
Abstract
Background: HIV infection and prolonged use of antiretroviral therapy (ART) can impact the body composition and muscle strength of HIV-infected children and adolescents. Therefore, the aim was to verify the association between lean soft tissue mass (LSTM) and handgrip strength (HGS) in children and adolescents diagnosed with HIV using or not using ART (with or without protease inhibitors [PI]).
Method: Cross-sectional study with 65 children and adolescents diagnosed with HIV aged 8–15 years of both sexes. LSTM was obtained through dual X-ray absorptiometry (DXA) and HGS using hydraulic dynamometer. Information on viral load, CD4+ T lymphocytes and type of ART (with or without [PI]) were obtained from medical records. Simple and multiple linear regression (adjusted for viral load and CD4+ T lymphocytes) was used, with p < 0.05.
Results: For children and adolescents diagnosed with HIV using ART without PI, the model (LSTM, viral load and CD4+ T lymphocytes) explained 68% of HGS variability. For group with ART and PI, the model explained 73%. For group that did not use ART, the model was not associated with HGS.
Conclusion: The magnitude of the association between LSTM and HGS was greater than in children and adolescents using ART with PI.
It is recognized that in the long-term antiretroviral drugs can negatively impact the body composition of children and adolescents diagnosed with HIV. However, few studies have investigated the short-term impact of drug use.
The use of antiretroviral therapy (ART) with protease inhibitor (PI) increased the explanatory power of lean soft tissue mass with muscle strength in children and adolescents diagnosed with HIV.
These results demonstrate the importance of antiretroviral drugs in the short term. Further studies are needed to identify how and when interventions are needed to reduce the negative effects of drugs in the long term.
Impact
Keywords:
Introduction
The advent of antiretroviral drugs (ART) enabled an increase in life expectancyCitation1 and an increase in body mass and height, although not enough to reach the average values of the general population. However, ART can bring adverse health effects, especially in the long term. To inhibit HIV replication, it is used the combination of at least three antiretroviral drugs, two drugs of different classes, which can be combined into a single pill.Citation2 The ‘catch-up growth’ may depend on age at the beginning of treatment, nutritional status, adherence to treatment, immunological status, clinical stage, sex, type of ART and opportunistic infections.Citation3
Of the classes of drugs is the class of protease inhibitors (PI), which act on the protease enzyme, blocking its action and preventing the production of new copies of HIV-infected cells.Citation2 The PI class was associated with deleterious health effects in adolescents diagnosed with HIV, in which 10% of adolescents who received PI had metabolic syndrome, 20% had two or more characteristics of the metabolic syndrome without obesity and 70% had any form of dyslipidemia.Citation4
A longitudinal study conducted with adults diagnosed with HIV identified marked loss of fat-free mass associated with the use of ART (class of nucleoside reverse transcriptase inhibitors and integrase inhibitors).Citation5 However, the study found no differences among ART classes and did not investigate PI.Citation5 In the pediatric population diagnosed with HIV, a study identified low fat-free mass associated with viral replication; however, it did not carry out analyses stratified by the type of medication used.Citation6 Previous studies have identified improvements in muscle reserve after the use of ART in children and adolescents.Citation7,Citation8 Studies have described that the increase in muscle reserve could be related to the decrease in viral load and increase in CD4+ T lymphocytes due to the use of ART.Citation8,Citation9 However, a large part of literature investigated specific components of physical growth, such as body mass, height, fat mass and fat-free mass,Citation10,Citation11 with little literature on the lean soft tissue mass (LSTM), the component closest to skeletal muscle mass.Citation12
Loss of LSTM was associated with lower handgrip strength (HGS) levels and increased mortality in adults diagnosed with HIV.Citation12 Muscle strength is closely related to the absolute amount of muscle mass and integrity of the nervous system.Citation13 However, assessing muscle mass is a complex task, and LSTM is often assessed. HGS decreases in individuals diagnosed with HIV, resulting in impaired locomotor function, deterioration of functional capacity and limitations in activities of the daily living.Citation14 Impaired neuromuscular function was also associated with restrictions on participation in physical activities and sports.Citation15 A systematic review identified that children and adolescents diagnosed with HIV had lower HGS levels compared to children and adolescents without the diagnosis.Citation16 Therefore, it is suggested that HIV infection and the use or not of ART can negatively impact the development of HGS. Given the above, the aim of this study was to verify the association between HGS and LSTM in children and adolescents diagnosed with HIV using ART or not.
Method
This is a cross-sectional study conducted with children and adolescents diagnosed with HIV. This study complied with ethical precepts, with approval (protocol No. 49691815.0.0000.0121). The informed consent form was signed by parents or legal guardians and the assent form by children and adolescents.
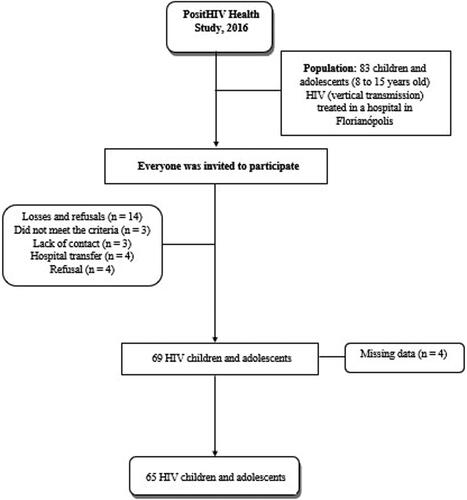
Inclusion criteria were (1) medical record of HIV infection by vertical transmission; (2) age between 8 and 15 years; (3) clinical and laboratory information available in the medical record and (4) able to stand and communicate. Exclusion criteria were (1) motor impairment or contraindication for vigorous exercise; impaired speech, hearing and/or cognition; (2) diseases that change body composition, with the exception of HIV infection and (4) regular use of diuretic drugs or immunotherapies. Information regarding type of study, population and sample is highlighted in .
Figure 1. Flowchart of participants in the PositHIV Health Study.
Sample calculation
Sample size was calculated a posteriori considering type I error (α = 0.05) and type II error (β = 0.80).Citation17 For multiple linear regression analysis, the posteriori analysis indicated that with α = 0.05 and β = 0.80, the sample composed of 65 children and adolescents enabled finding association between LSTM and muscle strength with average effect size of 0.50.Citation17 All calculations were performed using G * Power® software version 3.1.9.2 (Universitat Dusselfodorf, Germany).
Data collection procedures
Data collection was carried out in the second half of 2015 (August to November). Graduate Physical Education and Nutrition students acted as evaluators with full availability to perform fieldwork. The selection and training of the team was carried out by the study coordinator in order to standardize evaluation procedures.Citation18
Dependent variable
HGS was measured using Saehan® hydraulic dynamometer (Model SH5001, Saehan Corporation, Masan, Korea). Evaluation procedures followed protocol described by the Canadian Society for Exercise Physiology.Citation19 Briefly, during evaluation, participants were instructed to stand with arms extended on their sides, without the equipment touching their thigh. The equipment was located between the distal phalanges and the palm.Citation19 Subsequently, inspiration and maximum expiration were requested, followed by the greatest pressure with the hand on the equipment. The test was performed on both hands alternately twice, and the best strength result in kilograms [kilogram-force (Kg/f)] for each hand was recorded and added up, obtaining the total strength.
Independent variable
LSTM was obtained using dual X-ray emission absorptiometry (DXA), Lunar Prodigy Advance equipment, model Discovery Wi Fan-Beam - S/N 81593, (GE®, Medical Systems, Madison, USA), and analyzed in kilograms (Kg). The attenuation of X-rays in body tissues was computed by Encore 2004 software, version 8.10.027 (GE® Lunar Corporation, Madison, WI, USA). Monthly, weekly and daily calibrations were performed to ensure quality control. A previously trained researcher performed evaluations according to standardized procedures.Citation20 During evaluations, participants were wearing appropriate clothing, barefoot, without the use of earrings and/or rings. DXA measures the amount of bone mass in the body by means of algorithms generated by X-ray beams that pass through the body. When measuring bone mass, it distinguishes bones from adipose tissue and fat-free mass, and when subtracting these components, LSTM is estimated.Citation20
Characterization and stratification variables
Chronological age was obtained through self-administered questionnaire. Body mass and height were measured using the International Society for the Advancement of Kinanthropometry (ISAK) protocol. Body mass was measured with portable digital scale (Tanita®, 180 Tokyo, Japan), with maximum capacity of up to 150 kg and resolution of 0.1 kg. Height was measured using stadiometer (Altura Exata®, 77 182 Belo Horizonte, Brazil), with capacity from 115 cm to 210 cm and resolution of 0.1 cm. All measurements were performed by a single ISAK level 1 researcher. The intra-evaluator technical measure error (TME) was carried out with 32 children and adolescents of the same age group as in the present study and all measures resulted in adequate TME values.Citation21 ART was used as a stratification variable and categorized as not using ART and using ART (with or without protease inhibitors [drug class]) and obtained from the medical records of each participant.
Confounders variables
Information regarding HIV viral load (on a log basis) and amount of CD4+ T lymphocytes were obtained from the medical records of each participant in the last three years and averaged. Sex and age were obtained through an interview.
Statistical treatment
First, descriptive analysis (median and interquartile range) was performed, and then observations that presented some missing information were excluded. Kurtosis and asymmetry were used to verify data normality (range between −2 and + 2), in addition to the analysis of histograms to identify data normality distribution. After verifying data normality, analysis of variance (ANOVA) was used with the Bonferroni post-hoc test to compare groups.
Subsequently, Pearson's linear correlation and simple and multiple linear regression were used to test the correlation and association between outcome and exposure, respectively. For multiple linear regression, four models were built: model crude; model I: viral load of the last three years, model II: viral load of the last three years and CD4+ T lymphocytes of the last three years; model III viral load of the last three years, CD4+ T lymphocyte of the last three years and sex and model IV: viral load of the last three years and CD4+ T lymphocyte, sex and age.
Regression coefficients (β), 95% confidence intervals and determination coefficient were estimated for each model analyzed (R2), multicollinearity diagnosis (VIF), and the Cohen’DCitation17 effect size was calculated. For all analyses, the STATA software (Statistical Software for Professionals, Texas, USA), version 14.0, was used, adopting p ≤ 0.05.
Results
The study included 65 children and adolescents diagnosed with HIV and mean age of 12.14 years (± 1.95). Almost 70% of participants had undetectable viral load (<40 thousand copies.mL−1) and 16% (n = 11) did not use ART. Among those who did not use ART, two patients abandoned treatment, one had late diagnosis and eight did not present clinical, immunological and virological criteria for introduction of ART.
Children and adolescents who did not use ART had higher viral load when compared to those using ART with or without PI. Children and adolescents who used ART with PI had higher CD4+ T cells of the last three years compared to those who did not use ART ().
Table 1. Characteristics of children and adolescents diagnosed with HIV+.
Analyses showed a direct association between LSTM and handgrip strength for both groups (ART without PI, ART with PI and without ART). For children and adolescents with HIV using ART without PI, LSTM explained 74% of HGS variability, in which the increase of 1.10 kg in LSTM increased by 1.0 kg/f HGS. In model IV (adjusted for viral load of the last three years, CD4+ T lymphocytes of the last three years, sex and age), the explanatory power was 68%. In the group with ART and PI, the increase of 0.98 kg in LSTM would increase by 1.0 kg/f HGS. The explanatory power in models adjusted (IV) was 73% ().
Table 2. Simple and multiple linear regression between muscle strength and lean soft tissue mass and bone mass in children in adolescents diagnosed with HIV.
For children and adolescents with HIV who did not use ART, LSTM explained 54% of handgrip strength variability, in which the increase of 0.68 kg in LSTM increased by 1.0 kg/f HGS. When inserting adjustment variables (Model III and IV), the association between LSTM and HGS statistically disappeared ().
Discussion
The main results of this research were that the magnitude of the association between HGS and LSTM was greater in children and adolescents using ART with PI compared to those using ART without PI. A possible justification for results found may be related to the immunological condition of children and adolescents diagnosed with HIV using ART with PI,Citation22 which in the present study had lower viral load and greater amount of CD4+ T lymphocytes, indicating better health status. The count of CD4+ T lymphocytes quantifies the degree of infection immunosuppression and demonstrates the risk of opportunistic diseases, in addition to being one of the most important factors to indicate the drug regimen that should be used.Citation23
The class of drugs with PI was associated with abnormal glucose metabolism by inhibiting GLUT4, a glucose transporter, which results in decreased glucose transport to muscle and adipose tissue in adults diagnosed with HIV. However, in the present study, no differences in LSTM and HGS of children and adolescents diagnosed with HIV using ART with or without PI or not using ART were observed. Although the start of ART use is associated with increase in fat-free mass, a longitudinal study with adults diagnosed with HIV identified that the loss of fat-free mass was associated with longer exposure to the virus and ART, not with the type of medication used.Citation5
Regarding HGS, one study did not identify differences between those using ART or not; however, the authors found that HGS was lower in adults with low CD4+ T lymphocyte count.Citation24 Studies have identified that long-term ART can have a negative impact on different health outcomes, such as the pattern of body composition distribution, dyslipidemia, muscle strength and metabolic syndrome.Citation16,Citation25 However, other studies have observed that after the use of ART, physical growth and gross and fine motor capacity of HIV-infected children and adolescents was within the normal range for children and adolescents without diagnosis of HIV.Citation26 Therefore, it appears that ART can positively impact growth, development and physical function; however, side effects can have a negative influence, depending on the health outcome, time of exposure to the virus and drug regimens.
This study has limitations such as the sample heterogeneity due to the age group variability. The wide variability in age (8–15 years) indicates that there is great difference in the time of exposure to the virus and to medication regimens. Research conducted with 80 adolescents found that patients with long exposure to ART with PI were 1.04 times more likely of developing metabolic syndrome.Citation4 The variability of the patients' clinical condition is also considered a study limitation that might have impacted results. A study with children identified that viral load is a predictor of fat-free mass.Citation6 The lack of information about other ART classes is another study limitation. Studies comparing the other classes of drugs are necessary in order to identify which drug regimens may be less harmful to LSTM and HGS of children and adolescents diagnosed with HIV.
This research also has strengths, which should be highlighted, such as the instrument used to measure body composition, which is more accurate when compared to other techniques for measuring body composition, in addition to the representativeness of pediatric patients in the researched region (78% of HIV-infected children and adolescents treated at the reference hospital). Models adjusted for viral load and CD4 + T lymphocytes can also be considered a strong point, given the impact of these parameters on LSTM and HGS.
It could be concluded that there is a direct association between LSTM and HGS in HIV-infected children and adolescents. In addition, the magnitude of the association was greater for children and adolescents using ART with PI compared to those using ART without PI.
Disclosure statement
No potential conflict of interest was reported by the authors.
Funding
The author(s) reported there is no funding associated with the work featured in this article.
References
- Gortmaker SL, Hughes M, Cervia J, et al. Effect of combination therapy including protease inhibitors on mortality among children and adolescents infected with HIV-1. N Engl J Med. 2001;345(21):1522–1528.
- Almeida FJ, Kochi C, Sáfadi MAP, et al. Influence of the antiretroviral therapy on the growth pattern of children and adolescents living with HIV/AIDS. J Pediatric. 2019;95:95–101.
- Boletim Epidemiológico - HIV Aids. Departamento de Vigilância, P. E. C. D. I. S. T.: Secretaria de Vigilância em Saúde 2018.
- Santiprabhob J, Tanchaweng S, Maturapat S, et al. Metabolic disorders in HIV-infected adolescents receiving protease inhibitors. Biomed Res Int. 2017;2017:7481597.
- Debroy P, Lake JE, Sim M, the Modena HIV Metabolic Cohort Team, et al. Lean mass declines consistently over 10 years in people living with HIV on antiretroviral therapy, with patterns differing by sex. Antivir Ther. 2019;24(5):383–387.
- Arpadi SM, Cuff PA, Kotler DP, et al. Growth velocity, fat-free mass and energy intake are inversely related to viral load in HIV-infected children. J Nutr. 2000;130(10):2498–2502.
- Miller TL, Mawn BE, Orav EJ, et al. The effect of protease inhibitor therapy on growth and body composition in human immunodeficiency virus type 1-infected children. Pediatrics 2001;107(5):E77–77.
- Chantry CJ, Cervia JS, Hughes MD, PACTG 1010 Team, et al. Predictors of growth and body composition in HIV-infected children beginning or changing antiretroviral therapy . HIV Med. 2010;11(9):573–583.
- Kim RJ, Rutstein RM. Impact of antiretroviral therapy on growth, body composition and metabolism in pediatric HIV patients. Paediatr Drugs. 2010;12(3):187–199.
- Golucci APBS, Marson FAL, Valente MFF, et al. Influence of AIDS antiretroviral therapy on the growth pattern. J Pediatr (Rio J). 2019;95(1):7–17.
- Grant PM, Kitch D, McComsey GA, et al. Long-term body composition changes in antiretroviral-treated HIV-infected individuals. Aids. 2016;30(18):2805–2813.
- Erlandson KM, et al. Functional impairment is associated with low bone and muscle mass among persons aging with HIV-infection. J Acquir Immune Defic Syndr. 2013;3:209.
- Ogunrin AO, Odiase FE, Ogunniyi A. Reaction time in patients with HIV/AIDS and correlation with CD4 count: a casecontrol study. Trans R Soc Trop Med Hyg. 2007;101(5):517–522.
- Gomes-Neto M, Rodriguez I, Lédo AP, et al. Muscle strength and aerobic capacity in HIV-infected patients: a systematic review and meta-analysis. J Acquir Immune Defic Syndr. 2018;79(4):491–500.
- García-Hermoso A, Ramírez-Campillo R, Izquierdo M. Is muscular fitness associated with future health benefits in children and adolescents? A systematic review and meta-analysis of longitudinal studies. Sports Med. 2019;49(7):1079–1016.
- Macdonald V, Verster A, Baggaley R, et al. A call for differentiated approaches to delivering HIV services to key populations. J Int AIDS Soc. 2017;20(Suppl 4):21658.
- Cohen J. The effect size index: d. Statistical power analysis for the behavioral. Sciences 1988;2:284–288.
- de Lima LRA, Silva DAS, da Silva KS, et al. Aerobic fitness and moderate to vigorous physical activity in children and adolescents living with HIV. Pediatr Exer Sci. 2017;29(3):377–387.
- Canadian Society for Exercise Physiology. The Canadian Physical Activity, Fitness and Lifestyle Appraisal: CSEP's guide to health active living. 2003.
- Crabtree NJ, Kibirige MS, Fordham JN, et al. The relationship between lean body mass and bone mineral content in paediatric health and disease. Bone 2004;35(4):965–972.
- Pederson D, Gore C. Erros de Medição em Antropometria. Artmed: Kevin 412 N, Tim O. Antropométrica. Porto Alegre, 2005.
- Jacobson DL, Lindsey JC, Coull BA, et al. The association of fat and lean tissue with whole body and spine bone mineral density is modified by HIV status and sex in children and youth. Pediatr Infectious Disease J. 2018;37(1):71–77.
- Ford N, Meintjes G, Vitoria M, et al. The evolving role of CD4 cell counts in HIV care. Curr Opin HIV Aids. 2017;12(2):123–128. 2017.
- Raso V, Shephard RJ, Casseb JS, et al. Aerobic power and muscle strength of individuals living with HIV/AIDS. J Sports Med Phys Fitness. 2014;54(1):100–107.
- Espiau M, Yeste D, Noguera-Julian A, et al. Adiponectin, leptin and inflammatory markers in HIV-associated metabolic syndrome in children and adolescents. Pediatr Infect Dis J. 2017;36(2):e31–e37. 2017.
- Shariat M, et al. Growth and Neurodevelopmental Status in HIV Infected Children. Iranian J Pediatr. 2017; 27:e9406.