Abstract
Raltegravir was the first HIV integrase strand-transfer inhibitor to be approved by the US FDA, in October 2007, for the treatment of HIV-1 infection in combination with other antiretroviral agents. Raltegravir can be used in treatment-naïve and -experienced patients, as well as for the treatment of multidrug-resistant infection. Raltegravir exists in two formulations: a film-coated tablet administered orally at 400 mg twice daily, and a chewable tablet administered orally at 300 mg twice daily. In 2011, raltegravir was also approved for the treatment of children and adolescents, ages 2–18 years. For adolescents (ages 12–18 years), the recommended dose is 400 mg twice daily (film-coated tablet). If children (ages 6–12 years) weigh at least 25 kg, the film-coated tablet is recommended at 400 mg twice daily. Otherwise, patients receive the chewable tablet according to weight-based dosing at approximately 6 mg/kg/dose. Studies are ongoing for children ages 4 weeks to 2 years, and preliminary efficacy and safety data are promising. This article reviews current studies on the efficacy, safety, and pharmacokinetics of raltegravir in the pediatric population and the challenges of treating HIV in children and adolescents.
Introduction
According to the World Health Organization (WHO), there were approximately 34 million people living with HIV in 2011.Citation1 Children become infected through mother-to-child transmission (MTCT), which is the transmission of the virus from an HIV-infected mother to her child during pregnancy, labor and delivery, or breastfeeding. With proper antiretroviral (ARV) treatment, MTCT risks can be reduced to less than 5%.Citation2 However, limited availability and accessibility of ARV drugs in high-HIV-burden countries have resulted in an estimated 330,000 new infections in children in 2011.Citation3 Overall, children under the age of 15 years make up 10% of the global population infected with HIV/AIDS.Citation1,Citation3
The latest class of ARV drugs is integrase strand-transfer inhibitors, commonly referred to as integrase inhibitors. Two integrase inhibitors are currently marketed in the US, namely raltegravir and elvitegravir. Two second-generation inhibitors, dolutegravir and MK-2058, are in clinical trials. A liposomal form of dolutegravir, S/GSK744, is also under investigation. Raltegravir (brand name Isentress and formerly known as MK-0518) was developed by Merck and approved by the US Food and Drug Administration (FDA) in 2007 in combination with other ARV agents for treatment of adults infected with HIV. In 2011, raltegravir was also approved for use in children and adolescents, ages 2–18 years. At this time, it is not approved in the US for children less than 2 years of age.Citation4 Additional studies on raltegravir in the pediatric population are under way.
Raltegravir binds to the catalytic site of HIV-1 integrase and inhibits the insertion of viral deoxyribonucleic acid (DNA) into the chromosome of infected cluster of differentiation 4 (CD4+) lymphocytes. As a result, synthesis of the provirus is disrupted and new viral particles cannot be formed. Raltegravir has been shown to be potent, with an in vitro 95% inhibitory concentration (IC95) of 33 nM (0.014 mg/L) in 50% human serumCitation5 and an apparent in vitro IC50 of 2–7 nM (0.0008–0.003 mg/L).Citation6 This compound is effective against both wild-type and multidrug-resistant HIV-1 (isolates resistant to protease inhibitors, nucleoside reverse-transcriptase inhibitors, and non-nucleoside reverse transcriptase), and in both treatment-naïve and treatment-experienced HIV-infected adults.Citation4–Citation8
The aim of this paper is to briefly summarize clinically relevant information on raltegravir in adults and to present a more detailed description of raltegravir use in children and adolescents based on previously published clinical trials.
Clinical pharmacology
The US Department of Health and Human Services recommends administration of raltegravir with tenofovir and emtricitabine to treatment-naïve, HIV-infected patients.Citation9 HIV-infected adults (n = 160) receiving raltegravir 400 mg twice daily in combination with tenofovir 300 mg once daily and lamivudine 300 mg once daily had a geometric mean (GM) raltegravir area under the curve, 0–12 hours (AUC0–12) of 14.3 μMxhr (6.2 mgxh/L) and plasma concentration at 12 hours (C12) of 142 nM (0.062 mg/L).Citation4 At this dose, raltegravir achieved a mean viral load reduction of 1.66 log10 copies/mL in HIV-infected adults, with a C12 GM value greater than the in vitro IC95 in 50% serum.Citation5 Favorable safety and efficacy end points at 48 and 96 weeks have also been shown with 400 mg twice-daily raltegravir dosing in patients also receiving tenofovir/lamivudine.Citation5,Citation10,Citation11 Other studies, such as Blocking integrase in treatment Experienced patients with a Novel Compound against HIV: MeRcK, MK-0518 (NCT00293267 and NCT00293254)(BENCHMRK), Once Daily Isentress (NCT00941083)(ODIS) and MK-0518 protocol 071, (NCT00745823)(QDMRK), have been conducted and concluded that raltegravir (400 mg twice daily) was generally well tolerated and had potent ARV activityCitation8,Citation12–Citation14
In adults, the maximum plasma concentration (Cmax) is achieved approximately 3 hours postdose in the fasted state, and steady-state plasma concentrations are reached within the first 2 days of dosing. It is approximately 83% bound to human plasma protein over the concentration range of 2–10 μM (0.85–4.2 mg/L), and has an apparent terminal half-life of approximately 7–12 hours.Citation4 Raltegravir also exists as a chewable tablet and can be administered orally at 300 mg twice daily, since a bioequivalence study conducted in healthy adult volunteers suggested higher bioavailability with the chewable tablet compared to the 400 mg film-coated tablet.Citation4
The absorption of raltegravir is pH-dependent, such that the concentration of raltegravir is significantly altered by pH-altering agents such as proton-pump inhibitors. While omeprazole can cause a three- to four fold increase in raltegravir AUC and peak serum concentration, this effect is not clinically relevant and does not warrant a dose adjustment.Citation4,Citation15 Although raltegravir absorption can be affected by food intake, there were no clinically relevant changes in raltegravir pharmacokinetics.Citation4 Therefore, no dosage adjustment is needed because of diet, and raltegravir can be administered with or without food.
Raltegravir is metabolized primarily by the uridine diphosphate glucuronosyltransferase (UGT) 1A1 enzyme, leading to the formation of raltegravir glucuronide (30% of the dose).Citation16 Minor metabolism by UGT1A3 and UGT1A9 has also been reported.Citation16 In theory, it is possible that genetic variation in UGT isoenzymes could affect the pharmacokinetics of raltegravir. However, patients with UGT1A1*28, a decreased-function mutation allele of UGT1A1, did not have clinically relevant changes in the pharmacokinetics of raltegravir.Citation4 Raltegravir is not metabolized through the cytochrome P450 oxidation system. In in vitro studies, raltegravir was not a substrate of cytochrome P450 enzymes and did not induce or inhibit these enzymes. There are no reports of raltegravir inhibiting P-glycoprotein-mediated transport. Therefore, it is unlikely that raltegravir will alter the pharmacokinetics of drugs metabolized by the cytochrome P450 system or transported by P-glycoprotein. It is also unlikely that drugs altering cytochrome P450 enzyme activity will alter raltegravir exposure. Raltegravir is excreted in feces, mostly as raltegravir, and in urine, as raltegravir and raltegravir glucuronide. Dosage adjustments are not needed in patients with mild-to-moderate hepatic impairment. The effect of severe hepatic impairment on raltegravir exposure has not been studied.
Drug–drug interaction studies have been performed in adults. Changes in raltegravir plasma concentration are possible during coadministration of drugs that alter UGT1A1. For example, rifampin is an antibacterial drug used against tuberculosis and a strong inducer of UGT1A1. Therefore, the recommended raltegravir dose in patients concomitantly receiving rifampin is 800 mg twice daily.Citation4,Citation17 Other drugs that can induce or inhibit UGT1A1 have been shown to affect raltegravir plasma concentration. Atazanavir, an HIV protease inhibitor, inhibits UGT1A1 and has been shown to increase raltegravir plasma concentrations.Citation18,Citation19 However, the observed increases in C12, AUC0–12, and Cmax were not clinically relevant, and dose adjustments were not needed.Citation18,Citation19 Etravirine and efavirenz, two non-nucleoside reverse-transcriptase inhibitors, induce UGT1A1. One pharmacokinetic study with etravirine in healthy volunteers (n = 20) showed a 34% decrease in the minimum concentration (Cmin) of raltegravir.Citation20 The authors did not consider this change to be clinically significant, and therefore changing the dose of raltegravir is not needed. In contrast, suboptimal concentrations of raltegravir were detected in four HIV-infected patients also receiving etravirine.Citation21 The authors recommended further investigation of raltegravir in combination with etravirine in HIV-infected patients and the need for therapeutic drug monitoring.Citation21 In patients receiving efavirenz and raltegravir, the C12, AUC0–∞, and Cmax were lower compared to patients receiving raltegravir alone.Citation22 However, the authors concluded that these changes were not clinically significant. While ritonavir-boosted tipranavir treatment reduced the plasma concentration of raltegravir, the change was not clinically meaningful, and therefore it did not warrant a dose adjustment.Citation4
Raltegravir in the pediatric population
Managing HIV/AIDS in the pediatric population presents several challenges. Unlike HIV-infected adults, HIV-infected infants have a sharp rise in viral load in the first 2 months of life, followed by a slow decline in viral load within the next 2 years, which is often indicative of rapid disease progression.Citation23–Citation25 HIV-infected children will require lifelong treatment and monitoring for adherence, ARV toxicity, and the emergence of drug-resistant HIV-1 strains.
Pharmacological aspects, such as drug absorption, distribution, metabolism, and excretion, are age- and disease-dependent. Pharmacokinetic processes can differ between adults and children. For example, differences in raltegravir exposure due to gastric pH have been observed in adults. Thus, it is important to consider the variation in gastric pH, which affects pH-dependent passive diffusion in the first few years of life. At birth, the gastric pH is neutral (pH 6–8) due to the presence of amniotic fluid in the stomach.Citation26 Gastric pH quickly decreases within the first 48 hours of life and then increases again by days 8–10 of life.Citation26,Citation27 Adult values are approached by 3–7 years of age.Citation28 Based on differences seen in adults, it is likely that higher gastric pH at birth could increase absorption of raltegravir, while the subsequent lower gastric pH could decrease raltegravir exposure in neonates and infants. Gastric emptying, the rate at which drug is removed from the stomach, can also have an effect on drug absorption. Adult values are approached within 6–8 months of life.Citation28 Drug formulation and administration to children also need to be considered when dosing the pediatric population.
Since raltegravir is primarily metabolized by UGT1A1, it is important to consider the effect of age on UGT1A1 expression, which may affect raltegravir exposure. While transcripts of UGT1A and UGT1B isoenzyme family members are expressed in infants aged 6 months and up, hepatic glucuronidation activity of some drugs in children (ages 13–24 months) is lower than in adults.Citation29 However, differential metabolism of raltegravir in children has not been reported.
In 2011, raltegravir was approved for use in children aged 2–18 years. The primary study to support the broader treatment age was protocol P1066, conducted by the International Maternal Pediatric Adolescent Aids Clinical Trials (IMPAACT) network. P1066 is an ongoing phase I/II open-label multicenter trial evaluating the safety and pharmacokinetics of raltegravir in HIV-infected children aged 4 weeks to 18 years (clinicaltrials.gov, NCT00485264). The two-stage study was designed for treatment-experienced, integrase inhibitor-naïve children and adolescents, separated into six cohorts: cohort I (≥12 to <19 years), cohort IIA (≥6 to <12 years, receiving film-coated tablets), cohort IIB (≥6 to <12 years, receiving chewable tablets), cohort III (≥2 to <6 years), cohort IV (≥6 months to 2 years), and cohort V (≥4 weeks to <6 months). Age-based dosing and three formulations, namely film-coated tablets (cohorts I and IIA), chewable tablets (cohorts IIB and III), and oral granules in suspension (cohorts IV and V), were studied. Entry criteria included HIV infection with an HIV RNA ≥1,000 copies/mL and failure of at least one ARV regimen. Infants of less than 2 years were included if they failed preventive MTCT. Participants received raltegravir in combination with optimized background regimen. Target exposure in the pediatric population was calculated to approximate exposure reported in adults receiving 400 mg twice daily.
The primary objectives for stage 1 of P1066 were to evaluate short-term safety and tolerability over 4 weeks of raltegravir for each cohort, and to evaluate raltegravir pharmacokinetic parameters in each cohort to ascertain the appropriate dose. Dose evaluations were conducted sequentially from the oldest to the youngest cohorts, and alterations in doses were based upon mini-cohort and full-cohort pharmacokinetic results. Specifically, the first four subjects enrolled into a cohort were defined as a mini-cohort. If these four subjects passed the pharmacokinetic and safety criteria predefined by the protocol, the remaining stage 1 subjects (eight to twelve patients per cohort) were enrolled at that dose to complete enrollment of the full cohort. For mini-cohort and full-cohort dose decisions, the target minimum exposure was a GM AUC12 >14 μMxhr (6.2 mgxh/L), with a concurrent goal that the GM C12 exceed the in vitro IC95 of 33 nM (0.014 mg/L). Upon satisfactory pharmacokinetic and safety results for a full cohort, the next-younger cohort was opened (mini-cohort of four subjects, with stage 1 objectives). If pharmacokinetic and safety data for a mini- or full cohort were not acceptable, the raltegravir dose was linearly adjusted and intensive pharmacokinetics were performed at the new dose. The primary objectives for stage 2 of P1066 were to evaluate long-term safety and tolerability of raltegravir at the selected dose in combination with optimized background therapy in children and adolescents in the same age-based cohorts. Patient follow-up in this study is ongoing. Subjects will be followed for 5 years past 48 weeks, regardless of whether they continue raltegravir treatment.
In cohorts I–III, a total of 126 subjects were treated with raltegravir. After dose adjustments, pharmacokinetic analysis was performed on 96 patients receiving the final dose. For cohort I (≥12 to <19 years), the optimal dose established for the film-coated tablets was 400 mg twice daily for children between 12 and 18 years old. For cohort IIA (≥6 to <12 years), the appropriate dose was 400 mg (film-coated tablet) twice daily for patients between 6 and 11 years old and weighing more than 25 kg. For cohorts IIB (≥6 to <12 years) and III (≥2 to <6 years), the recommended dose was 6 mg/kg twice daily for a maximum of 300 mg (chewable tablet) twice daily. The recommended doses and pharmacokinetic data are summarized in . shows the concentration–time curves for cohorts I and IIA (film-coated tablet) and cohorts IIB and III (chewable tablet).
Figure 1 Raltegravir concentration–time curves for the adult formulation (triangles, n = 21) in P1066 cohorts I (≥12 to <19 years) and IIA (≥6 to <12 years) and the chewable tablet formulation (circles, n = 22) in cohorts ii (≥6 to <12 years) and III (≥2 to <6 years).
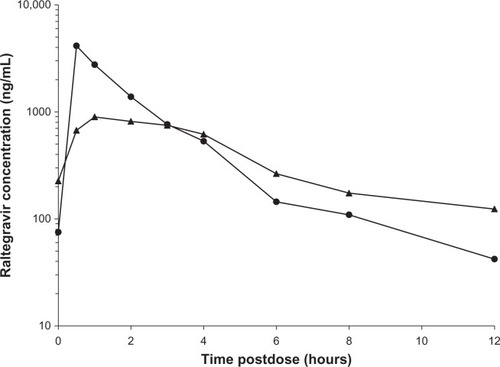
Table 1 Recommended doses and steady-state pharmacokinetic data for raltegravir in pediatric populationTable Footnotea
Raltegravir efficacy was assessed through virologic and immunologic responses at weeks 24 and 48. Preliminary data showed a virologic response in approximately 72% and 79% of patients at weeks 24 and 48, respectively.Citation30 The mean CD4+ change from baseline was 119 cells/mm3 and 156 cells/mm3 at 24 and 48 weeks, respectively.Citation30 Available and preliminary efficacy data are presented in . IMPAACT P1066 safety data showed that both film-coated and chewable tablets of raltegravir were generally well tolerated in children between 2 and 18 years. Up to week 24, only 13 of the 96 patients receiving the final dose had serious clinical events, and two subjects had serious laboratory events. Of these patients, two experienced raltegravir-related clinical events (psychomotor hyperactivity, abnormal behavior, insomnia, and allergic dermatitis) and one patient experienced raltegravir-related laboratory event (increase in transaminases).Citation4 Taken together, the safety and efficacy data gathered by the IMPAACT P1066 group were used to support the US FDA approval of raltegravir in combination with other ARV drugs for the treatment of HIV in children and adolescents, ages 2–18 years.
Table 2 Efficacy outcome of raltegravir in P1066 subjectsTable Footnotea
While raltegravir is not approved for children less than 2 years of age, the safety, efficacy, and pharmacokinetics of raltegravir in children between 4 weeks and 2 years old is currently being assessed within the P1066 protocol. Enrollment into cohorts IV (≥6 months to <2 years) and V (≥4 weeks to <6 months) is ongoing. Preliminary results have been reported from nine HIV-positive, treatment-experienced patients (ages 6 months to <2 years, mean 13 months) receiving raltegravir as oral granules in suspension at 6 mg/kg every 12 hours.Citation31 The AUC12 target was 14–25 μMxhr (6.2–12.1 mgxh/L) and a C12 >33 nM (0.014 mg/L). These targets (20 μMxhr and 115 nM for AUC12 and C12, respectively) were achieved in this study population (eight patients with pharmacokinetic data), indicating that weight-based dosing of raltegravir at 6 mg/kg every 12 hours is appropriate in patients aged 6 months to 2 years.Citation31 The median CD4+ T-cell change (95% confidence interval) from baseline was 687 (–297 to 1237) cells/μL at 12 weeks. Virologic success, defined as HIV RNA <400 copies/mL or ≥ 1 log drop from baseline, was observed in 78% of subjects. Furthermore, only two adverse events with grade ≥3 that could be due to raltegravir were noted, suggesting that raltegravir (oral granule formulation) was effective, well tolerated, and safe in children aged 6 months to 2 years.
The available P1066 results are in agreement with other studies (). Virologic, immunologic, and clinical responses to raltegravir-based therapy were evaluated in a study of 19 ARV-experienced children and adolescents, who did not experience a reduction in HIV-1 RNA to undetectable levels prior to the use of raltegravir.Citation25 The study population included two children aged 6 and 9 years, who received a dose of 8 mg/kg, and 17 adolescents (14–18 years), who received 400 mg raltegravir, twice daily. Patients also received one or two nucleoside reverse-transcriptase inhibitors, one non-nucleoside reverse-transcriptase inhibitor, and/or a boosted protease inhibitor (with or without maraviroc, enfuvirtide, and/or etravirine) background regimen. Sixteen patients were treated for more than 60 weeks, and six for more than 100 weeks. Seventeen patients (89%) had a 70%–90% increase in their CD4+ T-cell count. Virologic success was considered favorable, with 13 patients having HIV-RNA levels lower than 50 copies/mL within the first 4 months of raltegravir treatment. Moreover, only two ARV-related adverse events (mild-moderate short-term skin rash) were observed in patients receiving raltegravir, emtricitabine, and etravirine (one patient), or raltegravir, boosted darunavir, and etravirine (one patient), suggesting that raltegravir was safe for the population studied. Further, the authors did not find any resistance mutations to raltegravir at the end of follow-up.
Table 3 Comparison between adult (BENCHMRK) study and pediatric efficacy studies of raltegravir
Another study investigated the effects of raltegravir, etravirine, and darunavir/ritonavir in twelve perinatally HIV- 1-infected adolescents (median age was 15 years, range 12–17 years).Citation32 All patients had received prior ARV therapy (including one or two non-nucleoside reverse-transcriptase inhibitors, a median of six nucleoside reverse-transcriptase inhibitors, four protease inhibitors, and enfuvirtide were used in six patients) for a median duration of 15 years. All twelve patients had genotype-documented triple-class drug resistance. Patients received raltegravir 400 mg twice daily for a median treatment duration of 12 months (range 9–21 months). In 92% of patients (eleven), the viral load was less than 400 copies/mL at the 12-month median follow-up, and after 9 months of raltegravir treatment, the median CD4+ T-cell count (range) increased to 500 (18–1239) copies/mL from baseline (124 [13–484] copies/mL). This study therefore showed favorable virologic response in this group of adolescents.
At the time of FDA approval, raltegravir was designated as a pregnancy category C drug, since there were no adequate, well-controlled studies in pregnant women. Since then, several studies have evaluated raltegravir pharmacokinetics during the third trimester of pregnancy and postpartum. The authors of these studies found that while raltegravir exposure was highly variable between the third trimester and postpartum, these changes were not significantly different, suggesting that a dose adjustment was not needed during pregnancy.Citation33,Citation34 Case studies report a rapid decline in maternal HIV RNA without toxicity when raltegravir was initiated in combination with other ARV therapy during late pregnancy,Citation35–Citation37 which provides a rationale for its use in women with late antenatal care. More recently, IMPAACT protocol P1097 reported that raltegravir was safe over the first 20 weeks of life in infants born to HIV-infected pregnant women who received 400 mg of raltegravir twice daily for at least 2 weeks prior to delivery. Furthermore, MTCT of HIV was not observed.Citation38 Based upon these pharmacokinetic and safety findings, it is likely that raltegravir use during pregnancy will continue to rise.
Drug resistance
Mutations in the HIV integrase enzyme can lead to raltegravir failure. Three known pathways for resistance to raltegravir exist, and each pathway is characterized by at least two integrase mutations at Q148H/K/R, N155H, or Y143R/H/C in combination with at least one minor mutation in the Q148H/K/R pathway (L74M, E138A, E138K, or G140S).Citation39 The Q148R/H primary mutation is detected after short exposure to raltegravir, while after longer exposure to raltegravir, primary mutation Y143R predominates, suggesting a relationship between the prevalence of primary mutations and duration of raltegravir treatment.Citation40 It has also been suggested that as raltegravir administration continues, N155H mutants are replaced by viruses with higher resistance.Citation39
Most patients with raltegravir failure present with primary mutations at amino acid 155 and 148 and one or more secondary mutations.Citation41 Resistance to elvitegravir, the other approved integrase inhibitor, can also be attributed to primary mutations at positions 148 and 155. In a study investigating cross-resistance between raltegravir and elvitegravir in HIV-infected adults (ARV-experienced), 19 of the 40 samples who were failing on raltegravir-based ARV therapy (median treatment time [interquartile range] of 44.71 [22.57–70.57] weeks) had diminished elvitegravir susceptibility.Citation42 While resistance to elvitegravir appeared more frequently than to raltegravir, wide cross-resistance between raltegravir and elvitegravir was noted, suggesting that these two drugs cannot be used sequentially.
In a cross-resistance study between raltegravir and dolutegravir (an integrase inhibitor currently under FDA review), 39 clinical isolate samples obtained from 18 adults who failed raltegravir-based therapy were screened for integrase mutations, and 30 were found to have genotypic and phenotypic mutations to raltegravir.Citation43 Dolutegravir was shown to have normal level of activity against isolates with the N155H and the Y143R + T97A mutations and only small decreases in susceptibility to dolutegravir were observed in G140S + Q148H and G140S + Q148R mutants.Citation43 Similarly, dolutegravir was shown to have in vitro activity against site-directed molecular clones of integrase that were resistant to raltegravir.Citation44 Taken together, these results suggest limited cross-resistance between raltegravir and dolutegravir.
While raltegravir has a low genetic barrier to resistance, this effect has not been noted in pediatric studies. Nucleoside reverse-transcriptase inhibitors (emtricitabine, lamivudine, stavudine, and zidovudine), non-nucleoside reverse-transcriptase inhibitors (nevirapine) and protease inhibitors (lopinavir and ritonavir) can be administered at a very young age (starting at 15 days or younger). To limit the possibility of raltegravir acting as monotherapy and thereby increasing the chances of developing raltegravir resistance, it is important to determine whether these patients have baseline mutations in the reverse-transcriptase and protease enzymes before the addition of raltegravir to an ARV regimen. This could be important in infants that have received other drugs with a low genetic barrier to resistance, such as nevirapine.
Summary/conclusion
Significant advancement in ARV therapy has led to a reduction in MTCT of HIV in resource-rich countries. However, perinatal HIV infection has not been curbed in high-burden and often developing countries. As a result, the pediatric population infected with HIV increases every year. Raltegravir, the first FDA-approved integrase inhibitor, was shown to be safe and potent in both naïve- and treatment-experienced adult patients. Since its introduction to the market, its approval has been extended to children as young as 2 years with optimized background therapy.
Treating this special population can be tricky. Physiological differences between adults and children can alter drug pharmacokinetics. Furthermore, nonadherence can lead to decreased drug exposure and increased resistance. Finally, most ARVs are developed in tablet formulation and can be impractical for children. Liquid formulation, which requires syringes, refrigeration, and/or special dispensing bottles, may not be appropriate, especially in resource-poor countries. Raltegravir exists in two formulations: a film-coated tablet and a chewable tablet. These two formulations as well as an oral suspension of raltegravir were evaluated by IMPAACT protocol P1066. Results for the film-coated and chewable tablets showed that raltegravir was safe, well tolerated, and efficacious for the treatment of HIV-infected children aged 2–18 years. Studies with the oral suspension formulation, which would be advantageous for administration to infants, are ongoing. Further, in infants with single-dose nevirapine exposure, raltegravir-based therapy may be ideal, due to its high safety profile and efficacy.
More studies are needed with respect to the use of raltegravir in the pediatric population. In particular, there is a clear need to investigate and monitor drug resistance to raltegravir and cross-resistance with second-generation integrase inhibitors. Further, in most studies of ARV-experienced children, raltegravir has been used with protease inhibitors, and therefore there are limited data on its use with non-protease-inhibitor regimens. It will be important to ascertain that age-related physiological changes will not alter raltegravir pharmacokinetics, safety, efficacy, or drug–drug interactions.
If cohorts IV and V from P1066 demonstrate satisfactory pharmacokinetic, safety, and efficacy data, raltegravir will become the first integrase inhibitor to be approved in a population as young as 4 weeks of age. With other studies looking at raltegravir in pregnant women and for PMTCT, it is also possible that raltegravir could be used in neonates. As researchers strive to replicate the functional cure described by Persaud et al,Citation45 raltegravir, which has been shown to cause a rapid decline in HIV RNA, could be a contender in this strategy. In this context, raltegravir could also become a key player in preventing the establishment of latent HIV reservoirs.
While P1066 remains one of the more comprehensive studies investigating raltegravir in infants and adolescents, findings from P1066 are consistent with data from other, smaller studies. Because of its favorable efficacy, safety, and pharmacokinetic data, minimal drug interactions, and availability in different formulations, raltegravir is an ideal candidate for inclusion in treatment strategies for HIV-infected children and adolescents.
Disclosure
KBL and JRK have nothing to declare. EPA is the protocol pharmacologist for IMPAACT P1066. His laboratory is responsible for the analysis of patient samples and generating pharmacokinetic data for the protocol. The authors have no financial conflicts of interest to declare.
References
- World Health OrganizationHIV/AIDS fact sheet2013 Available from: http://www.who.int/mediacentre/factsheets/fs360/en/index.htmlAccessed March 15, 2013
- World Health OrganizationMother-to-child transmission of HIV Available from: http://www.who.int/hiv/topics/mtct/en/index.htmlAccessed March 18, 2013
- World Health OrganizationTreatment of children living with HIV Available from: http://www.who.int/hiv/topics/paediatric/en/index.htmlAccessed March 15, 2013
- Food and Drug AdministrationIsentress (raltegravir) tablets Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/022145s004lbl.pdfAccessed March 15, 2013
- MarkowitzMMorales-RamirezJONguyenBYAntiretroviral activity, pharmacokinetics, and tolerability of MK-0518, a novel inhibitor of HIV-1 integrase, dosed as monotherapy for 10 days in treatment-naive HIV-1-infected individualsJ Acquir Immune Defic Syndr200643550951517133211
- MillerMWitmerMStillmockKBiochemical and antiviral activity of MK-0518, a potent HIV integrase inhibitorPresented at: Oral abstract session of AIDS 2006 – XVI International AIDS ConferenceAugust 13–18, 2006Toronto, Canada Abstract THAA0302
- SteigbigelRTCooperDAKumarPNRaltegravir with optimized background therapy for resistant HIV-1 infectionN Engl J Med2008359433935418650512
- EronJJCooperDASteigbigelRTefficacy and safety of raltegravir for treatment of HIV for 5 years in the BENCHMRK studies: final results of two randomised, placebo-controlled trialsLancet Infect Dis201313758759623664333
- AIDSinfoGuidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents2013 Available from: http://aidsinfo.nih.gov/guidelines/html/1/adult-and-adolescent-arv-guidelines/0Accessed May 23, 2013
- MarkowitzMNguyenBYGotuzzoERapid and Durable Antiretroviral Effect of the HIV-1 Integrase Inhibitor Raltegravir as Part of Combination Therapy in Treatment-naive Patients with HIV-1 Infection: Results of a 48-week Controlled StudyJ Acquir Immune Defic Syndr200746212513317721395
- MarkowitzMNguyenBYGotuzzoESustained Antiretroviral Effect of Raltegravir After 96 Weeks of Combination Therapy in Treatment-naive Patients with HIV-1 InfectionJ Acquir Immune Defic Syndr200952335035619648823
- VispoEBarreiroPMaidaISimplification from protease inhibitors to once- or twice-daily raltegravir: the ODIS trialHIV Clin Trials201011419720420974575
- EronJJJrRockstrohJKReynesJRaltegravir once daily or twice daily in previously untreated patients with HIV-1: a randomised, active-controlled, phase 3 non-inferiority trialLancet Infect Dis2011111290791521933752
- SandkovskyUSwindellsSRobbinsBLNelsonSRAcostaEPFletcherCVMeasurement of plasma and intracellular concentrations of raltegravir in patients with HIV infectionAIDS201226172257225922948265
- IwamotoMWenningLANguyenBYEffects of omeprazole on plasma levels of raltegravirClin Infect Dis200948448949219143531
- KassahunKMcIntoshICuiDMetabolism and disposition in humans of raltegravir (MK-0518), an anti-AIDS drug targeting the human immunodeficiency virus 1 integrase enzymeDrug Metab Dispos20073591657166317591678
- WenningLAHanleyWDBrainardDMEffect of rifampin, a potent inducer of drug-metabolizing enzymes, on the pharmacokinetics of raltegravirAntimicrob Agents Chemother20095372852285619433563
- IwamotoMWenningLAMistryGCAtazanavir modestly increases plasma levels of raltegravir in healthy subjectsClin Infect Dis200847113714018513146
- NeelyMDecosterdLFayetAPharmacokinetics and pharmacogenomics of once-daily raltegravir and atazanavir in healthy volunteersAntimicrob Agents Chemother201054114619462520823282
- AndersonMSKakudaTNHanleyWMinimal pharmacokinetic interaction between the human immunodeficiency virus non-nucleoside reverse transcriptase inhibitor etravirine and the integrase inhibitor raltegravir in healthy subjectsAntimicrob Agents Chemother200852124228423218838586
- MénardASolasCMokthariSEtravirine-raltegravir, a marked interaction in HIV-1-infected patients: about four casesAIDS200923786987119363331
- IwamotoMWenningLAPetryASMinimal Effects of Ritonavir and Efavirenz on the Pharmacokinetics of RaltegravirAntimicrob Agents Chemother200852124338434318838589
- ShearerWTQuinnTCLaRussaPViral load and disease progression in infants infected with human immunodeficiency virus type 1. Women and Infants Transmission Study GroupN Engl J Med199733619133713429134873
- PalumboPEKwokSWatersSViral measurement by polymerase chain reaction-based assays in human immunodeficiency virus-infected infantsJ Pediatr199512645925957699539
- BrizVLeón-LealJAPalladinoCPotent and sustained antiviral response of raltegravir-based highly active antiretroviral therapy in HIV type 1-infected children and adolescentsPediatr Infect Dis J201231327327722330165
- AveryGBRandolphJGWeaverTGastric acidity in the first day of lifePediatrics1966376100510075949019
- Strolin BenedettiMBaltesELDrug metabolism and disposition in childrenFundam Clin Pharmacol200317328129912803568
- KingJAcostaEPediatric clinical pharmacology and its implications for antiretroviral drug developmentCurr Opin HIV AIDS20083327227619372978
- StrassburgCPStrassburgAKneipSDevelopmental aspects of human hepatic drug glucuronidation in young children and adultsGut200250225926511788570
- NachmanSAcostaEZhengNIMPAACT P1066: raltegravir (RAL) safety and efficacy in HIV infected (+) youth two to 18 years of age through week 48Presented at: 19th International AIDS ConferenceJuly 22–27, 2012Washington, DC Abstract TUAB0205
- SpectorSAcostaEPZhengNRaltegravir oral granules formulation in children 6 months to <2 years of age: interim results from IMPAACT P1066Programs and abstracts of the 19th Conference on Retroviruses and Opportunistic InfectionsMarch 5–8, 2012Seattle, WA Abstract 987
- ThuretIChaixM-LTamaletCRaltegravir, etravirine and r-darunavir combination in adolescents with multidrug-resistant virusAIDS200923172364236619823069
- BestBMCapparelliEStekARaltegravir pharmacokinetics during pregnancyPrograms and abstracts of the 50th Interscience Conference on Antimicrobial Agents and ChemotherapySeptember 12–15, 2010Boston, MA
- ColbersAMoltoJIvanovicJA comparison of the pharmacokinetics of raltegravir during pregnancy and post-partumPrograms and abstracts of the 12th International Workshop on Clinical Pharmacology of HIV TherapyApril 13–15, 2011Miami, FL
- JaworskyDThompsonCYudinMHUse of newer antiretroviral agents, darunavir and etravirine with or without raltegravir, in pregnancy: a report of two casesAntivir Ther201015467768020587860
- PinnettiCBaroncelliSVillaniPRapid HIV-RNA decline following addition of raltegravir and tenofovir to ongoing highly active antiretroviral therapy in a woman presenting with high-level HIV viraemia at week 38 of pregnancyJ Antimicrob Chemother20106592050205220630894
- WestlingKPetterssonKKaldmaANavérLRapid decline in HIV viral load when introducing raltegravir-containing antiretroviral treatment late in pregnancyAIDS Patient Care STDS2012261271471723101466
- ClarkeDAcostaEPRizkMLRaltegravir pharmacokinetics and safety in neonates (IMPAACT P1097)Programs and abstracts of the 20th Conference on Retroviruses and Opportunistic InfectionsMarch 3–6, 2013Atlanta, GA
- JohnsonVACalvezVGunthardHFUpdate of the drug resistance mutations in HIV-1: Mar 2013Top Antivir Med201321161423596273
- SichtigNSierraSKaiserREvolution of raltegravir resistance during therapyJ Antimicrob Chemother2009641253219447792
- GatellJMKatlamaCGrinsztejnBLong-term efficacy and safety of the HIV integrase inhibitor raltegravir in patients with limited treatment options in a phase II studyJ Acquir Immune Defic Syndr201053445646320306554
- GarridoCVillacianJZahoneroNBroad phenotypic cross-resistance to elvitegravir in HIV-infected patients failing on raltegravir-containing regimensAntimicrob Agents Chemother20125662873287822450969
- UnderwoodMRJohnsBASatoAMartinJNDeeksSGFujiwaraTThe activity of the integrase inhibitor dolutegravir against HIV-1 variants isolated from raltegravir-treated adultsJ Acquir Immune Defic Syndr201261329730122878423
- KobayashiMYoshinagaTSekiTIn vitro antiretroviral properties of S/GSK1349572, a next-generation HIV integrase inhibitorAntimicrob Agents Chemother201155281382121115794
- PersaudDGayHZiemniakCFFunctional HIV Cure after Very Early ART of an Infected InfantPrograms and abstracts of the 20th Conference on Retroviruses and Opportunistic InfectionsMarch 3–6, 2013Atlanta, GA Abstract 48LB