
ABSTRACT
Objectives: The relation between rapid infancy weight gain (RWG) and childhood obesity has been extensively evaluated but studies examining total food intake and food groups among infants with RWG and normal weight gain (NWG) are limited. Therefore, we aimed to explore: (i) the characteristics of infants with a rapid growth during the second semester of life; (ii) the association between feeding practices (breast-fed vs. formula-fed infants) and RWG and (iii) the association between food intake and food patterns at 9 months of age and RWG.
Study design: One-year follow-up study of a cohort of infants from the north of Spain.
Methods: 195 infants were measured. Parents recorded all infant´s food consumption for 3 days (grams/day). Mixed-effects logistic regression models were applied.
Results: In basic models, breast-feeding practices were associated with a lower risk of RWG (OR = 0.54, 95%CI 0.35–0.84) compared to formula-fed infants. However, this association was no longer significant when additionally adjusting for early-life risk factors and total food intake. Infants with RWG had a higher intake of cereals (OR = 1.03, 95%CI 1.00–1.07), fruit baby food (OR = 1.01, 95%CI 1.00–1.01), and total food intake (OR = 1.02, 95%CI 1.00–1.04) at 9 months of age.
Conclusions: Infants with rapid growth during the second semester of life had a higher intake of cereals, fruit baby food, and total food intake compared to the NWG group. Differences in food patterns and intake among infants with rapid weight gain during the second semester might lead to programming towards childhood obesity.
Introduction
Childhood obesity is a major health problem in Spain and around the world (WHO Citation2018). According to the latest data from the World Health Organization (WHO), more than 40% of the infants in southern European countries are overweight or obese (WHO Citation2018). Pregnancy and infancy are important life stages to prevent childhood obesity (Robinson et al. Citation2015). Smoking during pregnancy, parental overweight and obesity, and rapid infancy weight gain (RWG) are potentially modifiable risk factors of childhood obesity (Dennison et al. Citation2006; Weng et al. Citation2012; Iguacel et al. Citation2018). Among these potentially modifiable early life risk factors, RWG has been identified as the strongest risk factor for the onset of childhood obesity (Iguacel et al. Citation2018; Zheng et al. Citation2018). RWG has been generally defined as an increase of >0.67 in sex-specific weight-for-age z-score within a specific time period, representing biologically significant weight gain coincident with crossing one major percentile line on a growth chart (Ong and Loos Citation2006).
Weight gain during infancy has been linked with feeding practices (Mihrshahi et al. Citation2011; Li et al. Citation2012). The WHO recommends exclusive breastfeeding for the first 6 months of life with continued breastfeeding along with appropriate complementary food up to 2 years of age or beyond (WHO Citation2018). Breast-fed infants have a lower growth rate compared to formula-fed infants (Goetz et al. Citation2018). The higher protein and energy density of the formula act as a stimulus for the secretion of insulin-like growth, which meliorate the synthesis of protein as well as cell proliferation (Schack-Nielsen and Michaelsen Citation2007). Also, there is evidence that a higher protein intake during infancy increase weight gain and greater adiposity (Escribano et al. Citation2012; Luque et al. Citation2015). As a result, formula-fed infants have accelerated growth and increased muscle mass and adipose tissue compared to breast-fed infants (Ziegler Citation2006).
Although most of the small for gestational age infants show rapid early postnatal growth and weight gain (Ong Citation2007), the concept of healthy catch-up growth in these infants should be assessed to compare the benefits and disadvantages of rapid early growth (de Zegher et al. Citation2013).
To the best of our knowledge, no studies have described the characteristics of infants who experience RWG during the second semester of life assessing the association between food patterns at 9 months of age and RWG experience from 6 to 12 months of age.
We hypothesize that infants who have a rapid weight gain during the second semester of life are more likely to have a lower birth weight and gestational age, being formula-fed infants and having a higher intake of each food group. These infant characteristics finally lead to increased subsequent obesity risk. The present paper aims to explore: (i) the characteristics of infants who have a rapid growth during the second semester of life; (ii) the association between feeding practices (breast-fed vs. formula-fed infants) and RWG and (iii) the association between food patterns at 9 months of age and RWG in a cohort of infants from Spain.
Methods
Design and study population
A cohort of infants from different localities in the north of Spain (situated in the province of Huesca and Santander) was included in the present investigation. Infants who did not have any malformation, diseases or physical disabilities that could affect the growth and the nutritional status were excluded for our study. Infants were randomly selected from Primary Care Centres participating at the Spanish Child Health Program from March to July 2011 and were followed for 1 year (from 6 months of age to 18 months of age). The localities chosen for the present study were selected because the logistic capacity related with the geographic proximity of the involved research groups but also because they had previous experience in the area and some of the research members were working in the Primary Care Centres studied.
The general aims of the study were: (i) to assess children’s growth patterns and body composition; (ii) to study children’s feeding patterns and common-related digestive conditions, such as digestive tolerance, satiety, and depositions, and (iii) to examine early-life and socio-cultural factors which might have an influence on them.
In total 272 families were contacted during the scheduled appointment at 6 months of age in the Spanish Child Health Program to participate in the study and 245 accepted to participate in the study (acceptance rate 90%). These 245 new-born infants without any malformation, diseases or physical disabilities were examined at birth and periodically re-examined in Primary Care Centres at 6, 9 and 12, 15, and 18 months of age. After 1-year follow-up 61 infants did no longer participate in our study; thus, the retention rate was 75%. Fifty infants who had missing values in any of the exposures, covariates or outcomes were excluded from the analysis. Finally, the analysis included 195 infants (55.4% boys).
Parents or legal guardians gave written informed consent for examinations for their infants. Ethical approval was obtained from Aragon’s Committee of Ethics in Clinical Research (CEICA).
Measurements
Outcome measure (rapid infancy weight gain)
Age- and sex-specific weight z-scores at birth, at 6, 9, 12, and 15 months of age were computed using child growth standards tables from the WHO (Citation2006). Infant weight gain was calculated as gain in weight z-score between 6 months and 12 months of life. Early rapid infant body weight gain was defined as an increase in body weight z-score above +0.67 standard deviation (SD) from 6 months of age to 12 months of age (Ong and Loos Citation2006).
Exposures
Breastfeeding or formula-feeding practices at 9 months of age
Infant feeding practices (formula, breastfeeding or mixed feeding) at the age of 9 months were reported by the mothers. In particular, mothers were asked to inform about the duration of the exclusive breastfeeding (if the case), weaning time, introduction of formula feeding and intake of each food group during the introduction of complementary food.
Considering this information infants were categorized in two groups according to their feeding practices at 9 months of age: breast-fed (including infants who were both breast-fed and formula-fed) and formula-fed infants (infants who were just formula-fed).
Food groups intake at age of 9 months
A 24-h dietary recall interview was conducted in the Primary Care Centres to record all infant’s food consumption (in grams or cubic centimeters-cc a day). The intake of the following food groups was collected during the interview with parents, before the programmed visits at 9 months of age: (i) cereals (single grain cereals in powder to be mixed with water or formula), (ii) fruit baby food, (iii) vegetables with meat or fish baby food, (iv) formula, and (v) yogurt. Those intakes that were reported in cc were converted into grams.
Total food intake (grams/day) was calculated by summing the quantity of cereals, fruit baby food, vegetables with proteins, baby foods, infant formula, and yogurt.
In the present study, we have focused on infants at the age of 9 months because during this period the transition from exclusive breastfeeding to family foods, referred to as complementary feeding, should have already been established with the consumption of a large variety of foods. Moreover, 9 months of age is a representative period for quantifying the food and to assess infant food patterns. At this age infants eat a variety of food that can be easily assessed because usually they are in a liquid or smashed status that before (i.e. at 6 months) or after (i.e. at 18 months) would not be possible.
Weight, length, and body mass index at birth and at age 6, 9, and 12 months
Trained staff measured the length and weight of the infants by using the homologated SECA® 374 medical digital baby scale. Length and weight of the infants were measured in a fasting state without any clothes and shoes using a recumbent board to the nearest 0.1 cm and body weight was recorded in kg to the nearest 10 g. Age- and sex-specific weight, length and body mass index (BMI) z-scores at birthweight and at age 6, 9, 12, 15, and 18 months were calculated using the WHO reference data (WHO Citation2006). BMI was calculated by dividing body weight in kilograms by squared body length in meters and then transformed into age- and sex-specific z-score.
Potential confounding factors
Parental education
Parents indicated their maximum educational attainment level by an individual face-to-face interview. Particular response categories were coded according to International Standard Classification of Education (ISCED 1997) (Statistics. UNESaCOUIf) and re-categorized into three categories: low (0–2), medium (3–4) and high (5–6) ISCED educational levels.
Early-life risk factors
By a face-to-face interview parents also reported the gestational age and birth weight of the infant as well as pre-pregnancy weight and length. Afterward, paternal and maternal BMI were calculated.
Statistical analyses
We investigated whether characteristic of the infants (sex, feeding practices at 9 months, parental education and parental BMI, gestational age, birth weight, group food intakes, total food intake at 9 months and infant’s weight z-score, length z-score, and BMI z-score at birth, age 6, 9, and 12 months of age) differed according to RWG. Group differences were tested by chi-square goodness of fit analysis for categorical variables and unpaired t-test for independent samples was used to compare means of continuous variables.
Moreover, to test the associations between feeding practices at 9 months (breast-fed vs. formula-fed infants) and RWG (yes/no) logistic mixed-effect models were applied. To adjust for possible confounders, three different models were run: model 1 was adjusted for sex; model 2, was additionally adjusted for gestational age, birth weight, parental education, parental BMI, and weight at 6 months, and model 3 was additionally adjusted for total food intake in grams/day (sum of cereals, carbohydrates, fruit baby food, vegetables with proteins, baby food excluding infant formula, and breast milk in grams/day).
Additionally, to test the associations between each food group intake and total food intake (grams/day) at age 9 months and RWG from 6 to 12 months of age, logistic mixed-effect models were applied. To adjust for possible confounders, two different models were run: model 1 was adjusted for sex and model 2, was additionally adjusted for gestational age, birth weight, parental education, parental BMI, and weight at 6 months.
For all models, the reference category used was NWG.
Significance level was set at 0.05. Analyses were performed using the Statistical Package for the Social Sciences (version 22.0; SPSS, Inc.).
Results
summarises the characteristics of infants (sex, feeding practices at 9 months, parental education and parental BMI, gestational age, birth weight, group food intakes, and total food intake at 9 months) by RWG (yes/no) from 6 months to 12 months of age. Number of participants and percentages are shown for categorical variables and mean and standard deviation (SD) for continuous variables. RWG was not markedly different from infant’s characteristics of feeding practices, sex, paternal education, and parental BMI although formula-fed infants had a higher percentage of RWG (29.7%) compared to breast-fed infants (18.4%). Infants who presented RWG had a lower mean gestational age (38.42 vs 39.26 weeks), p < 0.002, had also a higher mean intake of cereals (26.69 vs 23.00 g/day), p < 0.026, fruit baby food (225.10 vs 190.78 g/day), p < 0.004, and a total intake of food when excluding formula and breast milk (1075.92 vs 956.03 g/day), p < 0.003, compared to those infants who did not present a rapid weight gain.
Table 1. Characteristics of children (sex, feeding practices at 9 months, parental education and parental BMI, gestational age, birth weight, group food intakes, and total food intake at 9 months) by rapid infancy weight gain (yes/no) from 6 months to 12 months of age. Number of participants and percentages are shown for categorical variables and mean and standard deviation (SD) for continuous variables.
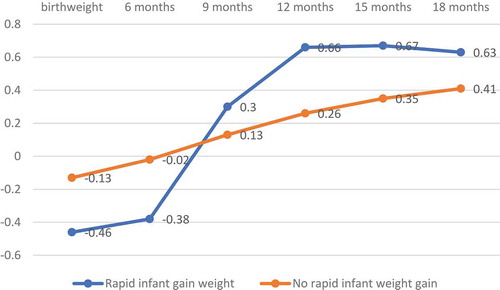
– show infants’ weight z-score, length z-score, and BMI z-score at 6, 9, 12, 15, and 18 months of age based on infants’ rapid infant weight gain (yes/no) experienced from 6 months to 12 months. Mean and standard deviation (SD) are reported. At birth, infants who experienced RWG did not differ statistically significantly in weight (−0.12 vs −0.03), length (−0.36 vs −0.07), and BMI z-score (−0.46 vs −0.13) compared to those who did not have an RWG. At 6 months, infants who experienced RWG differed statistically significantly in weight (−0.22 vs 0.18), and BMI z-score (−0.38 vs −0.02) but not in length (0.10 vs 0.34) compared to those who did not have an RWG. At 9 months, infants who had an RWG did not statistically differ significantly in weight (0.40 vs 0.27), length (0.32 vs 0.31), and BMI z-score (0.30 vs 0.13) compared to those who did not have an RWG. However, at 12 months of age, infants who experienced RWG compared to those who did not have an RWG had a statistically significant higher weight (0.77 vs 0.33), and BMI z-score (0.66 vs 0.26) but did not differ significantly in length (0.51 vs 0.26). Finally, similar patterns were found at 15 and 18 months of age. Particularly, at 15 months of age infants who experienced RWG compared to those who did have an NWG had a statistically significant higher weight (0.86 vs 0.42), length (0.68 vs 0.33), and BMI z-score (0.67 vs 0.35). Likewise, at 18 months differences remained significant for weight (0.90 vs 0.50), length (0.75 vs 0.38), but not for BMI (0.64 vs 0.41) in those with an RWG and NWG, respectively.
Figure 1. Children’s rapid infant weight gain (yes/no) based on children´s weight z-score at birth and at 6, 9 and 12, 15, and 18 months of age. Mean is reported.
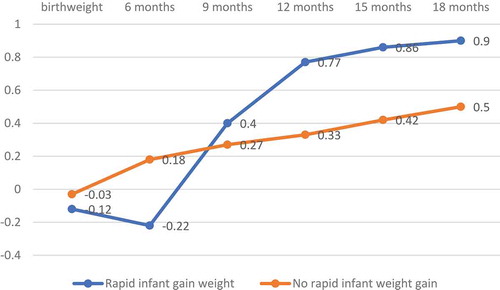
Figure 2. Children’s rapid infant weight gain (yes/no) based on children´s height z-score at birth and at 6, 9 and 12, 15, and 18 months of age. Mean is reported.
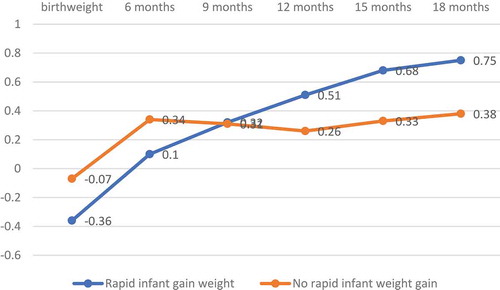
Figure 3. Children’s rapid infant weight gain (yes/no) based on children´s BMI z-score at birth and at 6, 9 and 12, 15, and 18 months of age. Mean is reported.
presents the odds ratio (OR) and 95% confidence intervals (CI) and p-values for models assessing the associations between breastfeeding status at age 9 months and RWG from 6 to 12 months of age. In the basic model (adjusted for sex), breast-feeding practices were associated with a lower risk of RWG (OR = 0.54, 95%CI 0.35–0.84) compared to formula-fed infants. This association was no longer significant in model 2 when additionally adjusting for gestational age, birth weight, parental education, parental BMI, and weight at 6 months (OR = 0.62, 95%CI 0.26–1.52) and model 3 (additionally adjusted for total food intake in grams/day) (OR = 0.49, 95%CI 0.29–1.80).
Table 2. Associations between feeding practices at age 9 months and rapid infancy weight gain from 6 to 12 months of age. Results from the logistic regressions modelsa. Odds Ratio (OR), 95% confidence intervals (CI), and p-values are shown.
represents the associations between each food group intake (grams/day) at age 9 months and RWG from 6 to 12 months of age. In fully adjusted models (after adjusting for sex, gestational age, birth weight, maternal and paternal BMI, and maternal and paternal education) a higher intake of cereals (OR = 1.03, 95%CI 1.00–1.07), of fruit baby food (OR = 1.01, 95%CI 1.00–1.01) and total food intake (OR = 1.02, 95%CI 1.00–1.04) at 9 months of age was associated with a higher risk of RWG. No other statistically significant associations were found between intake of yogurt, formula, and vegetables with proteins at 9 months and RWG from 6 to 12 months of age.
Table 3. Associations between each food group intake (grams/day) at age 9 months and rapid infancy weight gain from 6 to 12 months of age. Results from the logistic regressions models. Odds Ratio (OR), 95% confidence intervals (CI), and p-values are shown.
Discussion
In this cohort analysis, we described the characteristics of infants with rapid weight gain during the second semester of life and we investigated the association between feeding practices and food intake with RWG in a cohort of infants from Spain.
The results of the present study suggest that infants who showed rapid weight gain during the second semester of life had a higher total food intake at 9 months of age, after adjusting for sex, gestational age, birth weight, maternal and paternal BMI, and maternal and paternal education. This difference in the total food intake was mainly due to the higher intake of cereals but also, although in a lower proportion, due to a higher intake of fruit baby food. The consumption of cereals in powder by Spanish infants is a common practice. These cereals are usually added to water or milk (breastmilk or formula). We found that while infants with a rapid weight gain exhibited a lower mean weight-, length-, and BMI z-score at birth and at 6 months of age, at 9 months these infants already showed a higher mean weight-, length-, and BMI z-score compared to the NWG group and these differences were more apparent at 12 months of age. Similar to our study several papers have shown the different evolution in the anthropometric patterns between the rapid weight gain group and the no rapid weight gain group (Ibanez et al. Citation2006; Nanri et al. Citation2017).
In other studies, it have been demonstrated that during the period of complementary feeding (6–18 months of age), higher protein intake would lead to increased BMI and greater risk of later obesity (Gunther et al. Citation2006; Ohlund et al. Citation2010). Formula-feeding practices might be a risk factor for rapid infant weight gain (Mihrshahi et al. Citation2011) because formula-feeding result in higher protein-derived short-chain fatty acids and amino acids in stools. Moreover, formula-fed infants are different from breast-fed infants, at the level of lipid and energy metabolism (Martin et al. Citation2014). On the other hand, breastfeeding might promote satiety responsiveness because the infant has a greater opportunity to regulate their intake of milk in comparison to bottle-fed infants (Brown and Lee Citation2012). In our study,however, although basic models (only adjusted for sex) displayed a lower risk of developing RWG associated with breastfeeding, when adjusting for gestational age, birth weight, parental education, parental BMI, weight at 6 months, and total food intake in grams/day this relationship became no longer statistically significant.
According to the results of our investigation, RWG is the result of higher food intake rather than previous metabolic characteristics. Nonetheless, the small size of our study does not allow us to state whether the protective effect of breastfeeding could be more due to the effect of these covariates rather than the effect of breastfeeding may have itself.
A special strength of the present study is the fact that we are not aware of any study that has assessed the intakes of the different food groups at age 9 months to discuss its relationship with RWG including trajectories of growth in a Spanish cohort of infants. Additionally, by quantifying food intake at 9 months of age using grams a day instead of the amount of energy (the number of kilocalories – kcal–) we have avoided unnecessary bias because at this age food intake can be easily measured in grams since most of the food is mashed.
Nevertheless, the findings of the present study are not without limitations. Firstly, the small size of the sample (N = 198) might undermine the chance of detecting a true effect and the reproducibility of results. Additionally, the small range of the OR detected in the present study hinders the establishment of significant clinical correlations and conclusions. Secondly, a selection bias cannot be precluded since most of the parents participating in this study have high socioeconomic status (more than half of the mothers included in this study had a high education) (Galea and Tracy Citation2007). Thirdly, we have to take into account that some measures were self-reported (e.g. parental BMI or infant´s intake of the different food items reported by parents). Moreover, this study was limited by a geographically restricted sample of the north of Spain and therefore this study is not a representative sample of this country. Finally, the information on food consumption among the infants was collected using a single 24-h dietary recall. One 24-h recall cannot be sufficient to provide estimates of the intakes to a certain extent because there are random errors due to day-to-day variation in individual diets (Luque et al. Citation2013).
Conclusion
Children with a rapid infant weight gain during the second semester of life have a higher total food intake (especially due to a higher intake of cereals and fruit baby food). These results highlight the importance that the second semester of life might have to prevent future childhood obesity.
Authors’ contributions
The authors’ contributions were as follows: I.I carried out the statistical analysis and drafted the manuscript. L.M, M.J.C, L.AM, P.S, M.R.P, M.R, L.A, G.R. conducted and supervised the data collection. All the authors read and critically reviewed the manuscript.
Acknowledgments
I. I was supported by the FPU Predoctoral Programs (grant reference FPU014/00922) of the Spanish Ministry of Education and Science.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Brown A, Lee M. 2012. Breastfeeding during the first year promotes satiety responsiveness in children aged 18-24 months. Pediatr Obes. 7(5):382–390.
- de Zegher F, Sebastiani G, Diaz M, Gomez-Roig MD, Lopez-Bermejo A, Ibanez L. 2013. Breast-feeding vs formula-feeding for infants born small-for-gestational-age: divergent effects on fat mass and on circulating IGF-I and high-molecular-weight adiponectin in late infancy. J Clin Endocrinol Metab. 98(3):1242–1247.
- Dennison BA, Edmunds LS, Stratton HH, Pruzek RM. 2006. Rapid infant weight gain predicts childhood overweight. Obesity (Silver Spring). 14(3):491–499.
- Escribano J, Luque V, Ferre N, Mendez-Riera G, Koletzko B, Grote V,Demmelmair H, Bluck L, Wright A, Closa-Monasterolo R et al. 2012. Effect of protein intake and weight gain velocity on body fat mass at 6 months of age: the EU childhood obesity programme. Int J Obes (Lond). 36(4):548–553.
- Galea S, Tracy M. 2007. Participation rates in epidemiologic studies. Ann Epidemiol. 17(9):643–653.
- Goetz AR, Mara CA, Stark LJ. 2018. Greater breastfeeding in early infancy is associated with slower weight gain among high birth weight infants. J Pediatr. 201:27–33.e4).
- Gunther AL, Buyken AE, Kroke A. 2006. The influence of habitual protein intake in early childhood on BMI and age at adiposity rebound: results from the DONALD study. Int J Obes (Lond). 30(7):1072–1079.
- Ibanez L, Ong K, Dunger DB, de Zegher F. 2006. Early development of adiposity and insulin resistance after catch-up weight gain in small-for-gestational-age children. J Clin Endocrinol Metab. 91(6):2153–2158.
- Iguacel I, Escartin L, Fernandez-Alvira JM, Iglesia I, Labayen I, Moreno LA, Samper MP, Rodriguez G. 2018. Early life risk factors and their cumulative effects as predictors of overweight in Spanish children. Int J Public Health. 63(4):501–512.
- Li R, Magadia J, Fein SB, Grummer-Strawn LM. 2012. Risk of bottle-feeding for rapid weight gain during the first year of life. Arch Pediatr Adolesc Med. 166(5):431–436.
- Luque V, Closa-Monasterolo R, Escribano J, Ferré N. 2015. Early programming by protein intake: the effect of protein on adiposity development and the growth and functionality of vital organs. Nutr Metab Insights. 8:49–56.
- Luque V, Escribano J, Mendez-Riera G, Schiess S, Koletzko B, Verduci E, Stolarcyk A, Martin F, Closa-Monasterolo R. 2013. Methodological approaches for dietary intake assessment in formula-fed infants. J Pediatr Gastroenterol Nutr. 56(3):320–327.
- Martin FP, Moco S, Montoliu I, Collino S, Da Silva L, Rezzi S, Prieto R, Kussmann M, Inostroza J, Steenhout P. 2014. Impact of breast-feeding and high- and low-protein formula on the metabolism and growth of infants from overweight and obese mothers. Pediatr Res. 75(4):535–543.
- Mihrshahi S, Battistutta D, Magarey A, Daniels LA. 2011. Determinants of rapid weight gain during infancy: baseline results from the NOURISH randomised controlled trial. BMC Pediatr. 11:99.
- Nanri H, Shirasawa T, Ochiai H, Nomoto S, Hoshino H, Kokaze A. 2017. Rapid weight gain during infancy and early childhood is related to higher anthropometric measurements in preadolescence. Child Care Health Dev. 43(3):435–440.
- Ohlund I, Hernell O, Hornell A, Stenlund H, Lind T. 2010. BMI at 4 years of age is associated with previous and current protein intake and with paternal BMI. Eur J Clin Nutr. 64(2):138–145.
- Ong KK. 2007. Catch-up growth in small for gestational age babies: good or bad? Curr Opin Endocrinol Diabetes Obes. 14(1):30–34.
- Ong KK, Loos RJ. 2006. Rapid infancy weight gain and subsequent obesity: systematic reviews and hopeful suggestions. Acta Paediatr. 95(8):904–908.
- Robinson SM, Crozier SR, Harvey NC, Barton BD, Law CM, Godfrey KM, Cooper C, Inskip HM. 2015. Modifiable early-life risk factors for childhood adiposity and overweight: an analysis of their combined impact and potential for prevention. Am J Clin Nutr. 101(2):368–375.
- Schack-Nielsen L, Michaelsen KF. 2007. Advances in our understanding of the biology of human milk and its effects on the offspring. J Nutr. 137(2):503s–10s.
- UNESCO Institute for Statistics (1997). International standard classification of education (ISCED). Montreal (QC) 2006.
- Weng SF, Redsell SA, Swift JA, Yang M, Glazebrook CP. 2012. Systematic review and meta-analyses of risk factors for childhood overweight identifiable during infancy. Arch Dis Child. 97(12):1019–1026.
- [WHO] World Health Organization. 2006. The WHO child growth standards.
- [WHO] World Health Organization. 2018. Childhood obesity surveillance initiative highlights 2015-17 preliminary data. http://www.euro.who.int/__data/assets/pdf_file/0006/372426/wh14-cosi-factsheets-eng.pdf?ua=1.
- [WHO] World Health Organization. 2018. Exclusive breastfeeding for optimal growth, development and health of infants. [updated 2018 Mar]. http://www.who.int/elena/titles/exclusive_breastfeeding/en/.
- [WHO] World Health Organization. WHO Multicentre Growth Reference Study Group. 2006. WHO child growth standards: length/height-for-age, weightforage, weight-for-length, weight-for-height and body mass index-for-age: methods and development. Geneve.
- Zheng M, Lamb KE, Grimes C, Laws R, Bolton K, Ong KK, Campbell K. 2018. Rapid weight gain during infancy and subsequent adiposity: a systematic review and meta-analysis of evidence. Obes Rev. 19(3):321–332.
- Ziegler EE. 2006. Growth of breast-fed and formula-fed infants. Nestle Nutr Workshop Ser Pediatr Program. 58:51–59; discussion 9–63.