Abstract
Objective: To investigate the effect of bracket–ligature combination on the amount of orthodontic space closure over three months.
Design: Randomized clinical trial with three parallel groups.
Setting: A hospital orthodontic department (Chesterfield Royal Hospital, UK).
Participants: Forty-five patients requiring upper first premolar extractions.
Methods: Informed consent was obtained and participants were randomly allocated into one of three groups: (1) conventional pre-adjusted edgewise brackets and elastomeric ligatures; (2) conventional pre-adjusted edgewise brackets and Super Slick® low friction elastomeric ligatures; (3) Damon 3MX® passive self-ligating brackets. Space closure was undertaken on 0·019×0·025-inch stainless steel archwires with nickel–titanium coil springs. Participants were recalled at four weekly intervals. Upper alginate impressions were taken at each visit (maximum three). The primary outcome measure was the mean amount of space closure in a 3-month period.
Results: A one-way ANOVA was undertaken [dependent variable: mean space closure (mm); independent variable: group allocation]. The amount of space closure was very similar between the three groups (1 mm per 28 days); however, there was a wide variation in the rate of space closure between individuals. The differences in the amount of space closure over three months between the three groups was very small and non-significant (P = 0·718).
Conclusion: The hypothesis that reducing friction by modifying the bracket/ligature interface increases the rate of space closure was not supported. The major determinant of orthodontic tooth movement is probably the individual patient response.
Introduction
Proponents of self-ligating brackets suggest that low levels of friction between the archwire and bracket might increase the rate of tooth movement and hence reduce orthodontic treatment times compared with conventional brackets systems.Citation1,Citation2 One stage that might lead to prolonged treatment with fixed appliances is the closure of residual spaces following dental extraction to alleviate crowding or to reduce an increased overjet/overbite. Space closure can be undertaken with looped archwires; however, the introduction of the pre-adjusted edgewise appliance allows the use of sliding mechanics, which is simpler for the patient to maintain, has less potential for gingival trauma and is easier for the orthodontist to institute when compared to the bending of loops. The drawback of sliding mechanics is that it can be hindered by resistance arising from friction, binding, and notching that may contribute to slow tooth movement and prolonged treatment times.
In addition to self-ligating brackets various other products have been developed that claim to reduce static and/or dynamic friction between the bracket/archwire/ligature interfaces and thereby theoretically enable more rapid tooth movements.Citation3,Citation4 Super Slick® elastomeric ligatures have a covalently bonded Metafix coating to reduce friction, but laboratory tests have provided conflicting results.Citation5–Citation7 In contrast, laboratory tests have consistently shown that the friction between self-ligating brackets and archwires is greatly reduced; however, there is currently limited evidence that this is translated into more rapid tooth movement in the clinical environment.Citation8,Citation9
The aim of this clinical study was to investigate the amount of active orthodontic space closure over 3 months with different bracket/ligature combinations. The null hypothesis was that there was no difference in the rate of space closure in patients treated with fixed orthodontic appliances using conventional pre-adjusted edgewise brackets and elastomeric ligatures compared with patients treated with conventional pre-adjusted edgewise brackets and Super Slick® elastomeric ligatures or Damon 3MX® self-ligating brackets.
Participants and methods
The study was a single-blinded, randomized controlled clinical trial of parallel group design. The setting was the Orthodontic Department of Chesterfield Royal Hospital, Calow, United Kingdom from March 2007 to May 2011. The research protocol was approved by Derbyshire Research Ethics Committee (Ref: 06/Q2401/13245, October 2006) and all participants and their parents gave informed written consent to take part. The following inclusion criteria were applied:
Age between 12 and 16 years;
No contraindications to orthodontic treatment;
Treatment required extraction of at least both upper first premolars and space closure;
No requirement for anchorage supplementation.
The following exclusion criteria were applied:
Oral hygiene of insufficient standard for orthodontic treatment;
Missing teeth (other than third molars);
Cleft lip and palate or other craniofacial syndromes;
Patient not willing to participate in a randomized clinical trial.
Potential patients were screened at their first appointment in the Orthodontic Department and those that fulfilled the inclusion criteria were provided with verbal and written information about the study. They were given at least 1 week to consider whether or not to participate. At a subsequent review appointment, written consent was obtained from those who agreed to take part and they were randomly allocated to one of three groups. Randomization was carried out by one researcher not involved in recruiting patients to the study (PEB) using computer-generated random numbers. To ensure equal numbers, randomization was undertaken in three blocks of 3 (one of each group in a random sequence) and 6 (two of each group in a random sequence) and two blocks of 9 (three of each group in a random sequence). The blocks were placed in a random order. The allocations were concealed in consecutively numbered, sealed opaque envelopes, which were not opened until the patient had been enrolled into the study and consent obtained.
Group 1: Conventional brackets and elastomeric ligatures: Patients allocated to this group received conventional pre-adjusted edgewise brackets (American Orthodontics, Bucks, UK; 0·022×0·028-inch; MBT prescription) bonded in both arches and the archwires were retained with conventional elastomeric ligation (American Orthodontics).
Group 2: Conventional brackets and Super Slick® elastomeric ligatures: Patients allocated to this group received conventional pre-adjusted edgewise brackets (American Orthodontics; 0·022×0·028-inch; MBT prescription) bonded in both arches and the archwires were retained with Super Slick® elastomeric ligatures (TP Orthodontics, La Porte, IN, USA).
Group 3: Self-ligating brackets: Patients allocated to this group received Damon 3MX® passive self-ligating brackets (Ormco Corporation, Orange, CA, USA) bonded in both arches.
In all patients, bonded buccal tubes were used instead of molar bands, as it allowed simpler identification of the buccal groove of the first molar. Following extraction of maxillary first premolars, Group 1 and 2 underwent initial alignment with 0·016-inch and 0·018×0·025-inch nickel–titanium archwires prior to placement of a 0·019×0·025-inch rectangular stainless steel archwire. Group 3 received a series of copper nickel–titanium — 0·014-inch, 0·014×0·025-inch, 0·018×0·025-inch Damon archwires (Ormco, Europe) for initial alignment according to the manufacturer’s recommendation, followed by a 0·019×0·025-inch stainless steel working archwire. It was not possible to mask the operator to group allocation.
Prior to space closure, in all participants the 0·019×0·025-inch stainless-steel wires was in situ and passive for at least 6 weeks and the overbite reduced to normal (2–3 mm). Space closure involved en masse movement of the incisors and canines against the premolars and molars using 6 mm nickel–titanium coil springs (American Orthodontics). These were placed on the buccal hook of the first molar and extended to twice their resting length (12 mm). Nickel–titanium closing springs were chosen as several studies have shown that they produce a more consistent rate of space closure with sliding mechanics than elastics.Citation10–Citation12 The springs were secured to a soldered brass hook on the distal of the upper lateral incisor with metal ligatures. The final length of the nickel–titanium coil spring was recorded (). The use of intermaxillary elastics was postponed until the end of the upper space closure stage of treatment.
Figure 1. Standardized activation of nickel–titanium closing spring to approximately twice the resting length (12 mm)
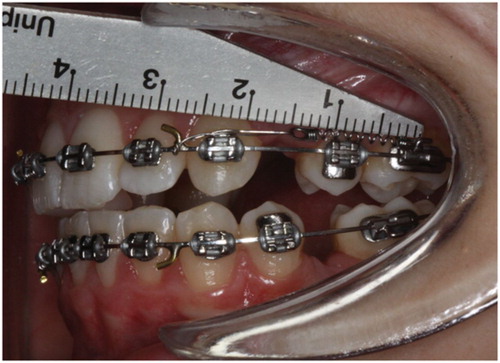
The primary outcome measure was the amount of space closure in millimetres, in both quadrants of the maxillary arch, after 3 months. Once the 0·019×0·025-inch stainless steel archwire had been in situ for at least 6 weeks and before space closure commenced, archwires were removed and alginate impressions of the maxillary arch were taken (T0). The impressions were cast in white stone on-site and within the same day. All patients were recalled at 4 week intervals for 3 months, or until space closure was complete. At each subsequent visit, appliances were assessed for damage, additional maxillary arch impressions were made once the archwire had been removed and the nickel–titanium springs were reactivated to 12 mm. The space closure study was discontinued at the end of 3 months, or one appointment before space closure was complete, to avoid the possibility that the spaces were closed and tooth movement finished before the next adjustment appointment. The aim was to collect four sets of maxillary arch models for each patient (T0–T3) by the end of the trial period.
Prior to measurement the patient details and dates when the study models were taken were masked and each cast was given a randomly generated number by an orthodontist not involved in the study. The size of the two upper arch extraction spaces were measured in the randomly generated order by one operator (HW), who was unaware of the group allocation, using digital callipers and the method described by Dixon et al.Citation10 After 2 weeks, 20 models were randomly selected, recoded in a new random order and the measurements repeated.
An a priori sample size calculation was undertaken based on data from the study by Dixon et al.Citation10 They found a mean difference in space closure between active ligatures and nickel–titanium springs of 0·46 mm/month (SD: 0·86 mm). Using these data, we estimated that a sample size of 13 subjects in each group would be sufficient to detect a difference in the rate of space closure of 3 mm (SD: 2·58) over 3 months, with a power of 90% and significance level of 0·05. To account for a 15% drop-out rate, the sample size was increased to 15 participants per group.
Statistical analysis
Once all the measurements had been undertaken the masking codes were broken and the data entered in a spreadsheet (Excel; Microsoft Corp., Redmond, WA, USA). The size of each remaining extraction space (in mm) measured on the models from time points T1, T2 and T3 was subtracted from the size of the remaining extraction space measured from the same site on the models from the preceding time point (i.e. T1–T0; T2–T1; T3–T2). This figure was then divided by the actual number of days that had elapsed between each study cast to obtain the amount of space closure per day. This was multiplied by 84 (28 days in 4 weeks multiplied by 3) to obtain a standard amount of space closure for each extraction site over three months.
The distribution of the data was examined using the Shapiro–Wilk test and found to be normal (P = 0·753). The repeatability of the measurements was assessed using an intra-class correlation coefficient (ICC) for random error and a paired t test for systematic error.
The null hypothesis that there was no difference between the three groups was tested using a one-way ANOVA. The dependent variable was the standardized amount of space closure over 3 months. The independent variable was group allocation. SPSS Statistics for Windows (v19 SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
Results
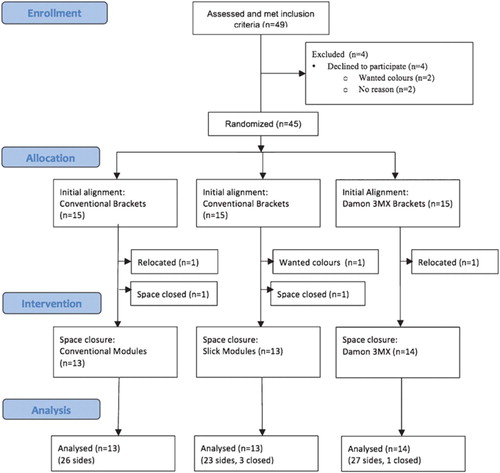
The progression of participants through the trial is shown in . A total of 45 patients were enrolled in the study, of which three were lost to follow-up (two relocated and one withdrew). In two patients, the extraction sites on both sides of the upper arch were closed within one visit and therefore no usable data were gathered. Of the remaining participants, the extraction sites on one side were closed within one visit in four patients, therefore data from only one side was included in the analysis.
Figure 2. CONSORT diagram showing the flow of participants through the trial
The baseline characteristics of the participants are shown in . The mean age at enrolment was 13·9 years (SD: 1 year 10 months), with 23 girls and 17 boys.
Table 1. Baseline characteristics of the three groups of patients.
The repeatability of the space measurements was high with a mean difference between the first and second reading of 0·05 mm (SD: 0·24) and an intraclass correlation coefficient of 0·995, indicating a low level of random error. There was no evidence of systematic error (P = 0·199).
The amount of space closure between the right and left sides of the arch within individuals was examined using a paired t test and no significant difference was found (mean difference was −0·14 mm; SD: 1·22; P = 0·498); therefore, the mean of the two sides was used for hypothesis testing. The descriptive statistics for the standardized amount of space closure in 3 months are shown in . The amounts of space closure were very similar between the three groups and averaged approximately 1 mm/month; however, there was a wide variation in the rate of space closure between individuals from 0·10 mm/month in one participant to 1·80 mm/month in another. The mean differences in space closure after 3 months between the three groups were very small, ranging from 0·1 to 0·3 mm and there was considerable overlap in the confidence intervals for the differences between the groups (). The one-way ANOVA confirmed that the bracket/ligature combination had no significant effect on the amount of space closure over this period (P = 0·718).
Table 2. Descriptive statistics for the standardized amount of space closure in 3 months (mm).
Table 3. One-way ANOVA with a dependent variable of standardized amount of space closure over 3 months and independent variable of bracket/ligature combination. The descriptives are for the differences between groups.
Discussion
This randomized controlled clinical trial did not find any significant differences in the average amount of space closure over 3 months between participants treated using three different bracket–ligature combinations. It would appear therefore, that factors other than bracket–ligature combinations determine the rate of orthodontic space closure.
These findings are consistent with previous prospective clinical trials that have found no differences in the rate of tooth movement between conventional and self-ligating brackets during initial alignment,Citation13–Citation16 en masse space closure using sliding mechanicsCitation17 retraction of upper canine teethCitation18 or overall treatment time in extraction cases.Citation19 Pandis and colleaguesCitation20 did find more rapid alignment when using self-ligating brackets in patients with moderately crowded lower incisors compared to conventional brackets, but in patients with severe crowding there were no differences. Interestingly, BurrowCitation21 concluded that canine retraction was quicker within individuals when using a conventional bracket compared with a self-ligating bracket on the contra-lateral side. Two recent systematic reviews have found no convincing evidence of improved treatment efficiency when self-ligating brackets are used.Citation8,Citation9
The average rate of space closure in this study was 1mm per month, which is very similar to other space closure studies.Citation10,Citation17,Citation18,Citation21,Citation22 Also consistent with other studies was the finding that there was a wide variation in the rates of tooth movement between individual participants. Pilon et al.Citation23 showed that despite all attempts to standardize the delivery of forces to the teeth of beagle dogs, the amount of tooth movement was much more dependent upon individual variation between dogs than on the force levels. They speculate that differences between ‘slow movers’ and ‘fast movers’ are due to variations in bone density, bone metabolism, and in particular turnover of the periodontal ligament, rather than treatment factors, such as force levels or bracket/ligature combinations.
We attempted to standardize the participant appointment intervals to every 4 weeks or 28 days, which is similar to other studies.Citation4,Citation18,Citation20 Unfortunately, it was not possible for all patients to attend exactly every 28 days; therefore an average daily amount of space closure was calculated according to the dates the study models were taken. This was multiplied by 28 to achieve the standardized amount per month, then multiplied by three to find a standardized amount over 3 months. We realize that in clinical practice recall intervals might be longer; however, 4 weeks was chosen because shorter time periods might prove to be a burden to participants and their parents, whereas longer recall intervals might lead to inaccuracies in recording the rate of tooth movement, as the spaces would be completely closed before the patient returns for their subsequent appointment.
Space closure was undertaken using nickel–titanium coil springs as they have been shown to be an efficient method of tooth movement.Citation10–Citation12 Sliding mechanics was carried out en masse, by including the whole of the labial segment (incisors and canines) against the premolars and molars and avoiding an initial canine retraction stage. En masse space closure represents common clinical practice and is usually required for patients treated with a pre-adjusted edgewise appliance and premolar extractions. The use of intermaxillary elastics was avoided until after space closure had been achieved, although Dixon and colleagues,Citation10 did not find this to be a significant factor explaining the rate of space closure. Another potential confounder could have been the number of broken appliances during the experimental period. There were eleven incidences of ‘broken appliances’ recorded in trial participants during the experimental period; however, only on four occasions were these considered relevant to space closure mechanics. As this number was small (4 out of 263 readings; 1·5%), we considered the effect on the results minimal.
We chose an inter-individual, parallel group design, similar to Dixon et al.,Citation10 as we did not consider the two sides of space closure to be mutually independent of each other because they involved the same archwire. Several studies investigating space closure or canine retraction have used an intra-individual, split mouth design.Citation4,Citation11,Citation12,Citation17,Citation18,Citation21 The advantage of an intra-individual design is that it might allow more precise comparison between techniques by removing the confounding factor of variability in the rate of tooth movement between individuals. Conversely, it could be argued that it would be unusual to use different methods of space closure on the two sides of an arch in the same individual, therefore this does not accurately reproduce orthodox clinical practice. It might also be possible that a split mouth design would introduce an additional confounder if the method of space closure on one side of the arch either increased or decreased the rate of tooth movement on the contra-lateral side. For these reasons we believe that an inter-individual, parallel group design to compare bracket/ligature combinations was appropriate. Although we found no statistical difference in the rate of space closure between the right and left sides of the arch, the sample size was not based on detecting this difference. Closer examination of the data revealed that when there were available data from both sides of the arch over half the readings (45 out of 87; 52%) demonstrated a 0·5 mm or greater difference in the amount of tooth movement between the sides (max 4·3 mm difference after 72 days). This would suggest that a parallel group study design would be more appropriate for research in this area in the future.
The method of data collection was similar to that of Mezomo et al.Citation18 and Dholakia and Bhat.Citation4 Study models were taken immediately before space closure was started and at each 4-week adjustment appointment for three visits or until the both spaces were closed. This allowed a visit-by-visit assessment of space closure, but more importantly the records were suitably masked and anonymized prior to both the initial and repeat measurements to minimize assessment bias. Neither Mezomo et al.Citation18 nor Dholakia and BhatCitation4 explain whether they masked their models. Dixon and colleaguesCitation10 collected data from masked study models taken before space closure was started and at four months or ‘earlier if space closure was complete’, but do not state what their recall appointment times were between 1 and 4 months. MilesCitation17 and BurrowCitation21 collected data from direct intra-oral measurements, the former using a digital calliper and the latter a flexible ruler. Although the investigators took several readings and averaged them, which would help to minimize random measurement error, neither describes how they adequately blinded the assessor as to group-side allocation.
We used data from a previous studyCitation10 to support an a priori sample size calculation to find a significant difference in the rate of space closure of 3 mm in 3 months. This was chosen as we considered it to be a reasonable length of time to detect a difference in the amount of space closure between the three groups if a difference did actually exist. It could be argued that 3 mm over 3 months is a large clinical difference to detect and a smaller difference would be more reasonable. Dixon et al.Citation10 used a similar figure in their sample size calculation and estimated that an average participant in their trial with 2 mm of space left in any quadrant at the end of four months would have a reduced treatment time of 3·2 months if treated with a nickel–titanium closing coil compared with an active ligature. The value for the variability of space closure over 3 months (2·58 mm) was an estimate, as we were unable to find any data in the literature. It was derived by multiplying the standard deviation quoted by Dixon et al.Citation10 for the variation in the monthly rate of space closure by three. This proved to be an overestimate of the variability in the rate of space closure over 3 months (). When the actual standard deviation (1·2 mm) from the study is used in the calculation the sample size was sufficient to detect a difference of 1·4 mm over 3 months with the same power and significance level.
We found a higher proportion of participants in our trial achieved space closure on one or both sides before the end of the 3-month trial period (22 patients, 52%) compared to other studies. MilesCitation17 reports that in two out of 15 patients who completed his trial (13%) the spaces closed during the alignment phase and were therefore excluded from the analysis. Dixon et al.Citation10 found that approximately one-third of the quadrants in their study were closed before the end of the 4-month experimental period. Our data would suggest that even if we had found a significant difference of 3 mm in a 3-month period between participant groups that this would equate to a saving of one visit or 4–6 weeks over the course of a 2-year treatment. It would be interesting to determine if patients consider this to be clinically significant.
Another criticism of this study might be that the sample size was too small to detect a significant difference between the bracket/archwire combinations; however, the descriptive data showed that there were very small mean differences in the amount of space closure between the three groups after 3 months with wide overlap of the confidence intervals. Based on these data, it is very unlikely that a study with a considerably larger sample size would detect a significant difference and suggests that the hypothesis of reducing static friction by modifying the bracket/ligature interface in order to increase the rate of tooth movement and hence reduce the length of orthodontic treatment, is questionable. Laboratory investigations indicate that archwire binding and notching have a more significant effect on any resistance to movement than static or dynamic friction.Citation24 The effects of other factors present in the mouth, such as salivary lubrication, shock absorption of the periodontal ligament and stress-breaking perturbations during mastication have also not been considered. Animal and clinical studies demonstrate that the largest factor in determining the rate of tooth movement is probably the individual patient response to any applied force.
Conclusions
No differences were found in the amount of space closure between three different bracket/archwire combinations.
The largest factor in determining the rate of tooth movement is probably the individual patient response to any applied force.
References
- Eberting JJ, Straja SR, Tuncay OC. Treatment time, outcome, and patient satisfaction comparisons of Damon and conventional brackets. Clin Orthod Res 2001; 4: 228–34.
- Harradine NW. Self-ligating brackets and treatment efficiency. Clin Orthod Res 2001; 4: 220–27.
- Crawford NL, McCarthy C, Murphy TC, Benson PE. Physical properties of conventional and Super Slick elastomeric ligatures after intraoral use. Angle Orthod 2010; 80: 175–81.
- Dholakia KK, Bhat SR. Clinical efficiency of nonconventional elastomeric ligatures in the canine retraction phase of preadjusted edgewise appliance therapy: an in-vivo study. Am J Orthod Dentofacial Orthop 2012; 141: 715–22.
- Khambay B, Millett D, McHugh S. Evaluation of methods of archwire ligation on frictional resistance. Eur J Orthod 2004; 26: 327–32.
- Griffiths HS, Sherriff M, Ireland AJ. Resistance to sliding with 3 types of elastomeric modules. Am J Orthod Dentofacial Orthop 2005; 127: 670–75.
- Hain M, Dhopatkar A, Rock P. A comparison of different ligation methods on friction. Am J Orthod Dentofacial Orthop 2006; 130: 666–70.
- Chen SS, Greenlee GM, Kim JE, Smith CL, Huang GJ. Systematic review of self-ligating brackets. Am J Orthod Dentofacial Orthop 2010; 137: 726 e1–18.
- Fleming PS, Johal A. Self-ligating brackets in orthodontics. A systematic review. Angle Orthod 2010; 80: 575–84.
- Dixon V, Read MJ, O’Brien KD, Worthington HV, Mandall NA. A randomized clinical trial to compare three methods of orthodontic space closure. J Orthod 2002; 29: 31–36.
- Samuels RH, Rudge SJ, Mair LH. A comparison of the rate of space closure using a nickel-titanium spring and an elastic module: a clinical study. Am J Orthod Dentofacial Orthop 1993; 103: 464–67.
- Samuels RH, Rudge SJ, Mair LH. A clinical study of space closure with nickel-titanium closed coil springs and an elastic module. Am J Orthod Dentofacial Orthop 1998; 114: 73–79.
- Miles PG, Weyant RJ, Rustveld L. A clinical trial of Damon 2 vs conventional twin brackets during initial alignment. Angle Orthod 2006; 76: 480–85.
- Scott P, DiBiase AT, Sherriff M, Cobourne MT. Alignment efficiency of Damon3 self-ligating and conventional orthodontic bracket systems: a randomized clinical trial. Am J Orthod Dentofacial Orthop 2008; 134: 470 e1–8.
- Fleming PS, DiBiase AT, Sarri G, Lee RT. Comparison of mandibular arch changes during alignment and leveling with 2 preadjusted edgewise appliances. Am J Orthod Dentofacial Orthop 2009; 136: 340–47.
- Fleming PS, DiBiase AT, Sarri G, Lee RT. Efficiency of mandibular arch alignment with 2 preadjusted edgewise appliances. Am J Orthod Dentofacial Orthop 2009; 135: 597–602.
- Miles PG. Self-ligating vs conventional twin brackets during en-masse space closure with sliding mechanics. Am J Orthod Dentofacial Orthop 2007; 132: 223–25.
- Mezomo M, de Lima ES, de Menezes LM, Weissheimer A, Allgayer S. Maxillary canine retraction with self-ligating and conventional brackets. Angle Orthod 2011; 81: 292–97.
- DiBiase AT, Nasr IH, Scott P, Cobourne MT. Duration of treatment and occlusal outcome using Damon3 self-ligated and conventional orthodontic bracket systems in extraction patients: a prospective randomized clinical trial. Am J Orthod Dentofacial Orthop 2011; 139: e111–16.
- Pandis N, Polychronopoulou A, Eliades T. Self-ligating vs conventional brackets in the treatment of mandibular crowding: a prospective clinical trial of treatment duration and dental effects. Am J Orthod Dentofacial Orthop 2007; 132: 208–15.
- Burrow SJ. Canine retraction rate with self-ligating brackets vs conventional edgewise brackets. Angle Orthod 2010; 80: 626–33.
- Nightingale C, Jones SP. A clinical investigation of force delivery systems for orthodontic space closure. J Orthod 2003; 30: 229–36.
- Pilon JJ, Kuijpers-Jagtman AM, Maltha JC. Magnitude of orthodontic forces and rate of bodily tooth movement. An experimental study. Am J Orthod Dentofacial Orthop 1996; 110: 16–23.
- Thorstenson GA, Kusy RP. Effects of ligation type and method on the resistance to sliding of novel orthodontic brackets with second-order angulation in the dry and wet states. Angle Orthod 2003; 73: 418–30.