributed to the success of NIV and positive outcomes.Citation51 However, such intense follow-up may not be feasible outside of a clinical trial. Remote monitoring of patient and device data downloads may be useful but this remains to be determined.Citation52 Hence, evaluation of more streamlined initiation and follow-up methods will be necessary to improve access to long-term NIV within the health care resources constraints, while maintaining optimal efficacy.
Finally, adverse effects of NIV are poorly reported in trials. When reported, they appear to consist primarily of interface-related skin and nasal/sinus issues.Citation5,Citation27,Citation32 that are remediable with interface adjustments. However, the high drop-out rate in some trials suggests that this therapy constitutes a significant burden to participants.Citation41 In one trial, certain domains of HRQoL were adversely impacted, even though survival was improved with NIV.Citation6 Tolerability and adherence can be affected by device settings as higher driving pressures appear to be preferred by patients,Citation39 but in turn, raise concerns about adverse cardiac effects in patients with preexisting heart failure (see Section 2).Citation53,Citation54 Hence, greater attention to adverse effects and patient experience will be needed in future research to optimize long-term NIV in this population.
Section 2: Modes of long-term non-invasive ventilation and settings
In this section, outcome prioritization by the panel resulted in ranking dyspnea, HRQoL and PaCO2 as most relevant and as having sufficient supporting literature.
Clinical remarks
High-intensity ventilation has been introduced following the suspicion that the failure of early clinical trials to confirm efficacy of long-term NIV in COPD was mostly related to suboptimal ventilatory settings.Citation39,Citation55 This mode of ventilation is characterized by higher inspiratory pressures (typically above 20 cmH2O) with back-up respiratory rate slightly above the natural breathing frequency (typically 14-18 breaths/min) with the objective of reducing PaCO2.Citation39 This ventilation strategy has been compared to low-intensity ventilation (IPAP of 14-16 mmHg) in a few clinical trials in which superior efficacy of high-intensity ventilation to improve dyspnea, HRQoL and PaCO2 during spontaneous breathing has not been confirmed. However, high-intensity NIV reduces mortality in patients with stable COPD and chronic hypercapnic respiratory failureCitation5 and hospital readmission after the recovery from an acute hypercapnic exacerbation.Citation7 Therefore, we suggest using high-intensity NIV when considering long-term NIV in patients with COPD and chronic hypercapnic respiratory failure.
There is no clear definition of what can be considered as “high-intensity” ventilation. Most would agree on the importance of attempting to normalize PaCO2, or if not feasible, of at least reducing daytime PaCO2 below 48 mmHg5 and/or daytime or nighttime ptCO2 by at least 20%.Citation5,Citation38,Citation56 This objective toward normocapnia is typically achieved with the use of IPAP ranging between 20 to 25 cmH2O, EPAP of 4 to 5 cmH2O, and back-up respiratory rates of 14-16 breaths/min.Citation5,Citation38,Citation56 Excessive pressures and high back-up rates may affect tolerability of NIV, as well as cause potential adverse consequences. Initiation in a controlled setting (often in hospital) with monitoring is advised, notably to allow acclimatization and progressive adjustments of the ventilatory settings. It is uncertain which of reducing PaCO2 or reaching high inspiratory pressures and back-up respiratory rates should be the primary goal of treatment initiation. Most successful clinical trials enrolled patients if the PaCO2 reduction objective was met.Citation5,Citation38,Citation56 According to this reasoning, high inspiratory pressures and back-up respiratory rates should be viewed as requirements for reducing PaCO2 and not as primary objective of the therapy.
Review of evidence by outcomes
We retrieved 3 studies comparing the effects of high versus low-intensity NIV on the clinical outcomes of dyspnea, HRQoL and PaCO2.Citation39,Citation53,Citation54 All studies used a cross-over study design, applying both ventilatory strategies either for 30 minutesCitation54 or for 6 weeks.Citation39,Citation53
1. Dyspnea
Dyspnea was investigated in 2 studies.Citation39,Citation53 In one of them, Borg dyspnea score was measured at the end of the 30-minute support intervention.Citation54 The other study Borg dyspnea score was assessed at the end of a 6-min walking test, completed after each of the 6-week NIV treatment periods.Citation39 The first study failed to report between-treatment differences in Borg dyspnea score with high versus low-intensity NIV while Dreher and colleaguesCitation39 reported a larger reduction in Borg dyspnea score at the end of the 6-min walking test following high-intensity NIV. It is difficult to reach a firm conclusion about the impact of high versus low-intensity NIV from these 2 studies in which the duration of exposure to the intervention was markedly different (30 min versus 6 weeks) and the assessment of dyspnea was done in different settings. Other potential sources of bias with these studies included lack of blinding to the intervention. Overall, the quality of data was deemed low for this outcome.
2. HRQoL
There is a paucity of data informing the impact of ventilatory pressures on HRQoL. The 2 studies that were reviewed used a cross-over study design with 6-week intervention periods and assessed HRQoL using the SRICitation39,Citation53 and/or the CAT.Citation53 Significantly improved HRQoL was reported with both high and low-intensity NIV with no added benefit of high-pressure ventilation. Absence of blinding to the study intervention was a major risk for bias when assessing HRQoL. Overall, the quality of data was deemed low for this outcome.
3. Daytime PaCO2
We reviewed 3 studies in which the impact of high versus low-intensity NIV on PaCO2 was assessed either while on ventilation during the day,Citation54 while on ventilation at night,Citation39 or while breathing spontaneously at rest during the day.Citation39,Citation53 Nighttime ptCO2 was also monitored in 2 trials.Citation39,Citation53 While on NIV, either during the day or the night, high-intensity ventilation led to greater decreases in PaCO2 compared to low-intensity ventilation;Citation39,Citation53,Citation54 however, this effect was not carried over during spontaneous breathing making the inferences of this finding uncertain. The reduction of PtCO2 overnight was numerically larger with high-intensity ventilation in 1 trial.Citation53 Overall, the quality of data was deemed low for this outcome.
Expert panel discussion of additional considerations and clinical judgment of risk versus benefit
The issue of tolerance and safety of high-intensity ventilation was discussed by the panel. While recognizing that this form of ventilation may not be acceptable to a proportion of patients, the panel was somewhat reassured by a clinical trial reporting that the mean daily use of NIV was greater with high-intensity compared to low-intensity NIV.Citation39 The possibility of worsening hyperinflation with high ventilation pressures and fast respiratory rate was discussed. This theoretical concern does not appear to be a major clinical issue in clinical trials. In general, low EPAP are used, minimizing the risk of further increase in lung volumes while potentially counterbalancing increased work of breathing related to intrinsic PEEP, if present. Similarly, the backup respiratory rates averaging 14 to 18 breaths/min in most studies, should allow sufficient time to complete expiration. Lastly, long-term NIV may lead to improved small airway function, mitigating any potential detrimental effects of NIV on operating lung volumes.Citation57 However, the study by Adler et al. introduced the notion of “deventilation syndrome,” defined as significant dyspnea in the morning after NIV use, which was relieved by adjusting NIV parameters toward less intense ventilation.Citation58 This suggests that excessive intensity of NIV may occur and result in adverse effects, and should therefore be avoided. The notion of high-intensity NIV versus high-pressure NIV was also discussed. High-pressure NIV differs from high-intensity NIV by the use of lower back-up respiratory rates as this may facilitate tolerance to the therapy and avoid potential adverse effects on NIV such as worsening hyperinflation.Citation56 Although conflicting data exists regarding the utility of the high back-up rates,Citation56,Citation59 the panel felt that there was no convincing evidence to recommend the use of high-pressure NIV instead of high-intensity NIV. Further research is required in this area.
Patient values and preferences
For this recommendation, we placed high value on NIV’s beneficial impact on delaying hospital readmission and improving survival. Tolerance to high-intensity ventilation was also considered to be important for the widespread applicability of this treatment. Considering that high-intensity NIV was a prerequisite for success in recent clinical trials,Citation5,Citation7 less emphasis was placed on the impact of NIV on costs and burden of utilization of long-term NIV.
Details of included studies
High versus low-intensity NIV
Dreher et al.Citation39 compared the effects of high versus low-intensity NIV on physiological outcomes and HRQoL in 13 patients with stable COPD and chronic hypercapnic respiratory failure (PaCO2 > 45 mmHg) who were already on NIV and on LTOT. The aim of high-intensity ventilation was to maximally reduce PaCO2 and this was done following a careful, in-hospital titration procedure. On average, an IPAP of 28 cmH2O and an EPAP of 4.5 cmH2O were used at a mean breathing frequency of 17.5 breaths/min. In comparison, the corresponding ventilatory parameters during low-intensity ventilation were: IPAP = 15 cmH2O, EPAP = 4 cmH2O, and breathing frequency of 8.0 breaths/min. Each ventilation strategy was applied for 6 weeks and all patients received nocturnal oxygen. PaCO2 during nocturnal ventilation was the primary outcome. Other outcome measures included daytime PaCO2 at rest while breathing oxygen, Borg dyspnea score immediately after a 6-min walking test, and HRQoL using the SRI. Significantly improved nighttime PaCO2 while on ventilation was seen with high- compared to low-intensity NIV (mean difference of 9 mmHg) and this was related to larger tidal volume. In contrast, no between-treatment differences in daytime PaCO2, 6-min walking distance, and HRQoL were observed. However, Borg dyspnea score immediately after a 6-min walking test was significantly improved in the high- compared to low-intensity NIV. Interestingly, adherence was significantly higher with high-intensity NIV by a mean of 3.6 hours per night.
Lukacsovits et al.Citation54 compared the short-term effects of high versus low-intensity NIV on PaCO2, work of breathing, non-invasive determination of cardiac output, and Borg dyspnea score at rest while receiving ventilatory support in 15 patients with COPD and chronic hypercapnic respiratory failure (PaCO2 ≥ 50 mmHg). Low-intensity ventilation was delivered according to a local protocol aiming to reduce PaCO2 by > 10%, achieving a VT of 6- ml/kg while reducing transdiaphragmatic pressure during tidal breathing by 50% of baseline value. These objectives were achieved with a mean IPAP of 17.7 cmH2O and mean EPAP of 4 cmH2O. High-intensity NIV was aimed at achieving the maximally tolerated pressure, at least 50% greater than with low-intensity NIV. This resulted in a mean IPAP of 27.6 cmH2O and mean EPAP of 4 cmH2O, thereby obtaining clear differences in the mean IPAP between the 2 ventilatory strategies. Each ventilatory strategy was applied for 30 minutes. High-intensity NIV improved breathing pattern, reduced work of breathing and PaCO2 at the end of the ventilatory period compared to low-intensity NIV. However, no between-group differences in dyspnea were found. More air leakage and greater reductions in cardiac output were seen with high-pressure ventilation. This short-term physiological study did not allow any conclusion with regard to the superiority of 1 ventilatory strategy over the other but nevertheless, pointed out possible adverse effects of high-pressure NIV in patients with COPD.
Duiverman et al.Citation53 compared the effects of 6 weeks of high and low-intensity NIV on cardiac and pulmonary function in patients with COPD and chronic hypercapnic respiratory failure in a randomized, open-label, 2-treatment period crossover design. Fourteen patients with GOLD stage 3 or 4 COPD who had symptoms of chronic respiratory failure and either ≥ 2 severe acute exacerbations with acute hypercapnic respiratory failure (pH <7.35) and/or a daytime PaCO2 ≥ 50 mmHg and/or nocturnal PaCO2 ≥ 52 mmHg or a rise in PtCO2 ≥ 7.5 mmHg during the night were randomized in accordance with the German CPGs for Home Mechanical Ventilation in patients with stable COPD.Citation60 NIV was titrated in-hospital; high-intensity NIV aimed at establishing normocapnia or the lowest PaCO2 value possible, according to patient’s tolerance. A back-up breathing rate just above the spontaneous breathing frequency during sleep was used. This resulted in a mean IPAP of 23.6 cmH2O and EPAP of 4–6 cmH2O. Low-intensity NIV used an IPAP ≤ 14 cmH2O and breathing frequency of ≤ 12 breaths/min. The primary outcome was percent change in cardiac output at rest, during spontaneous breathing after 6 weeks of treatment. Other outcome measures included the assessment of HRQoL (SRI, CAT), daytime PaCO2, nt-proBNP, lung function, and 6-min walking distance. Six weeks of either high-intensity or low-intensity NIV did not affect cardiac output. This study was not powered for many of the outcomes but suggested a benefit over time of both high and low-intensity NIV on HRQoL and physiological parameters. There were no significant differences between the 2 strategies for daytime PaCO2, night PtCO2, FEV1, HRQoL, and 6-min walking test.
Clinical remarks
Standard pressure-preset NIV (often referred to as pressure support ventilation) is the most commonly used mode of ventilation to treat chronic hypercapnic respiratory failure in patients with COPD. There is currently no evidence to support that this practice should change and standard pressure-preset NIV should remain the first line mode of ventilation.
Volume-assured pressure-preset modes of ventilation increase vulnerability to unintentional mask leaks and may be ineffective when leaks are not adequately controlled.
Review of evidence by outcomes
1. Dyspnea
We were unable to identify any study that compared the effects of volume-assured pressure-preset NIV with standard pressure-preset NIV on dyspnea.
2. HRQoL
The efficacy of volume-assured versus standard pressure-preset NIV to improve HRQoL has been compared in 2 cross-over studies.Citation61,Citation62 Both studies involved a small sample size and did not report any added benefits of volume-assured pressure-preset NIV over standard pressure-preset ventilation on HRQoL. Overall, the quality of data was deemed low for this outcome.
3. Daytime PaCO2
Four studies comparing the efficacy of volume-assured pressure-preset NIV versus standard pressure-preset NIV to reduce PaCO2 were reviewed.Citation61–64 Ekkernkamp et al.Citation63 reported larger reductions in PtCO2 with intelligent volume-assured pressure support (iVAPS) but this finding is not universal.Citation61,62,64 Volume-assured pressure-preset NIV does not lead to further reduction in daytime PaCO2 during spontaneous breathing when compared to high-intensity pressure ventilation.Citation61–63 Overall, the quality of data was deemed low for this outcome.
Expert panel discussion of additional considerations and clinical judgment of risk versus benefit
The panel concluded that there remain several uncertainties regarding the best ventilatory settings to provide long-term NIV in patients with COPD. In the absence of convincing evidence in favor of volume-assured modes, the use of standard pressure-preset ventilation appears as the most clinically useful method considering the widespread availability of this mode of ventilation and extensive clinical experience with its use.
Patient values and preferences
For this recommendation, we placed high value on the outcomes of hospital readmission and improving survival and on the fact that these relevant outcomes were positively impacted in clinical trials that have used standard pressure-preset ventilation. Tolerance to high-intensity ventilation was also considered to be important for the widespread applicability of this treatment. Less emphasis was placed on the impact of NIV on and burden of utilization of NIV therapy.
Details of included studies
Volume-assured pressure-preset NIV versus standard pressure-preset NIV
Oscroft et al.Citation61 reported the results of a randomized crossover trial comparing volume-assured pressure-preset and standard pressure-preset NIV in 24 patients with COPD and chronic hypercapnic respiratory failure. The 2 interventions were delivered for 8 weeks. The primary outcome was daytime PaCO2 and mean nighttime SpO2. Secondary outcomes included lung function, exercise capacity, mean nocturnal PtCO2, and HRQoL with the SGRQ and SF-36. Both treatments resulted in similar primary and secondary outcomes. No significant between-treatment difference was found in daytime PaCO2 during spontaneous breathing. A similar conclusion was reached for PtCO2 at night. Volume-assured NIV did not produce further clinical benefits on lung function, exercise capacity, and HRQoL compared to standard pressure-preset NIV.
Ekkernkamp and colleaguesCitation63 compared effects of volume-assured NIV to high-intensity pressure-preset NIV on sleep quality in patients with COPD and chronic hypercapnia. Patients with COPD already receiving home mechanical ventilation to treat chronic hypercapnic respiratory failure were enrolled. Both ventilatory strategies were applied for 1 night in a cross-over design to assess the impact of therapy on sleep stages. Following this, volume-assured and high-intensity pressure-preset NIV were applied for 6 weeks in a cross-over design to assess the impact on sleep quality as assessed by a visual analogue scale. No significant difference in the primary outcome of sleep quality was found between the 2 ventilatory modes, although patients reported more restfulness of sleep with volume-assured NIV. Both ventilatory strategies resulted in similar daytime PaCO2 during spontaneous breathing but lower PtCO2 at night with volume-assured NIV (43.2 mmHg with volume-assured NIV versus 37.8 mmHg with high-intensity pressure-preset NIV).
Storre et al.Citation62 investigated whether volume-assured NIV would produce added benefits on PaCO2, nighttime PtCO2, sleep quality, ventilatory patterns, HRQoL (SRI), lung function and exercise capacity compared to high-intensity pressure-preset NIV in 10 patients with COPD and chronic hypercapnic respiratory failure who were already on high-intensity NIV. These patients were switched to 1 of 2 volume-assured NIV strategies: 1 with tidal volume set at 8 ml/kg and 1 with tidal volume set at 110% of individual tidal volume during high-intensity NIV. Patients were then discharged for 3 months on volume-assured pressure-preset NIV using the strategy that produced the lower PtCO2. This complex study did not report any added benefit of volume-assured NIV beyond what was already achieved with high intensity pressure-preset NIV.
Nilius and colleaguesCitation64 compared volume-assured NIV to standard pressure-preset NIV on sleep parameters during a single night (one for each ventilator strategy) in 14 patients with COPD and chronic hypercapnic respiratory failure (PaCO2 ≥ 50 mmHg). The study interventions were delivered over 1 night during which sleep parameters and PtCO2 were recorded. The outcomes were polysomnography-derived sleep parameters (number of respiratory events per hour, sleep time, sleep quality, ventilatory pattern) and nighttime PtCO2. Although investigators used low-intensity NIV (mean IPAP of 18 cmH2O), they could not demonstrate the superiority of volume-assured NIV on nighttime PtCO2 between the 2 modes of ventilation. Ventilatory pressures were slightly higher and respiratory rate slightly lower with volume-assured NIV.
Additional evidence regarding adjustments of ventilatory parameters
The impact of adjusting the ventilatory parameters on physiological and clinical outcomes has been addressed in physiological studies. Adler et al.Citation58 evaluated whether fine adjustments in ventilatory settings could improve quality of sleep and dyspnea in the morning. They enrolled 8 patients with severe stable COPD who were already on long-term NIV, who were adherent to NIV, and who complained of dyspnea after the interruption of NIV. One night of recording was done with the usual ventilatory settings, and 1 night with adjustments of the ventilatory settings to reduce asynchrony. Visual analogue scales were used to quantify sleep quality and dyspnea on the morning following the night of recording. This small study of uncertain clinical significance suggests that fine adjustments of the ventilatory settings maybe useful in some patients with COPD experiencing dyspnea on removal of ventilation. In these patients, small decreases in IPAP and increases in EPAP, small increases in breathing frequency, and slowing time to peak IPAP may improve patient-ventilator synchrony. Future work/research is required to identify whether fine adjustments of ventilatory settings may improve patient comfort and long-term adherence to treatment.
Duiverman et al.Citation53 asked the question as to whether high-intensity pressure-preset NIV could be useful to reduce respiratory muscle activity and provide ventilatory muscle unloading. Ten patients with COPD and chronic hypercapnic respiratory failure already on NIV without exacerbation in the previous month were enrolled. Four ventilatory strategies applied for 15 minutes were assessed during 1 single night of recording: i) low pressure, low frequency NIV; ii) high pressure/low frequency NIV; iii) low pressure/high frequency NIV; and iv) high pressure/high frequency NIV. Low pressure was defined as a maximum pressure of 20 cmH2O, low frequency = 10 breaths/min, high pressure up to 34-35 cmH2O, and high frequency = 2 breaths above natural rate. Surface electromyography (EMG) was used to document the electrical activity of the respiratory muscles and a visual analogue scale was used to quantify comfort. High pressures seemed preferable to reduce respiratory muscle electrical activity and patient/ventilator asynchrony, but this was not statistically significant. No relationship was found between reduction in patient-ventilator asynchrony and comfort.
Good practice points for PICO 2 and 3
Published RCTs are inconclusive regarding the superiority of high versus low-intensity pressure-preset NIV in patients with COPD and chronic hypercapnic respiratory failure. Although this makes it difficult to draw firm conclusions about optimal ventilator settings in patients with COPD, the following concepts are nevertheless emerging:
the initiation period of long-term NIV is a crucial phase to ensure long-term adherence;
the objective of providing significant reductions in PaCO2, which requires the use of high IPAP and possibly controlled respiratory rate, is desirable as this strategy was used in mostCitation5,Citation7 but not all clinical trialsCitation6 with positive results;
the titration procedure should be conducted under close supervision, typically in the hospitalCitation5,Citation7,Citation53,Citation56 with the aim of achieving the largest possible reduction in PaCO2 while ensuring patient’s comfort;
more days are generally required to reach the target ventilatory pressures with high than with low-intensity NIV (3 to 5 days with high-intensity NIV versus 1 to 2 days with low-intensity NIV),Citation39 stressing the complexity of adjusting ventilation in patients with COPD; and
the existing data do not support a benefit of volume-assured NIV beyond what can be achieved with standard pressure-preset NIV.
The inability to reduce PaCO2 with NIV in a given patient should lead to questions regarding benefits of its long-term use, as favorable outcomes are unlikely to be obtained with suboptimal ventilatory parameters. However, such reduction in PaCO2 is not always achievable.Citation7 High pressure NIV (IPAP > 20 cmH2O) may be associated with increased unintentional air leakageCitation39,Citation54 and reduced cardiac output;Citation54 although the latter effect may be limited to patients with compromised cardiac function.Citation53 Typically, low EPAP levels (5 cmH2O) are used to avoid further hyperinflation in these patients. Whether an EPAP level targeting auto-PEEP levels could benefit work-of-breathing is unclear at present.
Future research needs
Information remains relatively scarce on how to best adjust ventilatory settings to improve comfort and adherence to NIV in patients with COPD and chronic hypercapnic respiratory failure. This is an important topic as highlighted by 1 cohort study that investigated whether or not adherence to long-term NIV was associated with reduced re-hospitalization following its initiation in patients with COPD.Citation50 This retrospective analysis of a cohort of 54 patients with COPD suggested that adherence with long-tern NIV for more than 4 hours per day, 70% of days was associated with a lower readmission rate, lower number of readmissions and lower readmission length of stay and readmission related costs. Finding ways to facilitate long-term adherence to therapy is thus an important research priority. In a cross-over study, high-intensity NIV led to greater adherence to the treatment versus low-intensity NIV.Citation39 However, one downside of using high backup frequency is that it may promote gas trapping and this would be expected to have detrimental effects on work of breathing and comfort. To address this issue, the use of high-pressure ventilation in which driving pressures similar to high-intensity NIV are used but at lower backup respiratory rate has been suggested.Citation56 Whether this will prove to be clinically useful remains to be determined. The optimal setting of other parameters such as rise time or inspiratory time also remains to be determined. It is also currently unclear how downloaded reports can help in adjusting settings, and whether, for example, one should target specific inspiratory to expiratory time (“I:E”) ratios or percentage of triggering of breaths by the patient (which may be relevant with regards to inspiratory muscle rest). Besides issues with parameters of ventilation, possible influence of interfaces on adherence to therapy should also be considered. In a cohort of 123 patients with COPD, Callegari and colleagues reported that full-face mask was the preferred interface in 77% of the cohort and that higher IPAP levels were associated with increased use of a full-face mask.Citation65 It remains that the choice of the best interface should be made on an individual basis and identifying the best option may be time consuming.
The most appropriate location to initiate and titrate long-term NIV is also uncertain. In recent clinical trials, the initiation and titration procedures were completed in-hospital, allowing close monitoring and fine adjustments of ventilatory settings to ensure efficacy in reducing PaCO2 or PtCO2 and comfort and tolerance to the treatment.Citation5,Citation7,Citation39 This in-hospital procedure is burdensome in terms of healthcare resources and may not be possible in several jurisdictions. One clinical trial has compared the efficacy of home initiation versus in-hospital initiation of long-term NIV in patients with COPD and chronic hypercapnia.Citation38 The study found that home initiation was as effective as in-hospital initiation to reduce PaCO2 and that it was safe and less costly than in-hospital initiation. Whether home initiation would also lead to similar clinical benefits of long-term NIV when it is initiated in-hospital was not addressed in this study. Also, the home protocol was standardized, and patients were followed with telemedicine technology, including remote monitoring of PtCO2 to adjust the ventilatory parameters. This study provides encouraging results about the feasibility of initiating long-term NIV in patients with COPD outside the hospital but it also the necessity of remote monitoring with recent technology.
Comparison with other guidelines on this topic
Our recommendations are globally in agreement with recently published CPGs of other international organizations (European Respiratory Society [ERS] and American Thoracic Society [ATS]).Citation36,Citation37 A key difference, most notably, concerns the PaCO2 threshold of 52 mmHg that we are proposing for considering the use of long-term NIV in COPD. Though others do not make specific recommendations beyond including “hypercapnic” patients, the ERS acknowledges that “It is likely that the higher level of PaCO2 at enrolment…were major determinants of the enhanced outcome in the HOT-HMV trial.”Citation36
Regarding initiation of NIV after hospitalization, the ERS is less specific in their recommendation; all 3 guidelines (CTS, ATS, and ERS) emphasize the need to reevaluate PaCO2 for persistent hypercapnia, ideally 2-4 weeks after the acute exacerbation, before committing the patient to long-term NIV.
In this guideline, we suggest high-intensity NIV with the objective of reducing PaCO2. The ERS suggests normalizing or reducing PaCO2 whereas the ATS specifically suggest normalization. However, normalization may not be achievable in all patients with severe COPD despite stringent protocols, as seen in studies reviewed in this document.
Fixed pressure support rather than auto-adjusting modes are preferred in this and the ERS guidelines. The ATS makes no recommendation regarding mode of NIV. The ATS suggests not performing sleep laboratory titration, favoring progressive adjustment based on monitoring information provided by the NIV device and daytime pCO2 measurements. The ATS also recommends screening for obstructive sleep apnea, since continuous positive airway pressure (CPAP) rather than NIV might be considered in this group.
Limitations
Data in this CPG were not synthesized in a meta-analytic fashion for each outcome and thus were not aggregated to produce standardized mean differences or risk ratios. However, heterogeneity of study populations and methods may have rendered the results of a meta-analysis difficult to interpret. Instead, we chose to evaluate and describe the methodology of the most important studies impacting our recommendations and eventual clinical decisions. Patient and caregiver input was not sought in the development of this current CPG. This will be addressed in future revisions.
Dissemination and implementation
Our CPG will be disseminated through traditional channels including this publication, through the CTS website and social media channels. Panel members, who come from across Canada, will disseminate recommendations through presentations at the national Canadian Respiratory Conference and in their respective centers and regions. Members will also seek opportunities to present CPGs more widely, through international organizations, journals and conferences. In addition, members who are involved in provincial home ventilation programs will utilize these CPGs in policy development in their jurisdictions.
Conclusion
This 2021 CTS CPG update constitutes a significant shift in the approach to long-term NIV in patients with COPD and chronic hypercapnic respiratory failure, moving from a 2011 recommendation of not using it in most circumstances to a weak/conditional but favorable recommendation supporting its use in this specific context.Citation15 Considering the high prevalence of COPD, which is now one of the most common reasons to initiate long-term NIV in many jurisdictions,Citation12–14 this revised recommendation may place a high burden on the already scarce sleep laboratory and respiratory home-care resources in Canada.
It should be appreciated that the reported benefits of long-term NIV in COPD to improve survival and to reduce hospital readmissions can be expected only under very specific circumstances. Long-term NIV should be offered to highly selected individuals who will adhere to therapy for more than 5 hours per day and in whom long-term NIV is successful in reducing PaCO2 and in controlling nocturnal hypoventilation.Citation5,Citation7,Citation38 Therapy should be considered in the presence of chronic and persistent hypercapnia (PaCO2 ≥ 52 mmHg) and this should be determined after 2-4 weeks of disease stability after an exacerbation.Citation7 Difficulties in reaching these stringent requirements to obtain success with the therapy are highlighted in the high screen failure rates (45 to 95%) or drop-out rates in recent large clinical trials.Citation5,Citation7,Citation38,Citation41
There are also important requirements regarding where and how long-term NIV is initiated. Long-term NIV in COPD should be initiated in a highly controlled environment, typically in the hospital, although an experienced team may succeed at home using remote monitoring.Citation38 The initiation procedure of long-term NIV in COPD is typically cumbersome and time consuming and may not be implementable across the country. This phase of the treatment is nevertheless critical to ensure long-term adherence and success of therapy.
There is currently conflicting evidence regarding the symptomatic benefit of long-term NIV in patients with COPD. As such, it is also important to place these recommendations in the context of patient’s preference and this should be discussed to ensure that expectations toward long-term NIV are realistic.
Long-term NIV has become a therapeutic option for patients with severe COPD and chronic hypercapnic respiratory failure but applicability is limited to highly selected clinical situations, with several unknowns remaining and requiring further research.
Editorial independence
The CTS HMV guideline panel is accountable to the CTS Canadian Respiratory Guidelines Committee and the CTS Board of Directors. The CTS HMV guideline panel is functionally and editorially independent from any funding sources of the CTS and does not receive any direct funding from external sources. The CTS receives unrestricted grants that are combined into a central operating account to facilitate the knowledge translation activities of the CTS Assemblies and its guideline panels. No funders played a role in the collection, review, analysis or interpretation of the scientific literature or in any decisions regarding the key messages presented in this document.
Acknowledgments
The authors would like to recognize and thank CTS staff (Anne Van Dam), CTS Executive members (Drs. Dina Brooks, Paul Hernandez, Richard Leigh, Mohit Bhutani and John Granton), and CTS CRGC Executive members (Samir Gupta, Sanjay Mehta and David Zielinski) for their input and guidance. We would also like to acknowledge with sincere appreciation our expert reviewers who made valuable contributions to the manuscript: Shawn Aaron, University of Ottawa, Ottawa Hospital Research Institute, Ottawa, Canada; Anita Simonds, National Heart and Lung Institute, Imperial College London, Royal Brompton Hospital, London, England; Amanda Piper, University of Sydney, Woolcock Institute of Medical Research, Sydney, Australia.
Disclosure statement
Members of the CTS HMV Guideline Panel declared potential conflicts of interest at the time of appointment and these were updated throughout the process in accordance with the CTS Conflict of Interest Disclosure Policy. Individual member conflict of interest statements are posted at https://cts-sct.ca/guideline-library/.
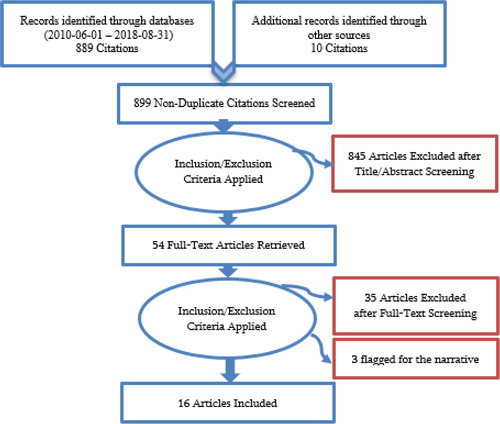
References
- Boushy SF, Thompson HK, Jr., North LB, et al. Prognosis in chronic obstructive pulmonary disease. Am Rev Respir Dis. 1973;108(6):1373–1383. doi:10.1164/arrd.1973.108.6.1373.
- Burrows B, Earle RH. Course and Prognosis of Chronic Obstructive Lung Disease. A prospective study of 200 patientsN Engl J Med. 1969;280(8):397–404. doi:10.1056/NEJM196902202800801.
- Casanova C, Celli BR, Tost L, et al. Long-term controlled trial of nocturnal nasal positive pressure ventilation in patients with severe COPD. Chest. 2000;118(6):1582–1590. doi:10.1378/chest.118.6.1582.
- Clini E, Rehabilitation and Chronic Care Study Group, Italian Association of Hospital Pulmonologists (AIPO), Sturani C, Rossi A, et al. The Italian multicentre study on noninvasive ventilation in chronic obstructive pulmonary disease patients. Eur Respir J. 2002;20(3):529–538. doi:10.1183/09031936.02.02162001.
- Kohnlein T, Windisch W, Kohler D, et al. Non-invasive positive pressure ventilation for the treatment of severe stable chronic obstructive pulmonary disease: a prospective, multicentre, randomised, controlled clinical trial. The Lancet. Respiratory Medicine. 2014;2(9):698–705. doi:10.1016/S2213-2600(14)70153-5.
- McEvoy RD, on behalf of the Australian trial of non-invasive Ventilation in Chronic Airflow Limitation (AVCAL) Study Group, Pierce RJ, Hillman D, et al. Nocturnal non-invasive nasal ventilation in stable hypercapnic COPD: a randomised controlled trial. Thorax. 2009;64(7):561–566. doi:10.1136/thx.2008.108274.
- Murphy PB, Rehal S, Arbane G, et al. Effect of home noninvasive ventilation with oxygen therapy vs oxygen therapy alone on hospital readmission or death after an acute COPD exacerbation: A randomized clinical trial. JAMA. 2017;317(21):2177–2186. doi:10.1001/jama.2017.4451.
- Cheung APS, Chan VL, Liong JT, et al. A pilot trial of non-invasive home ventilation after acidotic respiratory failure in chronic obstructive pulmonary disease. The International Journal of Tuberculosis and Lung Disease : The Official Journal of the International Union against Tuberculosis and Lung Disease. 2010;14(5):642–649.
- AF, ConnorsJr, Dawson NV, Thomas C, et al. Outcomes following acute exacerbation of severe chronic obstructive lung disease. The SUPPORT investigators (Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments). Am J Respir Crit Care Med. 1996;154(4 Pt 1):959–967. doi:10.1164/ajrccm.154.4.8887592.
- Shah T, Churpek MM, Coca Perraillon M, et al. Understanding why patients with COPD get readmitted: a large national study to delineate the Medicare population for the readmissions penalty expansion. Chest. 2015;147(5):1219–1226. doi:10.1378/chest.14-2181.
- Osadnik CR, Tee VS, Carson‐Chahhoud KV, et al. Non‐invasive ventilation for the management of acute hypercapnic respiratory failure due to exacerbation of chronic obstructive pulmonary disease. Cochrane Database of Syst Rev. 2017;7(7):CD004104.
- Lloyd-Owen SJ, Donaldson GC, Ambrosino N, et al. Patterns of home mechanical ventilation use in Europe: results from the Eurovent survey. Eur Respir J. 2005;25(6):1025–1031. doi:10.1183/09031936.05.00066704.
- Schwarz EI, Mackie M, Weston N, et al. Time-to-death in chronic respiratory failure on home mechanical ventilation: A cohort study. Respir Med. 2020;162:105877. doi:10.1016/j.rmed.2020.105877.
- Patout M, Lhuillier E, Kaltsakas G, et al. Long-term survival following initiation of home non-invasive ventilation: A European study. Thorax. 2020;75(11):965–973. doi:10.1136/thoraxjnl-2019-214204.
- McKim DA, Canadian Thoracic Society Home Mechanical Ventilation Committee, Road J, Avendano M, et al. Home Mechanical Ventilation: A Canadian Thoracic Society Clinical Practice Guideline. Can Respir J. 2011;18(4):197–215. doi:10.1155/2011/139769.
- Meecham Jones DJ, Paul EA, Jones PW, et al. Nasal pressure support ventilation plus oxygen compared with oxygen therapy alone in hypercapnic COPD. Am J Respir Crit Care Med. 1995;152(2):538–544. doi:10.1164/ajrccm.152.2.7633704.
- Ambrosino N, Montagna T, Nava S, et al. Short term effect of intermittent negative pressure ventilation in COPD patients with respiratory failure. Eur Respir J. 1990;3(5):502–508.
- Petrof BJ, Kimoff RJ, Levy RD, et al. Nasal Continuous Positive Airway Pressure Facilitates Respiratory Muscle Function during Sleep in Severe Chronic Obstructive Pulmonary Disease. Am Rev Respir Dis. 1991;143(5 Pt 1):928–935. doi:10.1164/ajrccm/143.5_Pt_1.928.
- Elliott MW, Mulvey DA, Moxham J, et al. Domiciliary nocturnal nasal intermittent positive pressure ventilation in COPD: mechanisms underlying changes in arterial blood gas tensions. Eur Respir J. 1991;4(9):1044–1052.
- Brouwers MC, AGREE Next Steps Consortium, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010;182(18):E839–842. doi:10.1503/cmaj.090449.
- Higgins JP, Cochrane Statistical Methods Group, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928 doi:10.1136/bmj.d5928.
- Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–394. doi:10.1016/j.jclinepi.2010.04.026.
- Alonso-Coello P, Schünemann HJ, Moberg J, et al. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. (Clinical Research ed.). 2016;353:i2016.
- Gupta S, Rai N, Bhattacharrya O, et al. Optimizing the language and format of guidelines to improve guideline uptake. CMAJ. 2016;188(14):E362–e368. doi:10.1503/cmaj.151102.
- Atkins D, Best D, Briss PA, et al. Grading quality of evidence and strength of recommendations. BMJ (Clinical Research ed.). 2004;328(7454):1490.
- Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ (Clinical Research ed.). 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD.
- Bhatt SP, Peterson MW, Wilson JS, et al. Noninvasive positive pressure ventilation in subjects with stable COPD: a randomized trial. Int J Chron Obstruct Pulmon Dis. 2013;8:581–589.
- Duiverman ML, Wempe JB, Bladder G, et al. Two-year home-based nocturnal noninvasive ventilation added to rehabilitation in chronic obstructive pulmonary disease patients: A randomized controlled trial. Respir Res. 2011;12(1):112. doi:10.1186/1465-9921-12-112.
- Garrod R, Mikelsons C, Paul EA, et al. Randomized controlled trial of domiciliary noninvasive positive pressure ventilation and physical training in severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;162(4):1335–1341. Pt doi:10.1164/ajrccm.162.4.9912029.
- Márquez-Martín E, Ruiz FO, Ramos PC, et al. Randomized trial of non-invasive ventilation combined with exercise training in patients with chronic hypercapnic failure due to chronic obstructive pulmonary disease. Respir Med. 2014;108(12):1741–1751. doi:10.1016/j.rmed.2014.10.005.
- Strumpf DA, Millman RP, Carlisle CC, et al. Nocturnal Positive-Pressure Ventilation via Nasal Mask in Patients with Severe Chronic Obstructive Pulmonary Disease. Am Rev Respir Dis. 1991;144(6):1234–1239. doi:10.1164/ajrccm/144.6.1234.
- Zhou L, Li X, Guan L, et al. Home noninvasive positive pressure ventilation with built-in software in stable hypercapnic COPD: a short-term prospective, multicenter, randomized, controlled trial. Int J Chron Obstruct Pulmon Dis. 2017;12:1279–1286. doi:10.2147/COPD.S127540.
- Oscroft NS, Quinnell TG, Shneerson JM, Smith IE. The effects of withdrawing long-term nocturnal non-invasive ventilation in COPD patients. COPD: Chronic Obstr Pulm Dis J. 2010;7(2):111–116. doi:10.3109/15412551003631725.
- Gay PC, Hubmayr RD, Stroetz RW. Efficacy of nocturnal nasal ventilation in stable, severe chronic obstructive pulmonary disease during a 3-month controlled trial. Mayo Clin Proc. 1996;71(6):533–542. doi:10.4065/71.6.533.
- Struik FM, Lacasse Y, Goldstein RS, et al. Nocturnal noninvasive positive pressure ventilation in stable COPD: a systematic review and individual patient data meta-analysis. Respir Med. 2014;108(2):329–337. doi:10.1016/j.rmed.2013.10.007.
- Ergan B, Oczkowski S, Rochwerg B, et al. European Respiratory Society guidelines on long-term home non-invasive ventilation for management of COPD. Eur Respir J. 2019;54(3):1901003. doi:10.1183/13993003.01003-2019.
- Macrea M, Oczkowski S, Rochwerg B, et al. Long-Term Noninvasive Ventilation in Chronic Stable Hypercapnic Chronic Obstructive Pulmonary Disease. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020;202(4):e74–e87. doi:10.1164/rccm.202006-2382ST.
- Duiverman ML, Vonk JM, Bladder G, et al. Home initiation of chronic non-invasive ventilation in COPD patients with chronic hypercapnic respiratory failure: a randomised controlled trial. Thorax. 2020;75(3):244–252. doi:10.1136/thoraxjnl-2019-213303.
- Dreher M, Storre JH, Schmoor C, et al. High-intensity versus low-intensity non-invasive ventilation in patients with stable hypercapnic COPD: a randomised crossover trial. Thorax. 2010;65(4):303–308. doi:10.1136/thx.2009.124263.
- de Backer L, Vos W, Dieriks B, et al. The effects of long-term noninvasive ventilation in hypercapnic COPD patients: A randomized controlled pilot study. Int J Chron Obstruct Pulmon Dis. 2011;6(1):615–624. doi:10.2147/COPD.S22823.
- Struik FM, Sprooten RTM, Kerstjens HAM, et al. Nocturnal non-invasive ventilation in copd patients with prolonged hypercapnia after ventilatory support for acute respiratory failure: A randomised, controlled, parallel-group study. Thorax. 2014;69(9):826–834. doi:10.1136/thoraxjnl-2014-205126.
- Redolfi S, Grassion L, Rivals I, et al. Abnormal Activity of Neck Inspiratory Muscles during Sleep as a Prognostic Indicator in Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2020;201(4):414–422. doi:10.1164/rccm.201907-1312OC.
- Borel J-C, Pepin J-L, Pison C, et al. Long-term adherence with non-invasive ventilation improves prognosis in obese COPD patients. Respirology (Carlton, Vic.). 2014;19(6):857–865. doi:10.1111/resp.12327.
- Lacasse Y, LaForge J, Maltais F. Got a match? Home oxygen therapy in current smokers. Thorax. 2006;61(5):374–375. doi:10.1136/thx.2006.060749.
- Mummery V, Matthew D, Brown C, et al. P195 INTU: improving non-invasive ventilation (NIV) through understanding. Using patient experience to improve acute NIV provision as part of a quality improvement project. Thorax. 2018. 73(Suppl 4):A206-A206. doi:10.1136/thorax-2018-212555.352.
- West GA, Primeau P. Nonmedical hazards of long-term oxygen therapy. Respir Care. 1983;28(7):906–912.
- Khakban A, Sin DD, FitzGerald JM, et al. Ten-Year Trends in Direct Costs of COPD: A Population-Based Study. Chest. 2015;148(3):640–646. doi:10.1378/chest.15-0721.
- Goss T, Criner G, Gu Q, et al. Cost-effectiveness of Home Oxygen Therapy-Home Mechanical Ventilation (HOT_HMV) for treatment of COPD with chronic hypercapnic respiratory failure following an acute exacerbation of COPD in the US. Chest. 2018;154(4):782A–783A. doi:10.1016/j.chest.2018.08.704.
- Murphy PB, Brueggenjuergen B, Reinhold T, et al. Cost-effectiveness of home oxygen therapy-home mechanical ventilation (HOT-HMV) for the treatment of chronic obstructive pulmonary disease (COPD) with chronic hypercapnic respiratory failure following an acute exacerbation of COPD in the United Kingdom (UK). Am J Respir Crit Care Med. 2018;308:A2517-A2517. https://doi.org/10.1164/ajrccm-conference.2018.197.1_MeetingAbstracts.A2517.
- Satici C, Arpinar Yigitbas B, Seker B, et al. Does Adherence to Domiciliary NIMV Decrease the Subsequent Hospitalizations Rates and Cost for Patients Diagnosed with COPD. Int J Chron Obstruct Pulmon Dis. 2018;15(3):303–309. doi:10.1080/15412555.2018.1500532.
- Coughlin S, Liang WE, Parthasarathy S. Retrospective Assessment of Home Ventilation to Reduce Rehospitalization in Chronic Obstructive Pulmonary Disease. J Clin Sleep Med. 2015;11(06):663–670. doi:10.5664/jcsm.4780.
- Arnal JM, Texereau J, Garnero A. Practical Insight to Monitor Home NIV in COPD Patients. Copd. 2017;14(4):401–410. doi:10.1080/15412555.2017.1298583.
- Duiverman ML, Maagh P, Magnet FS, et al. Impact of High-Intensity-NIV on the heart in stable COPD: A randomised cross-over pilot study. Respir Res. 2017;18(1):76 doi:10.1186/s12931-017-0542-9.
- Lukacsovits J, Carlucci A, Hill N, et al. Physiological changes during low- and high-intensity noninvasive ventilation. Eur Respir J. 2012;39(4):869–875. doi:10.1183/09031936.00056111.
- Windisch W, Storre JH, Köhnlein T. Nocturnal non-invasive positive pressure ventilation for COPD. Expert Rev Respir Med. 2015;9(3):295–308. doi:10.1586/17476348.2015.1035260.
- Murphy PB, Brignall K, Moxham J, et al. High pressure versus high intensity noninvasive ventilation in stable hypercapnic chronic obstructive pulmonary disease: A randomized crossover trial. Int J Chron Obstruct Pulmon Dis. 2012;7:811–818.
- Díaz O, Bégin P, Torrealba B, et al. Effects of noninvasive ventilation on lung hyperinflation in stable hypercapnic COPD. Eur Respir J. 2002;20(6):1490–1498. doi:10.1183/09031936.02.00034402.
- Adler D, Perrig S, Takahashi H, et al. Polysomnography in stable COPD under non-invasive ventilation to reduce patient-ventilator asynchrony and morning breathlessness. Sleep Breath. 2012;16(4):1081–1090. doi:10.1007/s11325-011-0605-y.
- Kerl J, Höhn E, Köhler D, et al. Spontaneous-timed versus controlled noninvasive ventilation in chronic hypercapnia - a crossover trial. MDER. 2019;12:173–181. doi:10.2147/MDER.S190841.
- Windisch W, Dreher M, Geiseler J, et al. Guidelines for Non-Invasive and Invasive Home Mechanical Ventilation for Treatment of Chronic Respiratory Failure - Update. Pneumologie (Stuttgart, Germany. 2017;71(11):722–795.
- Oscroft NS, Ali M, Gulati A, et al. A randomised crossover trial comparing volume assured and pressure preset noninvasive ventilation in stable hypercapnic COPD. COPD: Journal of Chronic Obstructive Pulmonary Disease. 2010;7(6):398–403. doi:10.3109/15412555.2010.528084.
- Storre JH, Matrosovich E, Ekkernkamp E, et al. Home mechanical ventilation for COPD: High-intensity versus target volume noninvasive ventilation. Respir Care. 2014;59(9):1389–1397. doi:10.4187/respcare.02941.
- Ekkernkamp E, Storre JH, Windisch W, Dreher M. Impact of intelligent volume-assured pressure support on sleep quality in stable hypercapnic chronic obstructive pulmonary disease patients: A randomized, crossover study. Respiration. 2014;88(4):270–276. doi:10.1159/000364946.
- Nilius G, Katamadze N, Domanski U, Schroeder M, Franke K-J. Non-invasive ventilation with intelligent volume-assured pressure support versus pressure-controlled ventilation: effects on the respiratory event rate and sleep quality in COPD with chronic hypercapnia. Int J Chron Obstruct Pulmon Dis. 2017;12:1039–1045. doi:10.2147/COPD.S126970.
- Callegari J, Magnet FS, Taubner S, et al. Interfaces and ventilator settings for long-term noninvasive ventilation in COPD patients. COPD. 2017;12:1883–1889. doi:10.2147/COPD.S132170.
Appendix 1.
Inclusion/exclusion criteria and citation flow
Study Inclusion/Exclusion Criteria and Screening: We included only randomized clinical trials for further review and inclusion. Other study designs and studies published in a language other than English were excluded. The chosen inclusion and exclusion criteria were noted at the abstract and full text review stages.