
Abstract
Background
Rating of Perceived Exertion (RPE) is a subjective scale to monitor overload and fatigue during exercise. Hypoxia may worsen the perception of fatigue, compromising the self-reported perception of effort and increasing RPE. The objective was to evaluate the effects of carbohydrate (CHO) supplementation on RPE during exercise in hypoxia simulating 4200 m.
Methods
Eight male physically active volunteers performed two exercises at 50% VO2peak and 1% slope: exercise in hypoxia + placebo or exercise in hypoxia + CHO (6% maltodextrin) with supplementation at 20, 40, and 60 min during exercise. Oxygen Saturation (SaO2%) was assessed at baseline and after exercise, while RPE and HR were measured each 10 min during the trial.
Results
SaO2% decreased after exercise in both conditions of hypoxia compared to rest. The RPE did not differ between groups. However, the RPE increased in hypoxia after 20 min of exercise in relation to 10 min. The Area Under the Curve (AUC) of RPE was lower in hypoxia + CHO compared to hypoxia. The AUC of the HR/RPE ratio in the hypoxia + CHO group was higher in relation to hypoxia.
Conclusions
Our results indicate that CHO supplementation does not change RPE induced by 60 min of exercise at 50% VO2peak in hypoxia equivalent to 4200 m at the different times analyzed. However, in hypoxia + CHO the (AUC)-60 min of total RPE decreased during exercise, while the heart rate/RPE ratio improved, indicating lower RPE in the hypoxic environment.
Introduction
The Rating of Perceived Exertion (RPE) is a subjective scale used to prescribe the intensity and volume of exercise and measure the level of fatigue after an acute bout of exercise [Citation3, Citation27]. Several studies have demonstrated a high correlation between the RPE and physiological parameters such as Heart Rate (HR), lactate, and VO2max [Citation10, Citation12, Citation15]. In addition, RPE presents psychobiological aspects, including mood state and cognitive and physiological parameters on a single scale [Citation29].
Despite the importance of RPE in normoxic conditions, little is known about the behavior of this scale in hypoxic conditions or high altitudes. Indeed, exposure to hypoxia can worsen cognitive functions [Citation26], affecting mood state variables such as tension, vigor, fatigue, and mental confusion [Citation30, Citation31] limiting the ability to make decisions [Citation26, Citation36, Citation37]. These results suggest worsening of the self-reported perception of effort. One of the few studies that evaluated the effects of hypoxia on the RPE showed that individuals who presented a higher number of symptoms of acute mountain sickness also reported higher levels of perceived exertion [Citation20]. In addition, Souza et al. [Citation30, Citation31] demonstrated that moderate exercises performed in hypoxic environments for 45 min increase the systolic pressure of young males, as well as modifying the mood state and increasing anxiety [Citation30, Citation31].
In normoxic environments, different nutritional strategies are commonly used, before, during, and after performing physical exercises, with the ability to induce psycho-physiological modulations, Close et al. [Citation8]. For some time, carbohydrates have received attention in sports nutrition due to their role in performance and adaptability to training, as they provide essential fuel for the brain and central nervous system. Carbohydrates are versatile substrates for muscle work, aiding muscle to withstand exercises in a wide range of intensities due to their use by the anaerobic and oxidative pathways [Citation34].
Specifically regarding RPE, Backhouse et al. [Citation5] demonstrated that carbohydrates could influence RPE in normoxia. However, the influence of carbohydrates in hypoxia environments on RPE and cognition functions is unclear. Golja et al. [Citation14] demonstrate that carbohydrate supplementation in hypoxia causes higher ventilation and oxygen saturation in healthy young males, this being a possible mechanism for the influence of carbohydrates on a lower RPE during physical exercise. Moreover, the importance of carbohydrates during exercise in moderate hypoxia environments is higher in hypoxia than normoxia conditions due to higher endogenous carbohydrate oxidation in this condition [Citation21].
Nevertheless, little is known about the influence of carbohydrates on RPE in hypoxic environments. Thus, we propose to evaluate the effects of carbohydrate supplementation on RPE during exercise in hypoxia, simulating an altitude of 4200 m. We hypothesized that carbohydrate supplementation would attenuate increased RPE during exercise.
Material and methods
The present study included eight male volunteers, healthy and physically active. The sample characterization is presented in Table . The participation of all volunteers was approved by a doctor after a clinical examination, resting electrocardiogram, and stress test. All volunteers signed the consent form.
Table 1 Physiological characteristic from voluntaries
Experimental design
This is a cross-over study, in which the volunteers visited the laboratory three times. On the first visit, the volunteers carried out the resting and effort electrocardiogram and, simultaneously, the cardiopulmonary exercise test for peak oxygen uptake (VO2peak) determination. On the two subsequent visits, the volunteers performed: (I) exercise in hypoxia and placebo supplementation and (II) exercise in hypoxia and carbohydrate supplementation. All procedures were double-blind and randomized with respect to supplementation. There was a 7-day interval between each visit [Citation9].
Physiological parameters
VO2peak was determined in normoxia using an incremental exercise test on a treadmill (LifeFitness® - 9700HR). The initial velocity was set at 6.0 km/ h, increased by 1.0 km/h per minute until voluntary exhaustion. Respiratory and metabolic variables were obtained breath by breath using a metabolic system (Cosmed PFT4, Rome, Italy). A 1% slope on the treadmill was maintained throughout the test.
The volunteers performed 60 min of acute exercise at 50% VO2peak, and a 1% slope on the treadmill in the hypoxia condition simulated to 4200 m. All the physical exercise sessions were performed after fasting for 3 hours, to avoid possible dietary influences, and began at 02:00 pm. The pre-test meal was not controlled, but it was suggested that volunteers eat a light meal, and water intake in the hours preceding the test was ad libitum. The volunteers were advised not to perform strenuous exercises in the 24 h preceding the exercise.
Carbohydrate supplementation
Volunteers received a 200 ml solution of carbohydrate - CHO (maltodextrina strawberry-flavored) at 6% (w/v), at 20, 40, and 60-min during exercise with 228 kcal, or a placebo 0 kcal (strawberry-flavored Crystal Light® - Kraft Foods, Northfield, IL – USA). The groups received the same volume of placebo or carbohydrate in a double-blind manner.
Hypoxic environment
The study was performed in a chamber (normobaric chamber; Colorado Altitude Training/12 CAT-Air Unit) for altitude simulations of up to 4200 m, which is equivalent to a barometric pressure of 433 mmHg and fraction of inspired oxygen (FiO2) of 13.5% O2. This equipment has two air units allocated on the outside, which allow gas exchange (nitrogen increase and O2 reduction). A display inside the chamber shows the simulated altitude in real-time, measured by a module that contains an O2 cell sensitive to O2 variations.
Rating of perceived exertion determination
The RPE scale was used as a measure of perceived exertion during exercise. The scale ranges from 6 to 20, with anchors ranging from “very, very light” to “very, very hard” [Citation7]. Heart rate (HR) was measured using the Frequency meter (Polar®, Advantage Model NV, Kempele, Finland), and Hemoglobin O2 saturation (SaO2%) was measured by a finger oximeter (FingerPulse® model MD300C202, Minnesota - USA). SaO2% was assessed at baseline and after exercise, while RPE and HR were measured each 10 min during the trial.
Statistical analysis
Results of SaO2%, HR, RPE, and the HR/RPE ratio are expressed as mean standard ± deviation, and statistical analyses were performed by two-way repeated-measures ANOVA, after the Shapiro-Wilk normality test, followed by the Tukey post hoc test, at p < 0.05. The Area Under the Curve (AUC) was calculated using the trapezoidal rule to quantify the overall response of RPE and HR/RPE to exercise in the two different conditions studied. Statistical analyses were performed using UNIANOVA.
Results
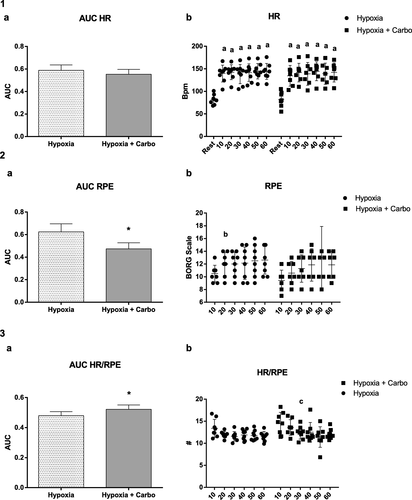
There was decrease in SaO2% after exercise in hypoxia (92.37 ± 3.50, F(1,6) = 3,79; p = 0.05) and hypoxia + CHO (89.25 ± 5.94, F(1,6) = 9,48; p = 0.03) in relation to rest in both groups (97.00 ± 0.92 / 96.00 ± 2.32), as shown in Fig. . In relation to HR there were increases at all moments during exercise in comparison to baseline, similarly in hypoxia F(1,6) = 16.64; p = 0.001 and hypoxia + CHO F(1,6) = 18.27; p = 0.001 as demonstrated in Fig. .1(b). The results of RPE are demonstrated in Fig. .2 (b). In hypoxia there was an increase at 20 min (12.37 ± 1.30 F(1,6) = 3.59; p = 0.041) in relation to 10 min (10.5 ± 1.30). In hypoxia + CHO supplementation we did not observe any increase at 20 (10.75 ± 1.75), 30 (11.50 ± 2.07), 40 (11.87 ± 2.35), 50 (12.87 ± 4.54), and 60 (11.87 ± 1.95) minutes in relation to 10 (9.62 ± 1.59) minutes F(1,6) = 2,03; p = 0,15). The HR/RPE ratio is shown in Fig. .3 (b). No differences were observed between the groups. However, in hypoxia + CHO there was a decrease at 20 min (13.56 ± 1.76) compared to 30 min (12.41 ± 1.46) F(1,6) = 5,51; p = 0.01. The AUC of HR did not differ between groups (0.58 ± 0.05 / 0.55 ± 0.04 F(1,5) = 1.69; p = 0.20), as shown in Fig. .1 (a). The AUC of RPE was lower in hypoxia + CHO (0.47 ± 0.05) compared to hypoxia (0.62 ± 0.07) F(1,4) = 11.66; p = 0.007, Fig. .2 (a). The AUC of HR/RPE in hypoxia + CHO (0.52 ± 0.02) was significantly higher than in the hypoxia condition (0.47 ± 0.02) F(1,4) = 5.09; p = 0.04, Fig. .3 (b).
Fig. 1 Hemoglobin Saturation. SaO2% in hypoxia and hypoxia + CHO conditions for n = 8 volunteers. The results represent the mean ± SD. (a) Different from Rest (b) different from Post in Hypoxia and Hypoxia + CHO group
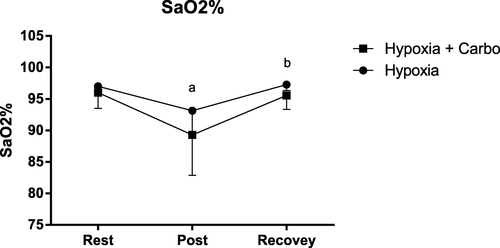
Fig. 2 HR and RPE. AUC – HR, RPE and HR/RPE in hypoxia and hypoxia + CHO conditions for n = 8 volunteers. 1(a) represents the AUC of Heart Rate, and 1(b) the Heart Rate during the different minutes. 2(a) represents the AUC of Rating Perception of Exertion, and 2(b) the Rating Perception of Exertion during the different minutes. 3(a) represents the AUC of the ratio of Heart Rate/Rating Perception Exertion, and 3(b) corresponds to the ratio of Heart Rate/Rating Perception Exertion during the different minutes. The results represent the mean ± SD. * different from Hypoxia, (a) different from Rest; (b) different from 10 min at Hypoxia Group; (c) different from 20 min in Hypoxia + CHO group
Discussion
The RPE represents psychobiological and physiological signs and symptoms on a single scale to evaluate the intensity and feeling of fatigue during exercise. However, little is known about this scale in hypoxia. Thus, the aim of the study was to evaluate the effects of carbohydrate supplementation on RPE during exercise in hypoxia, simulating an altitude of 4200 m. Our results indicate that there was no difference in the RPE during the different times analyzed after 60 min of exercise at moderate intensity in hypoxia. However, carbohydrate supplementation decreased total RPE during exercise in hypoxia, as indicated by a decrease in AUC of RPE and by the AUC of the HR/RPE ratio. The Area Under the Curve is a mathematical formula used to incorporate several time points to detect associations between repeated measures [Citation25]. An extensive review of AUC by Tilaki [Citation35] demonstrated that the analyses of AUC is of great importance for diagnostics, even being used in clinical epidemiology for the diagnosis of biomarkers and classification of disease. Different studies have used this statistical methodology to perform a global analysis of the results rather than just punctual analysis, as verified in the studies of [Citation1, Citation28, Citation32].
It is known that during hypoxia exposure, muscle carbohydrate metabolism changes, and there is higher carbohydrate oxidation compared to the normoxia condition. The energy supply via the glycolytic system is enhanced during endurance exercise in hypoxia, lactate and hydrogen ions (H+) are produced by the working muscle via the augmented energy supply from the glycolytic system and subsequently released into the blood circulation by Na+/H+ exchanger isoform 1 and monocarboxylate transporters, which elicits metabolic acidosis (lower muscle pH) [Citation33]. However, exogenous glucose uptake is compromised under hypoxic conditions, demonstrating the severity of exposure to high altitude. In a recent work, O'Hara et al. [Citation23] compared the co-ingestion of glucose and fructose on exogenous and endogenous substrate oxidation during prolonged exercise at high altitude (HA) versus sea level, in women, and the results showed that the rates of exogenous carbohydrate oxidation were significantly lower at HA.
In the present study, we evaluated the SaO2% in hemoglobin, as demonstrated in Fig. (a). We observed a significant decrease after exercise in both the hypoxia and hypoxia + CHO conditions, confirming previous studies [Citation6, Citation22]. A decrease in O2 saturation is one of the first consequences of hypoxia, occurring within a few minutes of exposure [Citation19]. Thus, the reduction in SaO2% after exercise found in hypoxia confirms the efficiency of the model studied to induce hypoxia and indicates that 4200 m, even for 60 min, is capable of reducing the O2 supply to several tissues.
This result could have a significant impact on the RPE since the supply of O2 is essential for the preservation of cognitive function and mood. Li et al. [Citation18] showed that mood, including stress, fatigue, and force progressively worsen proportionally to increases in hypoxia. Furthermore, studies have shown that hypoxia can worsen cognitive functions, including memory, learning, attention, and decision making [Citation13, Citation16, Citation24, Citation36].
In the current study, there was an increase in RPE at the 20th min of exercise compared to the 10th minute only in the hypoxia group. In addition, the AUC of RPE was significantly lower when the volunteers were supplemented with carbohydrates. Backhouse et al. [Citation5] demonstrated a reduction in self-reported perception of volitional fatigue in exercise lasting 90 min in normoxia. Furthermore, Fulco et al. [Citation11] did not find a difference in the RPE during exercise in hypoxia, similar to 4300 m after several days of energy deficit, unlike our study. Moreover, RPE increases when there is a decrease in blood glucose, since glucose is the primary fuel for the brain [Citation4].
RPE is influenced by the intensity and volume of exercise and presents high correlations with various physiological measures, including HR [Citation10, Citation15]. Despite the increase in HR from the 10th min of exercise, there was no difference between the two conditions studied. Fulco et al. [Citation11] found a higher HR after carbohydrate supplementation during exercise in hypoxia as opposed to our results. However, those authors used a different protocol and time of exposure. On the other hand, Ando et al. [Citation2] and Kubota et al. [Citation17] demonstrated differences in HR in a single bout of exercise performed in a hypoxia condition compared to normoxia.
The AUC of RPE demonstrated that carbohydrate supplementation was effective for reducing the effects of simulated hypoxic environments. The explanation is related to a possible increase in ventilation, as demonstrated in the study of Golja et al. [Citation14] and the increase in nutrients due to supplementation during the exercise, decreasing the fatigue generated by physical exercise Backhouse et al. [Citation5].
The HR/RPE ratio may be an index that represents the relationship between a physiological and psychological marker for recording the intensity of the exercise, and the level of fatigue [Citation29]. A reducing HR/RPE suggests an increased feeling of fatigue despite the intensity of the exercise. However, the effect of exercise in hypoxia on the HR/RPE ratio is unknown. In our study, there was no difference in the HR/RPE ratio at the different times analyzed during 60 min of exercise in hypoxia.
On the other hand, the HR/RPE was higher at 20 min in those supplemented with carbohydrate, but not significantly compared to hypoxia. Subsequently, after 30 min, the HR/RPE decreased, indicating that supplementation was efficient for partially preventing the first feelings of fatigue during exercise in hypoxia. Our results are confirmed by the AUC, demonstrating the global decline caused by exercise in hypoxia and recovery due to carbohydrate supplementation. This information on the response to carbohydrate supplementation during exercise can help sports nutritionists target better dietary strategies for athletes under hypoxic conditions.
Conclusion
In conclusion, our results indicate that carbohydrate supplementation does not change RPE at the different times analyzed during 60 min of exercise at 50% VO2peak in hypoxia equivalent to 4200 m. However, even during 60 min of acute hypoxia, the carbohydrate supplementation significantly decreased the Area Under the Curve (AUC)-60 min during exercise in hypoxia of RPE and improved the HR/RPE ratio, demonstrating the importance of carbohydrates to attenuate the impacts of hypoxic environments.
Authors’ contributions
ETS conceived, designed, and performed the experiments, analyzed the data, and wrote the paper. FFD and RMVM analyzed the data and wrote the paper. SAS and AVC performed the experiments. RVTS conceived and designed the experiments and wrote the paper. All authors read and approved the final manuscript.
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee for Research of the Universidade Federal de São Paulo (UNIFESP) - (CEP-0620/09) and is in accordance with the guidelines laid down in the Declaration of Helsinki adopted in 1964.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Abbreviations
| AUC | = | Area Under the Curve |
| CEP | = | Comitê de Ética e Pesquisa (Ethics Committee for Research) |
| CHO | = | Carbohydrate |
| FiO2 | = | Fraction of inspired oxygen |
| HA | = | High Altitude |
| HR | = | Heart Rate |
| O2 | = | Oxygen |
| RPE | = | Rating of Perceived Exertion |
| SaO2% | = | Hemoglobin O2 saturation |
| VO2max | = | Maximum oxygen volume |
| VO2peak | = | Peak oxygen volume |
Acknowledgments
All of the authors are grateful to the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP). We are also grateful to Sergio Tufik, for his support with reagents, materials, and analysis tools. Financial support: FAPESP: 2017/26563-2.
Funding
Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP). Financial Support: FAPESP: 2017/26563–2.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- Alsamir TibanaRManuel Frade de SousaNPrestesJ et al Is perceived exertion a useful indicator of the metabolic and cardiovascular responses to a metabolic conditioning session of functional fitness?Sports (Basel)20197 7 161 https://doi.org/10.3390/sports7070161
- AndoSHatamotoYSudoMKiyonagaATanakaHHigakiYThe effects of exercise under hypoxia on cognitive functionPLoS One20138 5
- AstorinoTAAllenRPRobersonDWJurancichMLewisRMcCarthyKAttenuated RPE and leg pain in response to short-term high-intensity interval trainingPhysiol Behav2012105 402 407 1:CAS:528:DC%2BC3MXhsFehu73J https://doi.org/10.1016/j.physbeh.2011.08.040 21925522 (a)
- AstorinoTARoupoliLRValdiviesoBRCaffeine does not alter RPE or pain perception during intense exercise in active womenAppetite201259 585 590 1:CAS:528:DC%2BC38Xht1GltbvE https://doi.org/10.1016/j.appet.2012.07.008 22813436 (b)
- BackhouseSHAliABiddleSJWilliamsCCarbohydrate ingestion during prolonged high-intensity intermittent exercise: impact on affect and perceived exertionScand J Med Sci Sports200717 605 610 1:STN:280:DC%2BD2sngtFemsQ%3D%3D https://doi.org/10.1111/j.1600-0838.2006.00613.x 17316376
- BillatVLLepretrePMHeubertRPKoralszteinJPGazeauFPInfluence of acute moderate hypoxia on time to exhaustion at vVO2max in unacclimatized runnersInt J Sports Med200324 9 14 1:STN:280:DC%2BD3s%2FntFKmsw%3D%3D https://doi.org/10.1055/s-2003-37251 12582946
- BorgGAVPsychophysical bases of perceived exertionMed Sci Sports Exerc198214 377 381 1:STN:280:DyaL3s7hsVChsw%3D%3D 7154893 7154893
- CloseGLHamiltonLPhilpABurkeLMortonJPNew strategies in sport nutrition to increase exercise performanceFree Radic Biol Med201698 144 158 1:CAS:528:DC%2BC28XitlSgur0%3D https://doi.org/10.1016/j.freeradbiomed.2016.01.016 26855422
- CoppelJHennisPGilbert-KawaiEGrocottMPThe physiological effects of hypobaric hypoxia versus normobaric hypoxia: A systematic review of crossover trialsExtreme Physiol Med20154 2 https://doi.org/10.1186/s13728-014-0021-6
- CouttsAJRampininiEMarcoraSMCastagnaCImpellizzeriFMHeart rate and blood lactate correlates of perceived exertion during small-sided soccer gamesJ Sci Med Sport200912 79 84 https://doi.org/10.1016/j.jsams.2007.08.005 18068433
- FulcoCSKambisKWFriedlanderALRockPBMuzaSRCymermanACarbohydrate supplementation improves time-trial cycle performance during energy deficit at 4,300-m altitudeJ Appl Physiol200599 867 876 1:CAS:528:DC%2BD2MXhtVChu7vE https://doi.org/10.1152/japplphysiol.00019.2005 15879171
- GarberCEBlissmerBDeschenesMRFranklinBALamonteMJLeeIMNiemanDCSwainDPQuantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exerciseMed Sci Sports Exerc201143 1334 1359 https://doi.org/10.1249/MSS.0b013e318213fefb 21694556
- GibsonGEPulsinelliWBlassJPDuffyTEBrain dysfunction in mild to moderate hypoxiaAm J Med198170 1247 1254 1:CAS:528:DyaL3MXksVSgs74%3D https://doi.org/10.1016/0002-9343(81)90834-2 6112879
- GoljaPFlanderPKlemencMMaverJPrinciTCarbohydrate ingestion improves oxygen delivery in acute hypoxiaHigh Alt Med Biol20089 53 62 1:CAS:528:DC%2BD1cXjtVKjt7Y%3D https://doi.org/10.1089/ham.2008.1021 18331221
- HaddadMChaouachiAWong delPCastagnaCHueOImpellizzeriFMChamariKInfluence of exercise intensity and duration on perceived exertion in adolescent taekwondo athletesEur J Sport Sci201414 275 281 https://doi.org/10.1080/17461391.2012.691115
- HornbeinTFTownesBDSchoeneRBSuttonJRHoustonCSThe cost the central nervous system of climbing to extremely high altitudeN Engl J Med198925 1714 1719 https://doi.org/10.1056/NEJM198912213212505
- KubotaYFukusakiCOkaneyaSMaegawaTNaritaKEffects of short hypoxic pre-exposure on physiological responses to subsequent hypoxic exerciseJ Phys Fit Sports Med20154 241 248 https://doi.org/10.7600/jpfsm.4.241
- Li XY, Wu XY, Fu C, Shen XF, Wu YH, Wang T. Effects of acute mild and moderate hypoxia on human mood state. Space Med Med Eng. 2000;(1):131–5.
- MazzeoRSPhysiological responses to exercise at altitude: an updateSports Med200838 1 8 https://doi.org/10.2165/00007256-200838010-00001
- MellorAJWoodsDRO’HaraJ et al Rating of perceived exertion and acute mountain sickness during a high-altitude trekAviat Space Environ Med201485 1214 1216 https://doi.org/10.3357/ASEM.4083.2014 25479264
- MorishimaTMoriASasakiHGotoKImpact of exercise and moderate hypoxia on glycemic regulation and substrate oxidation patternPLoS One201416 e108629 https://doi.org/10.1371/journal.pone.0108629
- MounierRPialouxVSchmittLRichaletJPRobachPCoudertJClottesEFellmannNEffects of acute hypoxia tests on blood markers in high-level endurance athletesEur J Appl Physiol2009106 713 720 https://doi.org/10.1007/s00421-009-1072-z 19430946
- O'HaraJPDuckworthLBlackAWoodsDRMellorAboosCGallagherLTsakiridesCArjomandkhahNCMorrisonDJPrestonTKingRFFuel use during exercise at altitude in women with glucose-fructose ingestionMed Sci Sports Exerc201951 2586 2594 1:CAS:528:DC%2BC1MXisVygtLrE https://doi.org/10.1249/MSS.0000000000002072 31206498
- PaintalSACognitive functions in extraordinary environmentsIndian J Med Res2004120 73 44 1:STN:280:DC%2BD2cvktFSrtA%3D%3D 15347855 15347855
- PruessnerJCKirschbaumCMeinlschmidGHellhammerDHTwo formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent changePsychoneuroendocrinology20037 916 931 https://doi.org/10.1016/S0306-4530(02)00108-7
- RoachEBBleibergJLathanCE et al AltitudeOmics: decreased reaction time after high altitude cognitive testing is a sensitive metric of hypoxic impairmentNeuroreport201425 814 818 https://doi.org/10.1097/WNR.0000000000000169 24722229
- RoseEAParfittGCan the feeling scale be used to regulate exercise intensity?Med Sci Sports Exerc200840 1852 1860 https://doi.org/10.1249/MSS.0b013e31817a8aea 18799997
- SakaguchiKTakedaKMaedaM et al Glucose area under the curve during oral glucose tolerance test as an index of glucose intoleranceDiabetol Int20157 1 53 58 https://doi.org/10.1007/s13340-015-0212-4 30603243
- SnyderACJeukendrupAEHesselinkMKKuipersHFosterCA physiological/psychological indicator of over-reaching during intensive trainingInt J Sports Med199314 29 32 1:STN:280:DyaK3s7nvFWntQ%3D%3D https://doi.org/10.1055/s-2007-1021141 8440542
- SouzaJFTGiampáSQCLEMOSVADe MelloMTSantosRVTAntunesHKMA condição de altitude simulada piora o estado de humor e aumenta a pressão arterial sistólica de jovens saudáveisMotricidade201511 71 81 https://doi.org/10.6063/motricidade.4042
- SouzaJFTGiampáSQCLEMOSVASantosSASilvaETDe MelloMTSantosRVTAntunesHKMExercise performed at hypoxia influences mood state and anxiety symptomsMotriz201521 177 184
- SteinerJLA CurmaciAPatrieJTGaesserGAWeltmanAEffects of carbohydrate supplementation on the RPE-blood lactate relationshipMed Sci Sports Exerc200941 6 1326 1333 1:CAS:528:DC%2BD1MXmt1ejtrs%3D https://doi.org/10.1249/MSS.0b013e3181967637 19461531
- SumiDKojimaCGotoKImpact of endurance exercise in hypoxia on muscle damage, inflammatory and performance responsesJ Strength Cond Res201832 1053 1062 https://doi.org/10.1519/JSC.0000000000001911 28368957
- ThomasDTErdmanKABurkeLMAmerican College of Sports Medicine position stand nutrition and athletic performanceMed Sci Sports Exerc201648 3 543 568 1:CAS:528:DC%2BC28XjtFKgtLk%3D https://doi.org/10.1249/MSS.0000000000000852 26891166
- TilakiKHReceiver operating characteristic (ROC) curve analysis for medical diagnostic test evaluationCaspian J Intern Med20134 627 635
- Virués-OrtegaJBuela-CasalGGarridoEAlcázarBNeuropsychological functioning associated with high-altitude exposureNeuropsychol Rev200414 197 224 https://doi.org/10.1007/s11065-004-8159-4 15796116
- ZhangGZhouSMYuanCTianHJLiPGaoYQThe effects of short-term and long-term exposure to a high-altitude hypoxic environment on neurobehavioral functionHigh Alt Med Biol201314 338 341 https://doi.org/10.1089/ham.2012.1091 24377340