
A light peel (superficial) stimulates epidermal growth.A medium peel causes epidermal regeneration and upper dermal renewal. A deep peel results in epidermal and dermal regeneration.
Protein precipitation can be an indicator of completion of chemical reaction or depth of chemical destruction, and cannot be neutralized.

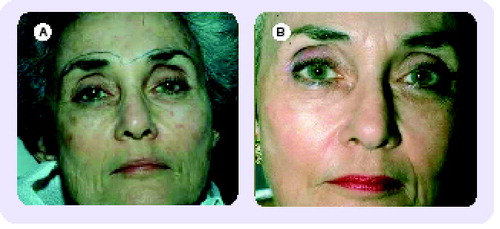
(A) Preoperative, (B) Postoperative.
With so many new peel preparations emerging onto the market today, it is important for the dermatologist to learn about the new products and the best way is by referring to the medical literature rather than the advertising or marketing campaign common among market-driven cosmetic products.
Since all peeling agents – superficial, medium-depth and deep – are derived from basic chemicals known to cause exfoliation, destruction and/or inflammation of skin in a controlled manner, the clinician must ask what is new and better about the product. Peeling agents, regardless of their proprietary new name, fall into chemical families. The clinical evaluation of these generic agents is well documented in our literature as to efficacy, technical care and safety.
It is the responsibility of the dermatological surgeon to be in control of their chemicals and products. Therefore, it is necessary to understand all the products and the peel formulation, and be sure it has undergone the test of objective scientific study with clear clinical evaluations and histology. Only then will we truly know the effectiveness of the agents we are using for exfoliating and resurfacing.
The explosion of interest in chemical peeling and laser resurfacing on the part of dermatologists has paralleled the general public’s interest in acquiring a youthful appearance by rehabilitating the photoaged skin. Advertising has further heightened the public’s interest for cosmetic agents, over-the-counter chemicals and treatment programs that have entered the general market of products meant to rejuvenate skin and erase the marks of sun damage and age. Patients have tried most of these over-the-counter home do-it-yourself programs and, by the time they consult their dermatologist, they are ready for a more definitive procedure performed with either chemical peeling or laser resurfacing. The patient would first request nonablative procedures with a laser such as intense pulsed light (IPL), radiofrequency skin tightening or Yag laser procedures with no down-time. If results are not adequate, the physician can suggest ablative procedures: light- or medium-depth peeling. It is the obligation of the physician to analyze the patient’s skin type and the degree of photoaging skin and, thus, prescribe the correct facial rejuvenation procedure. This should be the procedure or combination of procedures that will give the greatest benefit with fewer risk factors and morbidity. Chemical peeling has been the tried and true basic procedure. A renewed interest in realistic results has sparked new interest in chemical peels, especially the medium-depth peel.
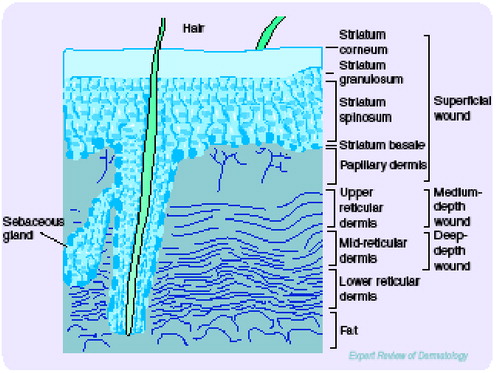
Chemical peeling involves the application of a chemical exfoliant to wound the epidermis and dermis, and thus, remove superficial lesions and improve the texture of skin. Various acidic and basic chemical agents are used to produce the varying effects of light to medium to deep chemical peels through differences in their ability to destroy skin. The level of penetration, destruction and inflammation determines the level of peeling Citation[1]. The stimulation of epidermal growth through the removal of the stratum corneum without necrosis is a light superficial peel. Through exfoliation, it thickens the epidermis with qualitative regenerative changes. Destruction of the epidermis defines a full superficial chemical peel, which induces the regeneration of the epidermis. Further destruction of the epidermis and induction of inflammation within the papillary dermis constitutes a medium-depth peel. Then, further inflammatory response in the deep reticular dermis induces new collagen production and ground substances, which constitutes a deep chemical peel. These have now been well classified, and use has been categorized for various degenerative conditions associated with photoaging skin, based on levels of penetration . Thus, the dermatologist has tools capable of solving problems that may be mild, moderate or severe with agents that are very superficial, superficial, medium-depth and deep peeling chemicals.
Indications & patient selection
Analyzing the patient with photoaging skin must take into account skin color and skin type, as well as the degree of photoaging. Pigmentary risks are generally not a great problem with very superficial chemical peeling, but may become a significant problem with medium and deep chemical peeling. It can also be a significant risk when regional areas, such as the lips and eyelids, are deep peeled, creating a significant color change in these cosmetic units from the rest of the face. The physician must inform the patient of this and other potential problems, especially if the skin type is III–VI. It must be justified whether the benefits of the procedure outweigh these risks and, in addition, the physician must plan for the appropriate techniques to prevent these unwanted changes in color.
The Glogau system classifies severity of photodamage, taking into account the degree of epidermal and dermal degenerative effects. The categorization is I–IV, ranging from mild, moderate, advanced and severe photodamaged skin. These categories are devised to project which patients need therapeutic intervention. Category I, or minimal degree photodamage, can be treated with light chemical peeling and medial treatment. Categories II and III would entail medium-depth chemical peeling, while category IV would need deep peeling or resurfacing plus cosmetic surgical intervention for gravitational changes Citation[2].
The peeling agent is a chemical eshcarotic that damages the skin in a therapeutic manner. It is important that the physician understands the patient’s skin and its ability to withstand this damage. The epidermis and stratum corneum have a barrier function against noxious chemicals and some skin types withstand the damage to a greater degree than others, while particular skin disorders have a greater tendency to produce side effects and complications from chemical peels, owing to poor barrier function or exaggerated inflammatory reactions. Patients with extensive photodamage may require stronger peeling agents and repeated applications of medium-depth peeling solutions to obtain therapeutic results. Therefore, a careful evaluation of skin types and problems must be assessed.
Herpes simplex can be a postoperative problem with significant morbidity. Susceptible patients should be pretreated with antiherpetic agents, such as acyclovir or valcyclovir, to prevent herpetic activation. These patients can be identified in the preoperative consultation and placed on appropriate therapy at the time of the chemical peel Citation[3].
Medium-depth chemical peeling
The definitive medium-depth resurfacing procedure has been, and remains, chemical peeling in the face of newer laser procedures. The procedure has 5–7 days down-time for healing, but truly delivers what the patient desires by resurfacing moderate photoaging skin. Medium-depth chemical peeling is defined as controlled damage from a chemical agent to the epidermis and papillary dermis, resulting in specific regenerative changes that can be performed in a single setting Citation[4]. Agents currently used include combination products, such as Jessner’s solution, 70% glycolic acid and solid carbon dioxide with 35% trichloroacetic acid (TCA) . The benchmark for this level peel was 50% TCA. It has traditionally achieved acceptable results in ameliorating fine wrinkles, actinic changes and preneoplasia. However, since TCA itself is an agent more likely to be fraught with complications, especially scarring, in strengths of 50% or higher, it has fallen out of favor as a single-agent chemical peel. It is for this reason that the combination products, along with a 35% TCA formula, have been found equally effective in producing this level of controlled damage without the risk of side effects.
Brody first developed the use of solid CO2 applied with acetone to the skin as a freezing technique prior to the application of 35% TCA. The preliminary freezing appears to break the epidermal barrier for a more even and complete penetration of the 35% TCA Citation[5].
Monheit then demonstrated the use of Jessner’s solution prior to the application of 35% TCA. Jessner’s solution was found to be effective in destroying the epidermal barrier by breaking up individual epidermal cells. This also enables a deeper penetration of the 35% TCA and a more even application of the peeling solution Citation[6]. Similarly, Coleman demonstrated the use of 70% glycolic acid prior to the application of 35% TCA. Its effect was very similar to that of Jessner’s solution.
All three combinations have proven to be as effective as the use of 50% TCA, but with a greater safety margin. The application of acid and resultant frosting are better controlled with the combination, and thus, the hot spots with higher concentrations of TCA can be controlled, creating an even peel with fewer incidences of dyschromias and scarring. The combination peel produces an even, uniform peel. The Monheit version of Jessner’s solution (35% TCA peel) is a relatively simple and safe combination . The technique is used for mild-to-moderate photoaging, including pigmentary changes, lentigines, epidermal growths, dyschromias and rhytids. It is a single procedure with a healing time of 7–10 days. It is also useful to remove diffuse actinic keratoses as an alternative to chemical exfoliation with topical 5-fluorouracil chemotherapy. Topical chemotherapy is applied for 3 weeks, creating erythema, scabs and crusts for up to 6 weeks. The combination peel will produce similar therapeutic benefits within 10 days of healing. Therefore, it reduces the morbidity significantly and gives the cosmetic benefits of improved photoaging skin.
The procedure is usually performed with mild preoperative sedation and nonsteroidal anti-iflammatory agents. The patient is told that the peeling agent will sting and burn temporarily, and aspirin is given before the peel and continued through the first 24 h if the patient can tolerate the medication. Its inflammatory effect is especially helpful in reducing swelling and relieving pain. If asprin is given before surgery, it may be all the patient requires during the postoperative phase.
Vigorous cleaning and degreasing is necessary for even penetration of the solution. The face is scrubbed gently with Ingasam (Septisol®, Vestal Laboratories) and next, an acetone preparation is applied to remove residual oils and debris.
After thorough cleaning, Jessner’s solution is applied with either cotton-tip applicators or 2 × 2 inch gauze. Jessner’s solution is applied evenly with usually one or two coats to achieve a light, but even, frosting. The TCA is painted evenly with one to four cotton-tipped applicators that can be applied over different areas with light or heavier doses of the acid.
The Jessner’s–TCA peel procedure is as follows:
| • | Skin should be cleaned thoroughly with septisol to remove oils | ||||
| • | Acetone or acetone alcohol is used to further debride oil and scale from the surface of the skin | ||||
| • | Jessner’s solution is applied | ||||
| • | 35% TCA is applied until a light frost appears | ||||
| • | Cool saline compresses are applied to dilute the solution | ||||
| • | The peel will heal with 0.25% acetic acid soaks and a mild emollient cream | ||||
The white frost from the TCA application appears complete on the treated area within 30 sec to 2 min. Even application should eliminate the need to reapply the TCA a second or third time, but if frosting is incomplete or uneven, the solution should be reapplied. The surgeon should wait at least 3–4 min after the application of TCA to ensure the frosting has reached its peak. The completeness of a frosted cosmetic unit can be documented and the area touched-up as required. Areas of poor frosting should be retreated carefully with a thin application of TCA. Overcoating TCA will increase its penetration and, thus, a second or third application will drive the acid further into the dermis, creating a deeper peel. Great care must be taken in overcoating areas, in which the take-up was not adequate or the skin is much thicker Citation[7].
Anatomical areas of the face are peeled sequentially from forehead to temple to cheeks and, finally, to the lips and eyelids. The white frosting indicates keratocoagulation or protein denaturation of keratin and, at that point, the reaction is complete. Careful feathering of the solution into the hairline and around the rim of the jaw and brow conceals the line demarcation between peeled and nonpeeled areas. The perioral area has rhytids that require a complete and even application of solution over the lip skin to the vermilion.
Eyelid skin must be treated delicately and carefully. A semi-dry applicator should be used to carry the solution within 2–3 mm of the lid margin. The solution should then be diluted immediately with cool saline compresses at the conclusion of the peel.
There is an immediate burning sensation as the peel solution is applied, but this subsides as frosting is completed. Cool saline compresses offer symptomatic relief for a peeled area as the solution is applied to other areas.
Postoperatively, edema, erythema and desquamation are expected. With periorbital peels and even forehead peels, eyelid edema can occur and may close the lids. For the first 24 h, the patient is instructed to soak four-times a day with a 0.25% acetic acid compress made of 1 tablespoon white vinegar in 1 pint of warm water. A bland emollient is applied to the desquamating areas after soaks. After 24 h, the patient can shower and clean gently with a mild nondetergent cleanser. The erythema intensifies as desquamation becomes complete within 4–5 days. Thus, healing is completed within 1 week to 10 days. At the end of 1 week, the bright red color has faded to pink and has the appearance of a sunburn. This can be covered by cosmetics and will fade fully within 2–3 weeks.
The medium-depth peel is dependent on three components for therapeutic effect: degreasing, Jessner’s solution and 35% TCA. The amount of each agent applied creates the intensity and, thus, the effectiveness of this peel. The variables can be adjusted according to the patient’s skin type and the areas of the face being treated. Therefore, it is the workhorse of peeling and resurfacing in the author’s practice as it can be individuated for most of the patients seen Citation[8].
Although the deep chemical peel has been a trusted method for severe photoaging, the use of the Baker’s peel has lost popularity for most dermatologists owing to its severity, risk factors, time factors, prolonged healing and down-time Citation[9]. In its place, the author prefers to use a combination of medium-depth peel for the face with selective CO2 laser resurfacing over discreet areas, perioral and periorbital, or manual dermasanding with the peel. The combined procedures are less aggressive without the significant side effects of hypopigmentation and alabaster texture. The younger population asking for skin rejuvenation wish for a more natural result than the older, deep peel procedures. The paradigm is to look natural and healthy for your age, rather than to produce dramatic results with obvious changes. The medium depth peels produce these results predictably.
Conclusion
The physician has the responsibility of choosing the correct modality to treat skin conditions, such as photoaging skin, scars, dyschromias and the removal of skin growths. There are many agents available including the three levels of chemical peels reviewed. It is the responsibility of the physician to have thorough knowledge of all of these tools to give each patient the correct treatment their condition warrants.
References
- Stegman SJ. A comparative histologic study of the effects of three peeling agents and dermabrasion on normal and sun-damaged skin. Aesthetic Plast. Surg.6, 123–125 (1982).
- Glogau RG. Chemical peeling and aging skin. J. Geratr. Dermatol.2(1), 30–35 (1994).
- Monheit GD. Facial resurfacing may trigger the herpes simplex virus. Cosm. Dermatol.8(7), 9–16 (1995).
- Brody HJ. Trichloracetic acid application in chemical peeling, operative techniques. Plast. Reconstr. Surg. 2(2), 127–128 (1995).
- Brody HJ. Variations and comparisons in medium depth chemical peeling. J. Dermatol. Surg. Oncol.15953–963 (1989).
- Monheit GD. The Jessner’s and TCA peel: a medium depth chemical peel. J. Dermatol. Surg. Oncol.15, 945–950 (1989).
- Rubin M. Manual of Chemical Peels. Lippincott, PA, USA, 120–121 (1995).
- Monheit GD, Zeitouni NC. Skin resurfacing for photoaging: laser resurfacing versus chemical peeling. Cosm. Dermatol.10(4), 11–12 (1997).
- Baker TJ, Gordon HL. Chemical Face Peeling. Surgical Rejuvenation of the Face.Mosby, St Louis, MO, USA (1986).