The maternal mortality rate (MMR) per 100 000 live births in developing regions of the world is currently more than 20-fold higher than in industrialized high-income countries. In particular, 85% of the estimated maternal deaths (245 000 cases) occur in sub-Saharan Africa and Southern Asia. The gap that separates some of these countries from European industrialized regions in terms of lifetime maternal death risk is unacceptably high, with MMR ranging from about 1 in 20 in Chad, Burundi and Sudan to 1 in 20 000 in Austria, Italy, Greece and Estonia. According to the last report published by WHO, UNICEF, UNFPA and WB, about 300 000 deaths occurred in pregnant women in 2010, which translates to an MMR of 210 with an associated lifetime maternal death risk of 1 in 180. Though these values represent a 50% decrease from the levels of 1990, the objective of reaching a reduction in the MMR by three quarters between 1990 and 2015, the Millennium Developmental Goal 5 (MDG5) ‘Improve maternal health’, could be beyond reach.
The overall level of maternal health in a population is a function of a complex interplay of societal, cultural and economic factors that range from the role and the value of pregnant women in society to the availability of adequate infrastructures (primary care centres, and hospitals), of well-educated medical and paramedical personnel and of resources to keep the pace with progresses in diagnosis and treatment. Accordingly, between 1990 and 2010 the countries that have made most progress in reducing maternal deaths are those that could rely on an existing public health infrastructure and well-educated medical personnel while enjoying political stability and economic growth. Notable examples include Estonia, Belarus, Romania, Bhutan, Equatorial Guinea and the Islamic Republic of Iran, that achieved more than 80% reduction in MMR.
At the other extreme, in many sub-Saharan countries in the period from 1990 to 2010, the number of maternal deaths, rather than being under control, has increased. Here, a combination of poverty, lack of infrastructure and political instability has hampered the implementation of measures aimed at reducing maternal deaths. The looming worldwide economic crisis casts a shadow on the prospect of further improvements. Low- and middle-income countries will find it increasingly difficult to commit resources to consolidating the results achieved so far and will struggle to make further progress in reducing maternal death.
This situation dictates the need to better understand and to model the relationship linking capital investment, recurrent costs and the expected reduction of maternal death at different levels of MMR. This information will be invaluable in assessing the affordability of reaching the objective of reducing maternal mortality by 75% over the 1990 levels as well as for guiding case-by-case intervention measures. It must also be taken into account that a wide range of pathological conditions, including underlying maternal illness, implant anomalies, fetal-pelvic disproportion, postpartum infections and hemorrhages, can lead to maternal death. The prevention, the identification and the treatment of these conditions require different levels of skills, resources and infrastructures. To progress further in the reduction of maternal deaths, the pathological conditions must be prioritized on a country-by-country basis taking into account the resources available and their predicted impact.
In this issue, we interview Dr. Giovanni Putoto, a member of the executive board of Doctors for Africa CUAMM, a non-profit organization with the mission to improve maternal health, that runs 14 hospitals and 25 primary health centres in sub-Saharan Africa, to better understand the prospect of further reducing maternal deaths in the coming years. We also have two invited articles, one on the research gap of preterm birth risk in critical and underdeveloped countries, and another on the gap between recommendation and implementation of maternal vaccination for vaccine-preventable diseases in young infants.
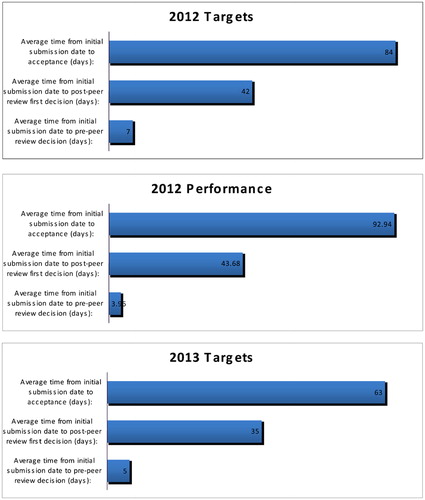
PGH targets and performance