
Abstract
Diarrhoea is the second-leading cause of death in Liberia, a sub-Saharan African country of 4.8 million people, with a majority living in rural villages. Diarrhoea has often been linked with poor water quality and malnutrition. Three organisations partnered to distribute point-of-use (POU) water filters to every household in Liberia without other access to safe water, documenting the distribution of filters to 101,706 households. Each such household was surveyed at a baseline, two weeks, and eight weeks. In addition to household characteristics, the prevalence of diarrhoea was reported at each survey. Our goal was to determine the extent of the impact that POU filter use had on diarrhoea prevalence by age group, controlling for effects of water source, location, and household size. Overall, there was a 94.2% decrease in diarrhoea cases from baseline to the 8-week follow-up. We discuss the success of the intervention in decreasing diarrhoea prevalence. The filter distribution focused on reaching remote villages, and providing access to clean water where there was none before. This study confirms that community-wide access to clean drinking water can reduce diarrhoea prevalence.
Keywords:
1. Introduction
Lack of access to clean drinking water continues to imperil health globally. The sixth of the United Nations’ Sustainable Development Goals (SDG) seeks to ensure the availability and sustainable management of water and sanitation for all (United Nations, Citation2021). As of 2017, 71% of the global population had access to safe drinking water, and an additional 19% had access to basic drinking water; however, this still leaves 10% of the population, or 785 million people, without access to basic drinking water (World Health Organization, Citation2019). In Liberia, as of 2020, 25% of the total population lacked access to basic drinking water; the disparity was greater in rural areas where 36% lacked access compared to 14% in urban areas (WHO/UNICEF Joint Monitoring Programme, Citation2021). As of 2020, only 15% of Liberian households had access to improved water on premises, and the proportion of the population with piped water was less than 4%, a decrease from 6% in 2015 (WHO/UNICEF Joint Monitoring Programme, Citation2021). There is also a lack of access to basic sanitation. Only 18% of Liberians used at least basic sanitation services as of 2020, with access associated with significant wealth inequalities in both urban and rural areas (WHO/UNICEF Joint Monitoring Programme, Citation2021). Furthermore, 38% of the population (and 59% of those in rural areas) practised open defecation (WHO/UNICEF Joint Monitoring Programme, Citation2021).
Global estimates suggest 88% of deaths from diarrhoea can be attributed to unsafe drinking water, inadequate availability of clean water for hygiene purposes, and lack of access to sanitation (Centers for Disease Control and Prevention, Citation2018). Diarrhoea is the second leading cause of death in Liberia following malaria (Centers for Disease Control and Prevention, Citation2019). Diarrhoea is the leading cause of child illness in Liberia, and 8% of deaths among children under the age of 5 can be attributed to diarrhoea (Informational Services et al., Citation2021).
Repeated diarrhoeal infections lead to several deleterious short-term and long-term health outcomes, particularly among young children. Diarrhoea is associated with acute dehydration and malnutrition, which are correlated with loss of height for age (Ajjampur et al., Citation2011; Pavlinac et al., Citation2018; Richard et al., Citation2013). Acute dehydration and malnutrition can result in deficiencies in long-term growth and height in children, and also in cognitive and social development (Lorntz et al., Citation2006; Oriá et al., Citation2016; Pinkerton et al., Citation2016; Tarleton et al., Citation2006). Furthermore, when children experience repeated enteric infections associated with diarrhoea, they are at increased risk for obesity (Guerrant et al., Citation2013), cardiovascular disease (DeBoer et al., Citation2012), and type-2 diabetes (DeBoer et al., Citation2012).
Previous work has compared piped-water and POU filter interventions to identify the most effective methods for providing widespread access to basic drinking water in low- and middle-income countries. In a systematic review of water interventions, Wolf et al. (Citation2014) demonstrated that high-quality piped water provided the largest protective effect on diarrhoeal disease. A Cochrane Review of water quality interventions demonstrated evidence to show that POU filtration systems reduce diarrhoea by about half (Clasen et al., Citation2015). Komarulzaman et al. (Citation2017) asserted that piped water, particularly when paired with high coverage of health facilities, was most effective in reducing diarrhoeal rates in Indonesia, while POU water treatment was not associated with reduction in diarrhoeal disease, potentially due to poor storage methods. However, in various household studies, filter interventions—particularly those paired with safe storage—were associated with large reductions in diarrhoeal disease (Lindquist et al., Citation2014; Raimann et al., Citation2019; Tintle et al., Citation2019; Wolf et al., Citation2014).
Previous studies of interventions using Sawyer PointONE POU filters have demonstrated significant decreases in diarrhoeal diseases and death (Lindquist et al., Citation2014; Tintle et al., Citation2021). In a cluster randomised controlled trial of 1,196 Bolivian households, Lindquist et al. (Citation2014) found an 85% mean reduction in diarrhoeal disease in children under 5 in households receiving the filter and a 78% mean reduction in diarrhoeal disease among children under the age of 5 who were in households that received a filter along with a WASH intervention. Among 503 households in Fiji who received a Sawyer filter, Tintle et al. (Citation2019) demonstrated a decrease in household diarrhoeal prevalence from 17.5% at time of installation to 1.8% at the two-week follow-up. In a similar study of 675 households in the Dominican Republic, Tintle et al. (Citation2021) demonstrated a household reduction of prevalence of diarrhoea from 25.6% at installation to 9.8% at follow-up, which occurred between 7 and 200 days post-intervention.
The sustainability and effectiveness of POU technologies vary. Compared to other POU technologies, POU water filters are more effective and are more likely to last over time (Albert et al., Citation2010; Kirby et al., Citation2019; Sobsey et al., Citation2008). For instance, in a large-scale distribution of household water filters in Rwanda, 75% of filters were in use after four months and 66% after one year (Kirby et al., Citation2019). Additionally, according to Pooi and Ng (Citation2018), despite higher initial costs of membrane filtration systems, their higher flow rate paired with longer estimated lifespan results in a lower cost-per-litre of water. Further, some evidence shows that POU filter interventions are preferred by households as compared to other technologies (Albert et al., Citation2010; Ogunyoku et al., Citation2011). In a study in rural Kenya, households were given dilute hypochlorite solution, porous ceramic filtration, and combined flocculent-disinfection mixture. Households were more likely to use ceramic filtration and dilute hypochlorite solution; the households preferred filtration over the other technologies (Albert et al., Citation2010). For some, the appearance of clear water after using water filters might contribute to their continued use as some see it as a visual indicator of the water being clean (Kirby et al., Citation2019; Lindquist et al., Citation2014).
There are certainly promising aspects of POU technology. They are inexpensive to install and can reach urban areas easier than piped water infrastructures. Since they are transportable, they can easily move with people and are easily distributed. Economically speaking, POU technology is the most cost-efficient, as piped water comes at a significant initial cost for installation and then ongoing costs to community members (such as water bills) (Nauges & Whittington, Citation2017). POU technology is also able to accommodate population growth and potentially stimulate the local economy if the technology can be produced by the community (Ren et al., Citation2013).
This study was conducted to assess the health effects of a large-scale water filtration intervention in the country of Liberia. Our sample, with filter distribution across all of Liberia, allows us to verify whether or not diarrhoeal reductions previously associated with POU filters in smaller and more-controlled settings are robust to the challenges posed by large-scale implementation across a broad and logistically challenging region. This study aims to measure potential diarrhoeal reductions after filter distribution, both overall and among specific age groups.
2. Materials and methods
2.1. Study settings and materials
The study site was the country of Liberia. This study is part of a larger intervention seeking to ensure the entire country of Liberia has access to basic drinking water within a 15-minute walk of their residence by December 2020. The lead NGO, The Last Well, along with several partnering organisations, conducted an extensive water needs assessment of the entire country of Liberia beginning in 2016. Most villages with over 200 households that lacked access to basic clean water were scheduled for well installations; villages with fewer than 200 households and villages too remote for well installation were scheduled for household-level distribution of POU filters. In these villages, each household received a filter, a bucket, and instruction in their use.
The Sawyer PointONE filter utilises gravity filtration and hollow fibre membranes, along with U-shaped micro fibres and pore sizes that do not exceed 0.1 microns (“Water Filters,”, Citationn.d.). The filter removes bacteria, protozoa, sediment, and other contaminants. The filter system is easy to use: the filter is attached to a large bucket, unfiltered water is poured into the bucket, and water flows through the hose and filter into a clean, sealed container. The system can filter a maximum of 1.4 l per minute, and, if cared for properly, can function for up to 10 years (“Water Filters,”, Citationn.d.).
2.2. Study design
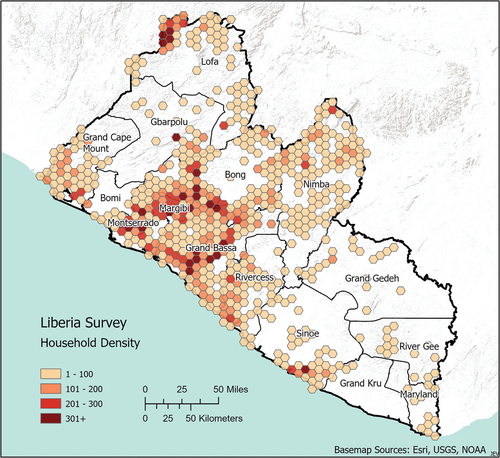
This study contains data gathered from November of 2017 through December of 2020 of 15,679 households receiving the PointONE filter, covering 13 of the 15 counties in Liberia (Figure ). An adults over the age of 18 in each participating household was asked to complete a brief verbal survey on behalf of the entire household at installation and at subsequent visits approximately two and eight weeks later. There were no inducements to participate; all households received and could keep their filter regardless of their participation in the survey. Field workers provided instructions and training on the use of the filters upon distribution, repeating such training as needed at subsequent visits. Alford et al. (Citation2022) provide details on filter functionality and user competence at follow-up visits.
Figure 1. Density of households receiving filters and participating in surveys, by geographic region
The survey interviews were conducted by trained Liberians representing the Last Well and other participating faith-based NGOs. The data were collected using electronic tablets and were then uploaded onto cloud storage. The surveys were linked using 6-digit filter codes (each filter provided to a household was labelled with a sticker displaying such a code, to be used as a unique identifier for that filter/household). Geographical coordinates were used to resolve any discrepancies that, which resulted due to duplicate codes or filters where the code stickers were no longer present.
2.3. Survey instruments
The baseline survey instrument included demographic and health variables. Age was grouped into the following categories: under age 5 (infants and young children), ages 5 to 17 (youths), and ages 18 and older (adults). The instrument utilised a more familiar term, running stomach, to capture prevalence of diarrhoea. The presence/absence of running stomach (diarrhoea) in the past 2 weeks was collected per member of the household. The location (district, county), water source (creek, open well, other), and season (wet or dry) were also recorded.
Follow-up surveys also gathered information on proper filter usage and whether the filter was still functioning properly. Filter usage was measured by observation at follow-up visits to determine whether the family was able to demonstrate the proper use of the filter. Filter functioning was based on whether there were any problems with or parts missing from the filter at follow-up visits.
2.4. Statistical methods
Data were processed and analysed using R and RStudio statistical computing software (R Core Team, Citation2021; RStudio Team, Citation2021) using the package glmmTMB (Brooks et al., Citation2017), which allows for efficient fitting of mixed-effects regression models. The dataset for analysis included all households for which data on 2-week prevalence of running stomach and all necessary covariates (County, district, village, household filter ID, water source, season, household size, age group) were available for all three visits (initial filter distribution and two follow-ups). The two-week prevalence of running stomach was modeled using logistic mixed-effects regression models with fixed effects of visit (baseline, 2 weeks, 8 weeks), household-level 2-week prevalence of running stomach at baseline, county, water source, season, age group, and number of people in the household, plus random effects of village nested within district, and household filter ID.
2.5. Ethics
The study was approved by the Calvin University Institutional Review Board (IRB) study approval number 17–016. The data were collected through the Last Well and partnering organisations that only distributed filters and collected data in villages in which the tribal chief had granted permission for the project. Community consent processes through the following of the village protocol and tribal chief permissions were utilised. The individual representing each household received a filter, was trained in its operation and use, and was asked verbally if they would additionally participate in the study.
3. Results
3.1. Study enrollment and participants
Table shows the characteristics of study participants. The study consisted of a total of 15,679 households, with the median household consisting of 6 members. Filters were distributed to 101,706 households, 78091 of which occurred between 27 November 2017 and 20 January 2021, the period being analysed here. To be included in the study, households required (a) survey completions at filter installation (baseline), two-week follow-up, and eight-week follow-up, with no duplicate visits (n = 30,154), that (b) included responses to the aforementioned variables necessary for modelling (n = 15,679). Figure provides a flow chart illustrating how households were selected for inclusion in the analysis presented here.
Figure 2. Flow chart depicting inclusion and exclusion criteria for the analyses in this study
Table 1. Participant characteristics. For total rows, percentages are out of the total sample size. When stratifying by age, water source, county, and household size, percentages are out of the total number of people or households participating at a given time point (baseline, 2 weeks, or 8 weeks)
Over 50% of the participants were 18 years and older, approximately 44% of the participants were ages 5 to 17, and the remaining 6% of participants were under the age of 5; the total number of participants at each timepoint ranged from 100,251 to 105,794 (Table ). The majority of households rely on rivers and creeks for their primary water supply (~80%). Grand Bassa, Bong, and Margibi counties represent most of the households in this study, accounting for 52% of the total households. It should be noted, however, that the dataset is not representative of Liberia as a whole, considering rural populations were more likely to qualify for POU filter distributions than urban populations (Figures ).
Table shows changes in diarrhoeal rates from baseline to 8 weeks by age. The percentage of those experiencing diarrhoea in the last two weeks was reduced significantly among all age groups between distribution of the filters and the two follow-up visits at two weeks and eight weeks. Across all age groups, the decrease in diarrhoeal rates was approximately 94.2% (from about 10.5% to about 0.6%). Adults, youth, and infants/young children showed a decrease in diarrhoeal rates similar to that of the entire population with reductions of 94.6% and 93.6%, and 94.3%, respectively.
Table 2. Changes in diarrhoeal rates from baseline to 8 weeks by age. N is the total number of people, and N_RS is the number of people with running stomach (diarrhoea). The overall change (%) gives percentage change of running stomach prevalence from baseline to eight weeks, computed by subtracting the baseline percentage from the 8-week percentage and then dividing by the baseline percentage (and finally multiplying by 100 to obtain the percent change)
According to the regression model, which also controlled for variation of location, season, water source, and household size, youth diarrhoeal prevalence was comparable to adults (OR 0.97, 95% CI 0.93–1.02), while prevalence in children was slightly higher (OR 1.34, 95% CI 1.22–1.46) (Table ). Diarrhoeal prevalence showed a greater decrease over longer periods of time, with odds ratios for diarrhoea being 0.071 (95% CI 0.066–0.076) and 0.027 (95% CI 0.024–0.029) for 2 and 8 weeks, respectively (Tables ). There were also variations in reported diarrhoeal prevalence by county (Figure ). Grand Cape Mount, Grand Gedeh, and Maryland reported the highest diarrhoeal prevalence at baseline.
Figure 3. Reported diarrhoeal prevalence at the initial visit and at follow-up visits approximately two and eight weeks later
Table 3. Odds of diarrhoea by participant characteristics. This table presents results from the mixed-effects logistic regression model. Base levels for each variable are water source: Creek, County: Bong, timepoint: baseline, season: dry, and age group: adults
4. Discussion
The purpose of this study was to evaluate the health outcomes of a large-scale water filter distribution effort on diarrhoeal rates in Liberia. There were substantial reductions in two-week self-reported diarrhoea prevalence in all age groups, with an overall 94.2% reduction in prevalence of diarrhoea between the receipt of the filter and 8-week follow-up. This percent change is higher than in previous studies, which show reductions in prevalence between 62% and 90% (Kirby et al., Citation2019; Lindquist et al., Citation2014; Tintle et al., Citation2019, Citation2021). However, these variations may be attributed to differences in geographic locations, prevalence of running stomach at installation, and time between follow-up visits, among other things.
POU interventions can only be successful if they are used consistently and correctly. In other settings, even when filters were utilised, they were not used as the primary source of drinking water or were not the only means to drinking water (Fabiszewski de Aceituno et al., Citation2012). Additionally, even when filters are used consistently, storage containers are often contaminated (Kamara et al., Citation2017; Komarulzaman et al., Citation2017; Peletz et al., Citation2013). While the current study did not collect data on the consistency of filter use, a separate analysis of the survey data confirmed that the majority (over 95%) of filters functioned properly and the majority of households (over 90%) could properly demonstrate filtering and backwashing after 8 weeks, indicating some degree of sustainability of the intervention (Alford et al., Citation2022). In order to reinforce compliance and proper use in POU interventions, follow-up visits provide an opportunity for further education and training (Alford et al., Citation2022; Sisson et al., Citation2013).
In a time where there is a global imperative to ensure access to clean drinking water for all, it is essential we identify cost-effective and efficient ways to provide safe drinking water (Bain, Johnston, & Slaymaker, Citation2020). There continue to be disparities in how populations gain access to piped water, often considered the gold standard in the delivery of clean water. The disparity is particularly pronounced along the urban-rural and wealth divides in sub-Saharan Africa (Chitonge et al., Citation2020; Armah et al., Citation2018). Access to clean water is not only critical for population health but also for educational attainment, civic participation, and economic development opportunities (Apeh et al., Citation2020; Burt & Keiru, Citation2011). However, challenges exist both in building and in maintaining the infrastructure to deliver piped water to rural communities. POU filters, or household filters, are more cost-effective than point-of-source methods, such as wells and piped water (Clasen et al., Citation2015). Our results support the use of hollow membrane filter distribution as an effective short-term solution to address water access needs.
Unfortunately, access to clean drinking water alone does not equal health. It is ideal to implement clean water interventions in concert with other water, sanitation, and hygiene (WASH) efforts, including the integration of proper storage of clean water, handwashing practices, and sanitation interventions, as faecal exposure is a major contributor to diarrhoeal disease (Bain, Johnston, & Slaymaker, Citation2020; Dagnew et al., Citation2019; Fabiszewski de Aceituno et al., Citation2012; Jiwani & Antiporta, Citation2020; Kamara et al., Citation2017; Komarulzaman et al., Citation2017; Wolf et al., Citation2014). However, others argue that POU interventions can still be effective in areas where sanitation has not been addressed (Clasen et al., Citation2015).
There is some evidence to suggest that large-scale WASH interventions may result in spillover effects for neighbours, correlated with the size of effects on intervention participants (Benjamin-Chung, Arnold, et al., Citation2018). In a study of WASH benefits in Bangladesh, Benjamin-Chung, Amin, et al. (Citation2018) postulated limited spillover effects due to insufficient intervention coverage and lack of resources for those not included in the intervention arm to engage in behaviour change. While spillover was not explicitly addressed in this study, by providing access to improved water country-wide, our hope is that the positive health effects among those who continue to use the filter will result in a lower prevalence of diarrhoea throughout the country of Liberia.
It is our hope that the results of the USAID Liberia Demographic and Health Surveys before and after the work of the Last Well will demonstrate some of the expected changes in population health following a country-wide clean water intervention. Such results would provide crucial confirmation of our findings, particularly in light of limitations of this study related primarily to the study design. The study lacked a control, or non-intervention arm, preventing the ability to fully analyse change in diarrhoeal rates due to POU filter implementation. Further, we relied on self-report for diarrhoea within households. This can be problematic as the 14-day recall for diarrhoeal rates is too long and self-reports are often influenced by social desirability bias (Melo et al., Citation2007; Rosa et al., Citation2016; Schmidt et al., Citation2007). In order to account for some of this bias, use of secondary data, such as clinic records before and after the intervention can assist with determining true changes. Some survey questions often went unanswered, such as how much was spent on water and how many days of work and school were lost due to diarrhoea. This limited the ability to fully analyse the effects of the filter distribution. Since the intervention served primarily small, remote rural villages these results are not representative of the country as a whole and may not be entirely representative of those households who received filters due to missing covariates and/or follow-up data.
Despite the limitations, this study demonstrates the magnitude of impact that a large scale, border-to-border water project can have on the health of an entire nation. It complements other studies analysing the effectiveness of the POU filter interventions from other parts of the world, further demonstrating the potential for this water technology to be implemented in many regions of the world (Lindquist et al., Citation2014; Tintle et al., Citation2019, Citation2021). Furthermore, this intervention focuses on bringing clean water to entire communities rather than select households, a strategy that others have found to further improve health (Komarulzaman et al., Citation2017).
Acknowledgments
The authors would like to acknowledge other team members and organisations who have contributed to the project: Grace M. Bolt, Rebekah Cross, Yue He, Megumu Jansen, Kyuhyun Jeong, Kate McClain, Hallie Miller, Abbi Stratton, Samuel Zeleke, and Sebrina Zeleke of Calvin University; Darrel Larson of Sawyer Products, Inc.; staff of the Last Well; and all of the organisations and individuals in Liberia, who worked tirelessly to ensure that everyone in their nation has access to clean water.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
The data are not available due to the protection of participant privacy.
Additional information
Funding
Notes on contributors
K. R. Alford
Dr. Kristen Alford is currently a consultant working with the National Association of Chronic Disease Directors. She previously served as an associate professor of public health and social work at Calvin University.
L. K. Walls
Lydia Walls carried out this work during undergraduate studies at Calvin University, while working as a summer research fellow in Public Health.
S. L. DeRuiter
Dr. Stacy DeRuiter is associate professor of Mathematics and Statistics at Calvin University.
R Pruim
Dr. Randall Pruim is a professor of Mathematics and Statistics and co-director of the undergraduate and graduate data science programs at Calvin University.
J. E. VanHorn
Dr. Jason E. VanHorn is a Professor of Geography and expert in GIS, cartography, and remote sensing.
M. Bone
Matthew Bone carried out this work during undergraduate studies at Calvin University, while working as a summer research fellow in Statistics.
J. Deighton
Jared Deighton is a Ph.D. Candidate and Graduate Research Assistant at The University of Tennessee, Knoxville. He studies the intersection between neuroscience and machine learning through the lens of applied mathematics. He carried out this work during his undergraduate studies at Calvin University while working as a summer research fellow in Statistics.
J. Koeman
Jamison Koeman carried out this work during his undergraduate studies at Calvin University, while working as a summer research fellow in Public Health. He is now the program manager of two research initiatives on housing and urban health at the University of Michigan School of Public Health.
S. Kornoelje
Sadie Kornoelje carried out this work during undergraduate studies at Calvin University, while working as a summer research fellow in Statistics.
A. Koroma
Abdul Hafiz Koroma completed this research as part of his work with The Last Well. Currently, Abdul is a Subject Matter Expert with Social Impact in the USAID Human Resources for WASH Assessment in Liberia Project.
R. LeTourneau
Randy LeTourneau had 20+ years working in IT with for-profit companies and has since used his technology experience in serving in several non-profit organizations. Randy was the VP of Field Operations for The Last Well and was responsible for the implementation of the interventions of this study. He later moved to be the Director of Monitoring and Evaluation for The Bucket Ministry. Along with a career in global IT, Randy has traveled to or worked in 32 different countries with extensive ministry in Peru, Ecuador, Colombia, Kenya and Liberia.
B. Lika
Blerta Lika carried out this work during undergraduate studies at Calvin University, while working as a summer research fellow in Statistics.
K. Rosendale
Katherine Rosendale carried out this work during her undergraduate studies at Calvin University, while working as a summer research fellow in public health. She currently works in journalism.
N. Wang
Nathan Wang carried out this work during his Bachelor of Computer Science program at Calvin University, while working as a summer research fellow in the Department of Statistics.
References
- Ajjampur, S. S. R., Koshy, B., Venkataramani, M., Sarkar, R., Joseph, A. A., Jacob, K. S., Ward, H., & Kang, G. (2011). Effect of cryptosporidial and giardial diarrhoea on social maturity, intelligence and physical growth in children in a semi-urban slum in south India. Annals of Tropical Paediatrics, 31(3), 205–13. https://doi.org/10.1179/1465328111Y.0000000003
- Albert, J., Luoto, J., & Levine, D. (2010). End-user preferences for and performance of competing POU water treatment technologies among the rural poor of Kenya. Environmental Science & Technology, 44(12), 4426–4432. https://doi.org/10.1021/es1000566
- Alford, K. R., Rosendale, K. D., Koroma, A. H., DeRuiter, S. L., Pruim, R., VanHorn, J. E., Bone, M., Deighton, J., DenHaan, A., Koeman, J., Kornoelje, S., Lika, B., Stratton, A., Walls, L., & Wang, N. (2022). Evaluating filter functionality and user competence after a hollow fiber membrane filter intervention in Liberia. Journal of Water, Sanitation and Hygiene for Development, 12(12), 851–861. https://doi.org/10.2166/washdev.2022.075
- Apeh, C. C., Onyekuru, A. N., Offorma, J. T., & Akogwu, C. I. (2020). Rural transformation in Liberia: Strategies for civil society participation. International NGO Journal, 15(1), 1–6. https://doi.org/10.5897/INGOJ2018.0332
- Armah, F. A., Ekumah, B., Yawson, D. O., Odoi, J. O., Afitiri, A. -R., & Nyieku, F. E. (2018). Access to improved water and sanitation in sub-Saharan Africa in a quarter century. Heliyon, 4(11), e00931. https://doi.org/10.1016/j.heliyon.2018.e00931
- Bain, R., Johnston, R., & Slaymaker, T. (2020). Drinking water quality and the SDGs. Npj Clean Water, 3(1), 1–3. https://doi.org/10.1038/s41545-020-00085-z
- Benjamin-Chung, J., Amin, N., Ercumen, A., Arnold, B. F., Hubbard, A. E., Unicomb, L., & Colford, J. M., Jr. (2018). A randomized controlled trial to measure spillover effects of a combined water, sanitation, and handwashing intervention in rural Bangladesh. American Journal of Epidemiology, 187(8), 1733–1744. https://doi.org/10.1093/aje/kwy046
- Benjamin-Chung, J., Arnold, B. F., Berger, D., Luby, S. P., Miguel, E., Colford, J. M., Jr., & Hubbard, A. E. (2018). Spillover effects in epidemiology: Parameters, study designs and methodological considerations. International Journal of Epidemiology, 47(1), 332–347. https://doi.org/10.1093/ije/dyx201
- Brooks, M. E., Kristensen, K., van Benthem, K. J., Magnusson, A., Berg, C. W., Nielsen, A., Skaug, H. J., Mächler, M., & Bolker, B. M. (2017). GlmmTMB balances speed and flexibility among packages for zero-inflated generalized linear mixed modeling. The R Journal, 9(2), 378. https://doi.org/10.32614/RJ-2017-066
- Burt, M., & Keiru, B. J. (2011). Strengthening post-conflict peacebuilding through community water-resource management: Case studies from Democratic Republic of Congo, Afghanistan and Liberia. Water International, 36(2), 232–241. https://doi.org/10.1080/02508060.2011.558885
- Centers for Disease Control and Prevention. (2018). Global WASH fast facts. https://www.cdc.gov/healthywater/global/wash_statistics.html
- Centers for Disease Control and Prevention. (2019). Global Health: Liberia. https://www.cdc.gov/globalhealth/countries/liberia/default.htm
- Chitonge, H., Mokoena, A., & Kongo, M. (2020). Water and Sanitation Inequality in Africa: Challenges for SDG 6. In M. Ramutsindela & D. Mickler (Eds.), Africa and the Sustainable Development Goals (pp. 207–218). Springer International Publishing. https://doi.org/10.1007/978-3-030-14857-7_20
- Clasen, T. F., Alexander, K. T., Sinclair, D., Boisson, S., Peletz, R., Chang, H. H., Majorin, F., & Cairncross, S. (2015). Interventions to improve water quality for preventing diarrhoea. Cochrane Database of Systematic Reviews, 2015(10), 10. https://doi.org/10.1002/14651858.CD004794.pub3
- Dagnew, A. B., Tewabe, T., Miskir, Y., Eshetu, T., Kefelegn, W., Zerihun, K., Urgessa, M., & Teka, T. (2019). Prevalence of diarrhea and associated factors among under-five children in Bahir Dar city, Northwest Ethiopia, 2016: A cross-sectional study. BMC Infectious Diseases, 19(1), 417. https://doi.org/10.1186/s12879-019-4030-3
- DeBoer, M. D., Lima, A. A., Oría, R. B., Scharf, R. J., Moore, S. R., Luna, M. A., & Guerrant, R. L. (2012). Early childhood growth failure and the developmental origins of adult disease: Do enteric infections and malnutrition increase risk for the metabolic syndrome? Nutrition Reviews, 70(11), 642–653. https://doi.org/10.1111/j.1753-4887.2012.00543.x
- Fabiszewski de Aceituno, A. M., Stauber, C. E., Walters, A. R., Meza Sanchez, R. E., & Sobsey, M. D. (2012). A randomized controlled trial of the plastic-housing biosand filter and its impact on diarrheal disease in Copan, Honduras. The American Journal of Tropical Medicine and Hygiene, 86(6), 913–921. https://doi.org/10.4269/ajtmh.2012.11-0066
- Guerrant, R. L., DeBoer, M. D., Moore, S. R., Scharf, R. J., & Lima, A. A. M. (2013). The impoverished gut—A triple burden of diarrhoea, stunting and chronic disease. Nature Reviews Gastroenterology & Hepatology, 10(4), 220–229. https://doi.org/10.1038/nrgastro.2012.239
- Jiwani, S. S., & Antiporta, D. A. (2020). Inequalities in access to water and soap matter for the COVID-19 response in sub-Saharan Africa. International Journal for Equity in Health, 19(1), 82. https://doi.org/10.1186/s12939-020-01199-z
- Kamara, J. K., Galukande, M., Maeda, F., Luboga, S., & Renzaho, A. M. N. (2017). Understanding the challenges of improving sanitation and hygiene outcomes in a community based intervention: A cross-sectional study in rural Tanzania. International Journal of Environmental Research and Public Health, 14(6), 602. https://doi.org/10.3390/ijerph14060602
- Kirby, M. A., Nagel, C. L., Rosa, G., Zambrano, L. D., Musafiri, S., Ngirabega, J. D. D., Thomas, E. A., & Clasen, T. (2019). Effects of a large-scale distribution of water filters and natural draft rocket-style cookstoves on diarrhea and acute respiratory infection: A cluster-randomized controlled trial in Western Province, Rwanda. PLoS Medicine, 16(6), e1002812. https://doi.org/10.1371/journal.pmed.1002812
- Komarulzaman, A., Smits, J., & de Jong, E. (2017). Clean water, sanitation and diarrhoea in Indonesia: Effects of household and community factors. Global Public Health, 12(9), 1141–1155. https://doi.org/10.1080/17441692.2015.1127985
- Liberia Institute of Statistics & Geo-Informational Services, Ministry of Health [Liberia], & ICF. (2021). 2019-20 Liberia Demographic and Health Survey.
- Lindquist, E. D., George, C. M., Perin, J., de Calani, K. J. N., Norman, W. R., Davis, T. P., & Perry, H. (2014). A cluster randomized controlled trial to reduce childhood diarrhea using hollow fiber water filter and/or hygiene–sanitation educational interventions. The American Journal of Tropical Medicine and Hygiene, 91(1), 190–197. https://doi.org/10.4269/ajtmh.13-0568
- Lorntz, B., Soares, A. M., Moore, S. R., Pinkerton, R., Gansneder, B., Bovbjerg, V. E., Guyatt, H., Lima, A. M., & Guerrant, R. L. (2006). Early childhood diarrhea predicts impaired school performance. The Pediatric Infectious Disease Journal, 25(6), 513–520. https://doi.org/10.1097/01.inf.0000219524.64448.90
- Melo, M. C. N. D., Taddei, J. A. D. A. C., Diniz-Santos, D. R., May, D. S., Carneiro, N. B., & Silva, L. R. (2007). Incidence of diarrhea: Poor parental recall ability. The Brazilian Journal of Infectious Diseases: An Official Publication of the Brazilian Society of Infectious Diseases, 11(6), 571–579. https://doi.org/10.1590/s1413-86702007000600009
- Nauges, C., & Whittington, D. (2017). Evaluating the performance of alternative municipal water tariff designs: Quantifying the tradeoffs between equity, economic efficiency, and cost recovery. World Development, 91, 125–143. https://doi.org/10.1016/j.worlddev.2016.10.014
- Ogunyoku, T. A., Nover, D. M., McKenzie, E. R., Joshi, G., & Fleenor, W. E. (2011). Point-of-use drinking water treatment in the developing world: Community acceptance, project monitoring and revision. International Journal for Service Learning in Engineering, Humanitarian Engineering and Social Entrepreneurship, 6(1), 14. https://doi.org/10.24908/ijsle.v6i1.3207
- Oriá, R. B., Murray-Kolb, L. E., Scharf, R. J., Pendergast, L. L., Lang, D. R., Kolling, G. L., & Guerrant, R. L. (2016). Early-life enteric infections: Relation between chronic systemic inflammation and poor cognition in children. Nutrition Reviews, 74(6), 374–386. https://doi.org/10.1093/nutrit/nuw008
- Pavlinac, P. B., Brander, R. L., Atlas, H. E., John-Stewart, G. C., Denno, D. M., & Walson, J. L. (2018). Interventions to reduce post-acute consequences of diarrheal disease in children: A systematic review. BMC Public Health, 18(1), 208. https://doi.org/10.1186/s12889-018-5092-7
- Peletz, R., Simuyandi, M., Simunyama, M., Sarenje, K., Kelly, P., & Clasen, T. (2013). Follow-up study to assess the use and performance of household filters in Zambia. The American Journal of Tropical Medicine and Hygiene, 89(6), 1190–1194. https://doi.org/10.4269/ajtmh.13-0054
- Pinkerton, R., Oriá, R. B., Lima, A. A. M., Rogawski, E. T., Oriá, M. O. B., Patrick, P. D., Moore, S. R., Wiseman, B. L., Niehaus, M. D., & Guerrant, R. L. (2016). Early childhood diarrhea predicts cognitive delays in later childhood independently of malnutrition. The American Journal of Tropical Medicine and Hygiene, 95(5), 1004–1010. https://doi.org/10.4269/ajtmh.16-0150
- Pooi, C. K., & Ng, H. Y. (2018). Review of low-cost point-of-use water treatment systems for developing communities. Npj Clean Water, 1(1), 11. https://doi.org/10.1038/s41545-018-0011-0
- Raimann, J. G., Boaheng, J. M., Narh, P., Johnson, S., Donald, L., Zhang, H., Port, F., & Levin, N. W. (2019). Decentralized water purification using novel membrane filtration technology approach to improve community health. https://doi.org/10.20944/preprints201909.0175.v1
- R Core Team. (2021). R: A language and environment for statistical computing. R Foundation for Statistical Computing. https://rstudio.com/
- Ren, D., Colosi, L. M., & Smith, J. A. (2013). Evaluating the sustainability of ceramic filters for point-of-use drinking water treatment. Environmental Science & Technology, 47(19), 11206–11213. https://doi.org/10.1021/es4026084
- Richard, S. A., Black, R. E., Gilman, R. H., Guerrant, R. L., Kang, G., Lanata, C. F., Mølbak, K., Rasmussen, Z. A., Sack, R. B., Valentiner-Branth, P., Checkley, W., & for the Childhood Malnutrition and Infection Network. (2013). Diarrhea in early childhood: Short-term association with weight and long-term association with length. American Journal of Epidemiology, 178(7), 1129–1138. https://doi.org/10.1093/aje/kwt094
- Rosa, G., Kelly, P., & Clasen, T. (2016). Consistency of use and effectiveness of household water treatment practices among urban and rural populations claiming to treat their drinking water at home: A case study in Zambia. The American Journal of Tropical Medicine and Hygiene, 94(2), 445–455. https://doi.org/10.4269/ajtmh.15-0563
- RStudio Team. (2021). RStudio: Integrated Development for R. RStudio, PBC. http://www.rstudio.com/
- Schmidt, W. P., Luby, S. P., Genser, B., Barreto, M. L., & Clasen, T. (2007). Estimating the longitudinal prevalence of diarrhea and other episodic diseases: Continuous versus intermittent surveillance. Epidemiology (Cambridge Mass), 18(5), 537–543. https://doi.org/10.1097/EDE.0b013e318093f3ce
- Sisson, A. J., Wampler, P. J., Rediske, R. R., & Molla, A. R. (2013). An assessment of long-term biosand filter use and sustainability in the Artibonite Valley near Deschapelles, Haiti. Journal of Water, Sanitation and Hygiene for Development, 3(1), 51–60. https://doi.org/10.2166/washdev.2013.092
- Sobsey, M. D., Stauber, C. E., Casanova, L. M., Brown, J. M., & Elliott, M. A. (2008). Point of use household drinking water filtration: A practical, effective solution for providing sustained access to safe drinking water in the developing world. Environmental Science & Technology, 42(12), 4261–4267. https://doi.org/10.1021/es702746n
- Tarleton, J. L., Haque, R., Mondal, D., Shu, J., Farr, B. M., & Petri, W. A. (2006). Cognitive effects of diarrhea, malnutrition, and entamoeba histolytica infection on school age children in Dhaka, Bangladesh. The American Journal of Tropical Medicine and Hygiene, 74(3), 475–481. https://doi.org/10.4269/ajtmh.2006.74.475
- Tintle, N., Heynen, A., Van De Griend, K., Ulrich, R., Ojo, M., Boven, E., Brokus, S., Wade, R., & Best, A. A. (2019). Evaluating the efficacy of point-of-use water filtration units in Fiji. Tropical Medicine and Health, 47(1), 48. https://doi.org/10.1186/s41182-019-0175-4
- Tintle, N., Van De Griend, K., Ulrich, R., Wade, R. D., Baar, T. M., Boven, E., Cooper, C. E. A., Couch, O., Eekhoff, L., Fry, B., Goszkowicz, G. K., Hecksel, M. A., Heynen, A., Laughlin, J. A., Les, S. M., Lombard, T. R., Munson, B. D., Peterson, J. M., Schumann, E., & Best, A. A. (2021). Diarrhea prevalence in a randomized, controlled prospective trial of point-of-use water filters in homes and schools in the Dominican Republic. Tropical Medicine and Health, 49(1), 1. https://doi.org/10.1186/s41182-020-00291-y
- United Nations. (2021). Goal 6: Ensure availability and sustainable management of water and sanitation for all. United Nations Department of Economic and Social Affairs. https://sustainabledevelopment.un.org/sdg6
- Water Filters. (n.d.). Sawyer International. Retrieved July 5, 2021, from https://international.sawyer.com/water-filters/
- WHO/UNICEF Joint Monitoring Programme for Water Supply, Sanitation and Hygiene. (2021). Progress on household drinking water, sanitation and hygiene: 2000-2020. WHO and UNICEF. https://washdata.org/report/jmp-2021-wash-households
- Wolf, J., Prüss-Ustün, A., Cumming, O., Bartram, J., Bonjour, S., Cairncross, S., Clasen, T., Colford, J. M., Curtis, V., De France, J., Fewtrell, L., Freeman, M. C., Gordon, B., Hunter, P. R., Jeandron, A., Johnston, R. B., Mäusezahl, D., Mathers, C., Neira, M., & Higgins, J. P. T. (2014). Systematic review: Assessing the impact of drinking water and sanitation on diarrhoeal disease in low- and middle-income settings: Systematic review and meta-regression. Tropical Medicine & International Health, 19(8), 928–942. https://doi.org/10.1111/tmi.12331
- World Health Organization. (2019, June 14). Drinking water. https://www.who.int/news-room/fact-sheets/detail/drinking-water