
Abstract
Background and objectives
The objective of this study was to assess the impact of strategies on the intention of dental students/graduates to practice in rural areas. The strategies included the recruitment of dental students from rural backgrounds and clinical rotations in rural areas during the training of dental students.
Materials and methods
The study undertook a systematic review and utilized meta-analysis to assess these strategies. International literature published between 2000 and 2015 was retrieved from three main search engines: Medline, Embase, and Scopus. The selected articles were scanned to extract the main content. The impact of the strategies was quantitatively assessed by meta-analysis, using the random-effect model. The pooled effect was reported in terms of odds ratios (ORs) with 95% confidence intervals. Sensitivity and subgroup analyses were performed. Publication bias was assessed by the Funnel plot and Egger’s test.
Results
Seven of the initially selected 897 articles were included for the full review. The majority of the selected articles had been published in developed countries. The meta-analysis results revealed that the pooled OR of rural exposure on the intention to practice in rural areas was approximately 4.1, statistically significant. Subgroup analysis showed that clinical rotations in rural areas tended to have a slightly greater influence on rural dental practice than recruiting students from rural backgrounds (OR 4.3 versus 4.2). There was weaker evidence of publication bias, which was derived from small-study effects.
Conclusion
Enrolling students with rural backgrounds and imposing compulsory clinical rotation in rural areas during their study appeared to be effective strategies in tackling the shortage and maldistribution of dentists in rural areas.
Introduction
It is universally accepted that the health workforce is a critical component of health systems. An adequate volume of skilled health workers with equitable distribution significantly contributes to achieving health goals.Citation1–Citation3 It is recommended that all countries should seek to achieve a health-workforce density of 2.28 doctors, nurses, and midwives per 1,000 population in order to ensure favorable health outcomes for their population.Citation3,Citation4 In this regard, the World Health Organization (WHO) has issued global recommendations to improve the recruitment and retention of a health workforce, particularly in rural and underserved areas.Citation4 Of the 16 recommended interventions, those that have proved successful in many countries have been the recruitment of students from rural backgrounds and the establishment of teaching programs that encourage students to have rural experience during their studies.Citation5,Citation6
While there is a fair amount of evidence in the fields of medicine and nursing, little is known about whether, or to what extent, the aforementioned aforementioned strategies are still applicable to other health cadres.Citation7–Citation10 Dentists are one of the groups within the health workforce for which there is the least evidence; this is despite the fact that oral diseases are a major health problem worldwide. Petersen et al highlighted the fact that the burden of oral diseases is particularly heavy on disadvantaged populations, in both developing and developed nations.Citation11–Citation14 Although the WHO recommendations are intended to cover all types of health workers, the evidence that was used to generate the recommendations was mostly based on medicine and nursing. Of the 105 pieces of research presented in the WHO recommendations, only one was directly related to dentistry.Citation15
Nonetheless, in recent years, there has been a growing body of research that has sought to assess the success of the aforementioned interventions in promoting the rural retention of dentists.Citation16–Citation18 However, there has not been any study attempting to compile all of this evidence in order to provide a robust answer about whether rural-retention strategies have “really” worked with regard to dentists. This study seeks to fill that knowledge gap by gathering evidence, via systematic review and meta-analysis approaches, to assess the impact of interventions promoting the retention of dentists in rural areas. It is hoped that the findings from this study will help to inform policy makers and academics interested in human resources for health planning, and that this may in turn assist them in implementing effective strategies to promote better recruitment and retention of dentists in rural areas. Furthermore, this study will help update the evidence of the validity of the WHO recommendations, six years after their initial publication. Note that the scope of this study is confined only to “rural exposure” strategies, ie, the recruitment of students from rural backgrounds, and the implementation of clinical rotations in rural areas during the training of dental students.
Materials and methods
A roundtable discussion was held by the authors to develop the review process, identify inclusion and exclusion criteria, and design the analysis plan. The review and meta-analysis findings were reported according to Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.Citation19
Search strategy
Potential articles were selected from two strands: a systematic search and a purposive search. In the systematic search, articles in the areas of medicine and dentistry were identified through three main search engines: Medline, Embase, and Scopus. In Medline, the search was performed through Medical Subject Headings (MeSH) and plain text. In Embase and Scopus, where MeSH searches are not applicable, an “exploding” search strategy was employed instead. The search was conducted in the keywords, abstracts, and titles of articles. The publication date was limited to studies published between January 1, 2000 and December 31, 2015. Due to limited capacity in language translation, studies written in any language but English were excluded. Truncations and wildcards were used in all search engines. The potential abstracts were retrieved from the library of the International Health Policy Programme, Ministry of Public Health of Thailand and its network libraries. presents the search terms applied in each database.
Table 1 Search terms used in Medline, Embase, and Scopus
In the purposive search, potential articles were retrieved from the website of the Human Resources for Health journal in the corresponding years. The search was focused on articles where the title keywords contained the terms “dentist” and “rural”. Additional references considered relevant to the review objective were also explored.
Study inclusion/exclusion
Abstracts of the articles initially retrieved from the search strategy were independently screened by two reviewers (RS and NC). Any disagreement between the two reviewers was resolved through discussion to reach a consensus. Articles that passed the initial screening were read in full to extract their key message to add to the data-extraction table. Eligible articles were included if they met all the following criteria: first, the study participants had to be either dental students or dental graduates; second, the main research method had to have been a quantitative approach; third, the study participants had to be divisible into two groups (an “exposure group” versus a “control group”); and fourth, the main outcome of interest had to be binary data, focusing on dental service in rural areas, either in terms of the intention to serve rural communities or real practice that already took place (“event” versus “no event”).
It should be noted that for convenience in communication, this study has outlined operational definitions of some important words/terms, which will be used from this point onward. “Exposure” participants refers to those participants with extensive experience in rural areas, either through having been brought up in rural areas or having experienced a program through school or university that provided opportunities to work, or practice, in a rural setting. Participants who did not fall into this category were considered “control” participants. For the study outcome, where participants (in the case of dental graduates) were providing dental services in rural areas, or where they showed a willingness/intention to practice in rural areas after graduation, this was described as “event”, while “nonevent” meant that they were neither practicing in rural areas, nor had they demonstrated a willingness/intention to do so. In addition, the term “rural” in this review encompassed a wide range of settings, including but not limited to remote areas, underserved areas, charitable works servicing underserved populations, and community-based settings. The authors were fully aware of the fact that each study site has its own way of defining “rural”. Given this situation, it is difficult to draw a rigid line indicating which setting should be regarded as “rural” and which should not. Accordingly, a more flexible approach was applied allowing for the interpretation of “rural” to be assessed according to each study’s context. A remark to remind the reader of the operational definition of how each study defined the term “rural” is displayed in the data-extraction table.
Articles were excluded from the review if they met any one of the following criteria: populations of interest were neither dental graduates nor dental students; the main data-collection technique used was a qualitative approach; the main message was not related to the intention of dental students/graduates to practice in rural communities; the study participants could not be classified into “exposure” and “control” groups; the outcome of the study demonstrating the binary difference between “event” and “nonevent” was lacking (note that a study exploring participants’ satisfaction with dental rural service in terms of satisfaction scores [using the Likert scale, for instance] without specifying a cutoff point for the authors to distinguish between an “event” and a “nonevent” also met this exclusion condition); and finally, articles where the information shown in the study abstract was insufficient to assess the relevance of the research to this review’s objective. All potential articles were then checked for duplication. EndNote software version X4 was used to store and manage recruited studies in a computerized format.
Assessment of study quality
The authors assessed the risk of bias and the quality of the selected studies without calculating a composite score or imposing a cutoff score to eliminate articles of apparently poor quality. Reasons for not using a cutoff score are outlined. Unlike in clinical trials, for observational studies (like all articles selected here), there has not been agreement on the critical elements for evaluating susceptibility to bias. Sanderson et al suggested that there were more than 86 tools for evaluating the quality of observational studies.Citation20 Furthermore, an article that appears to have poor quality from a checklist score may actually be less biased, because most scoring systems, such as the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline, assess the quality of “reporting” rather than the rigor of study design and methodology.Citation21 Even in clinical trials, Jüni et al recommended that the use of summary scores to identify studies of high quality might be problematic: relevant methodological aspects of each study should be assessed individually.Citation22 Therefore, in this study, the risk of bias and methodological limitations of the selected articles were described qualitatively in the data-extraction table, in order to remind the readers of possible biases that might influence the accuracy of the review results.
Statistical analyses
Main analysis
Meta-analysis was performed using the random-effect (RE) model (DerSimonian–Laird method).Citation23 Since almost all the selected articles were cross-sectional studies, the pooled and individual effects were reported in terms of odds ratios (ORs) with 95% confidence intervals (CIs). P-values less than 0.05 were considered statistically significant. As suggested by Borenstein et al, the authors considered the RE model to be a more appropriate choice than the fixed-effect (FE) model in this setting. This was because, firstly, it was assumed that there might be a considerable degree of heterogeneity between studies, resulting from intrinsic differences in the health care systems of each country. Furthermore, the RE model does not impose a restriction of common effect size like the FE model. This grants the RE model greater power of generalizability than the FE model.Citation23 Nonetheless, the pooled effect calculated by the FE model is briefly presented in the sensitivity-analysis subsection to allow the reader to compare the results between the two models. The degree of heterogeneity between studies was assessed by the I2 statistic. All calculations were performed by Stata 12.
Sensitivity and subgroup analyses
Sensitivity analysis was conducted by changing the effect size from OR to risk ratio (RR). While OR is more commonly used than RR in many observational studies, there is a risk of serious divergence between OR and RR when a study of interest has an extremely large effect. In such circumstances, OR might lead to an overestimation of the RR.Citation24 The sensitivity analysis also helped test whether the rural-exposure strategies were still robust, given a change in measurement of effect size. In addition, subgroup analysis was performed by dividing the selected articles into two groups: studies that explored the effect of a rural background on dental students/graduates, and studies that explored the effect of curricula or teaching programs that aimed at increasing the experience dental students had of rural areas.
Assessment of publication bias
Publication bias was assessed by two means: a visual inspection by funnel plot and Egger’s test. Egger’s test has been by far the most widely used approach for assessing small-study effects (a tendency for the effects estimated in small groups of students to differ from those estimated in larger studies). The result of Egger’s test are presented in terms of bias coefficient, which is derived from a regressing standard normal deviate of the effect estimated against its standard error.Citation25
Ethical approval
As this is a review manuscript where data were retrieved from open sources, the study was waived for applying for approval by the ethics committee of the Institute of the Development of Human Research Protections, Thailand.
Results
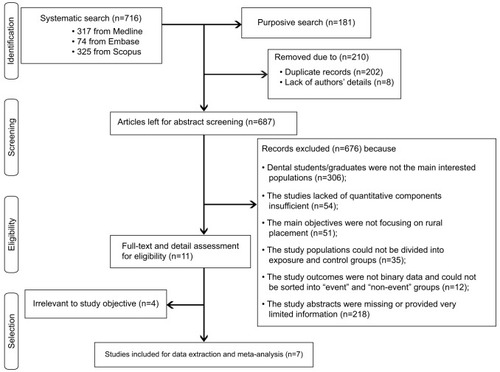
An overview of the study-selection process is illustrated in . A total of 897 articles were retrieved for initial screening: 716 articles from the systematic search (317 from Medline, 74 from Embase, and 325 from Scopus) and 181 articles through the purposive search. After the dropping of 202 duplicated articles and eight articles where the authors’ details were not available, 687 articles were left for initial abstract screening. Of the 687 articles, eleven met the inclusion criteria and were then read in full to assess their relevance to the review’s objective. The κ-coefficient for between-rater agreement came out at 0.4, indicating a fair level of agreement between the two reviewers (P<0.001).Citation26 The eleven articles were read in full, and of these, seven were identified that had sufficient information to be included in the meta-analysis. An example of the excluded articles was the study by Rohra et al, which investigated the association between community-based dental education and dentists’ attitude toward treating patients from underserved populations.Citation27 Although the article’s abstract appeared to meet the review’s inclusion criteria, its full text showed that the study participants were assessed for their attitudes by Likert-scale questionnaires: this made it difficult to distinguish the “event” participants from the “nonevent” participants.Citation27
Figure 1 Overview of the article-selection process.
Of the seven articles included for the final review, five were from high-income countries (three from the US and two from Australia).Citation28–Citation32 Only two studies were conducted in middle-income countries: South Africa and Thailand.Citation33,Citation34 Three articles explored the influence of rural origins of dental students/graduates,Citation32–Citation34 while the other four articles investigated the impact of special didactic programs or rural placements after graduation.Citation28–Citation31 It should be noted that the definition of “rural” varied across studies. For instance, McMillan and Barrie defined “rural” in South Africa as any administrative area that was smaller than a town or city,Citation33 whereas Thammatacharee et al considered the term “rural” to refer to all districts, other than provincial capitals, in all Thai provinces outside Greater Bangkok.Citation34 All the selected articles demonstrated some degree of bias, as they were conducted in uncontrolled settings where randomization was not feasible. A cross-sectional design was the most commonly used approach. Detailed characteristics and potential biases of each study are displayed in data-extraction tables ( and ). The number of participants varied considerably between studies. The lowest number of participants was found in Johnson and Blinkhorn (n=62).Citation29 McFarland et al enrolled the largest number of participants (n=1,361).Citation32
Table 2 Data-extraction table presenting key characteristics of each study
Table 3 Potential biases and methodological limitations in each study
Overall, experience of living or working in rural areas appeared to have a positive impact on intention to practice in rural areas. The ORs in most studies varied from 2.2 to 6.9. The only exceptions were found in Johnson and Blink-horn, where there was only one person from the “exposure” group that experienced the “event”, and this situation led to a huge OR of 56.4. Note that the ORs presented here might be slightly different from those presented in the original studies, since they were recalculated by the authors after excluding missing data and regrouping each study’s participants according to the review objective. The RE model meta-analysis revealed that the pooled estimate of the ORs of all seven studies was approximately 4.1, with statistical significance (as evidenced by the 95% CI of 2.6–6.5). The I2 statistic was as large as 66%, which reflected a substantial degree of heterogeneity (P=0.007). Therefore, because of this considerable degree of heterogeneity, the application of the RE model is considered a valid approach (; ).
Figure 2 Meta-analysis of all seven studies with random-effect model, showing results in terms of OR.
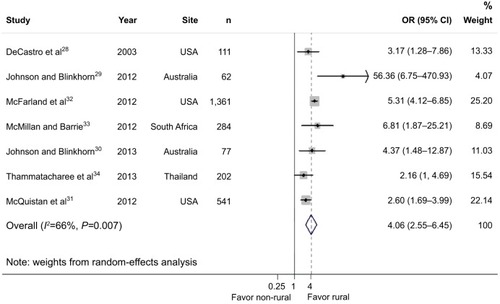
Table 4 Number of “exposure” and “control” participants in each study
The FE model (data not shown) had a slightly different result, with the pooled estimate increased to 4.3. A potential explanation for this slight difference from the RE model is that the FE model gave greater weight to articles with a larger volume of participants.
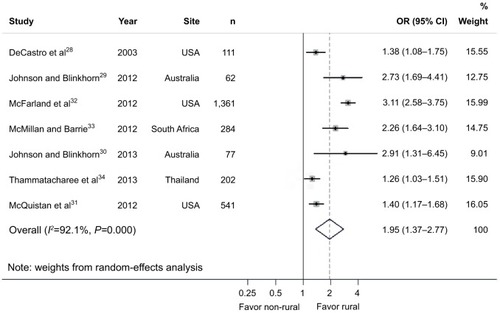
The sensitivity analysis was conducted by changing the measurement of the pooled estimate from OR to RR. The pooled RR (2) appeared to be about half the size of the pooled OR (4.1) but still had statistical significance. The I2 statistic became larger in the sensitivity analysis (92.1), illustrating that the RE model had greater validity than the FE model in this situation ().
Figure 3 Meta-analysis of all seven studies with random-effect model, showing results in terms of RR.
Abbreviations: RR, risk ratio; CI confidence interval.
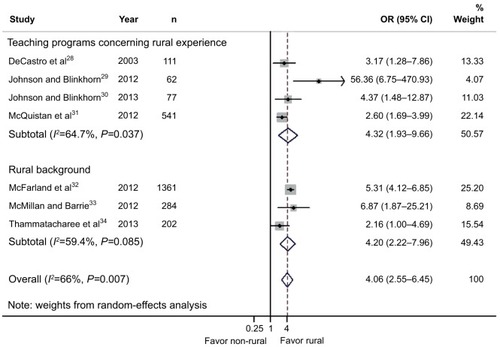
Subgroup analysis showed that the teaching programs that helped increase rural experience in dental students tended to have a marginally greater impact on intention to serve rural communities than the interventions that aimed to recruit more students with a rural background (OR 4.3 versus 4.2), but both strategies still had a statistically significant impact ().
Figure 4 Subgroup meta-analysis between rural background and rural clinical rotation.
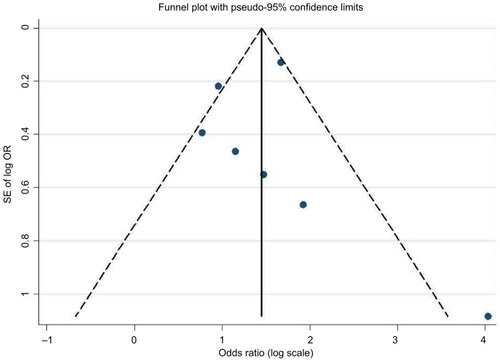
The funnel plot demonstrated quite a symmetrical distribution of the dots (representing the effect size of each study) on either side of the vertical line (representing the pooled estimate). The only exception was found in Johnson and Blink-horn, where the OR seemed to be an outlier.Citation29 The seemingly symmetrical appearance of the plot suggested weak evidence of publication bias. Egger’s test also supported this notion, because the bias coefficient did not significantly deviate from zero (coefficient 0.06, P=0.961; data not shown). The interpretation of Egger’s test was that if the coefficient deviated from zero, with statistical significance, then publication bias could not be ruled out. This point will be discussed further ().
Figure 5 Funnel plot of the seven studies.
Discussion
This review is one of the very first studies in the human resources for health research field that has attempted to estimate the impact of rural experience on the placement of dental graduates in remote and rural areas through a meta-analysis approach, which is commonly accepted in medical and public health fields as the highest level of evidence.Citation35 However, while meta-analysis is widely accepted as the means to obtain the highest level of evidence, the authors are aware that this is dependent on the quality of the individual studies that make up the meta-analysis. The key findings suggested that dental students/graduates with rural experience tended to have an approximately fourfold higher probability of practicing in rural areas than those without rural experience (or about twofold higher possibility if the effect was measured by RR).
As highlighted in the introduction, research on the retention of dental professionals in remote and rural areas is quite sparse relative to similar research regarding medical and nursing professionals.Citation7–Citation10 Therefore, this study helps fill the knowledge gaps on this subject in the field of dental professionals, and the methodology applied serves as an example for health-system researchers of how to gather and analyze evidence to answer real-life policy-research questions.
In addition, this discovery helps provide evidence to support the WHO guidelines for improving the retention of health workers in remote and rural areas.Citation4 The WHO guidelines previously gave the level of evidence in recommendation item A1, “enrolling students with rural background”, and item A3, “clinical rotations in rural areas during studies”, as “moderate” and “very low”, respectively. Moreover, the strength of recommendation for the implementation of these strategies was ranked as “conditional” rather than “strong”.Citation4
Given this study’s findings, it is suggested that enrolling rural students and imposing clinical rotation during study years in the WHO guideline should be regarded as “strong evidence” support. The countries with health-workforce shortages in rural areas should be “strongly” encouraged to implement these strategies.
A range of qualitative literature also shed light on how and why rural experience shaped the attitudes that dental students had toward rural work. For instance, Abuzar et al reported that clinical rotations in rural areas provided “worthwhile” and “enjoyable” experiences for dental students. These experiences also helped dental students appreciate and understand the specific oral health needs of underserved populations.Citation36 Aside from the increase of “rural spirit” in dental students, Mashabi and MascarenhasCitation37 and Formicola and BailitCitation38 suggested that clinical rotations in rural areas had important benefits in increasing basic skills, self-confidence, and speed in dental practice.Citation37,Citation38 Another related advantage of rural clinical rotations was a better understanding of practice management, including the roles of clinical and administrative staff.Citation37
Despite the rigorous review protocol and statistical analyses, this study still encountered some key limitations. Even though three well-known databases were searched, there is a possibility that important studies were missed, particularly those published in domestic journals or in gray-literature databases (so-called citation bias). It should be remembered that only studies published in English were considered for selection. Among the seven selected articles, there was only one study, Thammatacharee et al,Citation34 that was conducted in a country where English is not the official language, and articles from some regions, ie, Europe and Africa, were still missing. Therefore, it is quite likely that language bias exists in the review. Though the funnel plot and Egger’s test suggested weak evidence of publication bias, this does not mean that all sources of publication bias were ruled out. Egger’s test is helpful in detecting publication bias that is derived from the small-study effect, ie, the possibility of including small studies with spuriously inflated estimates in the review, while ignoring those without statistically significant effects, which had a lower possibility of being published.Citation39 However, other causes of publication bias have not been addressed. Finally, to apply the review findings to real-world policy implementation, one must be fully aware that the strategies of enrolling students from rural backgrounds and providing clinical rotations in rural areas are not a silver bullet for tackling the shortage and maldistribution of the health workforce. Other supporting measures, which are beyond the scope of this study, such as the continuous development of health staff, adequate financial incentives, and sufficient outreach support, should also be implemented concurrently. Future reviews and meta-analyses that explore the impact of these mutually supportive measures are recommended.
Conclusion
Enrolling students with rural backgrounds and imposing clinical rotation in rural areas during study years appeared to be effective strategies in tackling the shortage and mald-istribution of dentists in rural areas. The evidence from the meta-analysis revealed that students with rural exposure tended to have a fourfold-higher chance of proceeding to or intending to serve rural populations than those without exposure to rural areas. This phenomenon is most likely due to the fact that rural experience enabled students better to understand the oral health needs of underserved populations and at the same time improved their clinical knowledge and skills. Future reviews and meta-analyses that explore the impact of other supporting measures aside from these strategies are recommended.
Author contributions
RS, NC, and WP designed the study. RS and NC were responsible for data collection and analysis. RS, NC, and AD crafted the first draft of the manuscript. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank all IHPP staff for their unrelenting support and invaluable advice throughout the course of the study. The study was supported by IHPP’s core resources.
Disclosure
The authors report no conflicts of interest in this work.
References
- World Health OrganizationReviewing Progress, Renewing Commitment: Progress Report on the Kampala Declaration and Agenda for Global ActionGenevaWHO2011
- BuchanJCouperIDTangcharoensathienVEarly implementation of WHO recommendations for the retention of health workers in remote and rural areasBull World Health Organ2013911183484024347707
- World Health OrganizationWorking Together for Health: World Health Report 2006GenevaWHO2006
- World Health OrganizationGlobal Policy Recommendations: Increasing Access to Health Workers in Remote and Rural Areas Through Improved RetentionGenevaWHO2010
- JonesMHumphreysJPrideauxDPredicting medical students’ intentions to take up rural practice after graduationMed Educ200943101001100919769650
- DoleaCStormontLBraichetJMEvaluated strategies to increase attraction and retention of health workers in remote and rural areasBull World Health Organ201088537938520461133
- PagaiyaNKongkamLSriratanaSRural retention of doctors graduating from the rural medical education project to increase rural doctors in Thailand: a cohort studyHum Resour Health2015131025889590
- WaskoKJenkinsJMeiliRMedical practice in rural Saskatchewan: factors in physician recruitment and retentionCan J Rural Med2014193939824991859
- TateRBAokiFYRural practice and the personal and educational characteristics of medical students: survey of 1269 graduates of the University of ManitobaCan Fam Physician20125811e641e64823152471
- KuligJCStewartNPenzKForbesDMorganDEmersonPWork setting, community attachment, and satisfaction among rural and remote nursesPublic Health Nurs200926543043919706126
- PetersenPEBourgeoisDOgawaHEstupinan-DaySNdiayeCThe global burden of oral diseases and risks to oral healthBull World Health Organ200583966166916211157
- al-BanyanRAEcheverriEANarendranSKeeneHJOral health survey of 5–12-year-old children of National Guard employees in Riyadh, Saudi ArabiaInt J Paediatr Dent2000101394511310125
- MotohashiMNakajimaIAboshiHThe oral health of children in a rural area of the Lao People’s Democratic RepublicJ Oral Sci200951113113519325210
- Al-HaddadKAAl-HebshiNNAl-Ak’haliMSOral health status and treatment needs among school children in Sana’a City, YemenInt J Dent Hyg201082808520522129
- Niger Ministry of Public HealthImpact of financial incentive measures for doctors, pharmacists and dentistsNiameyMinistère de la Santé Publique2008 French
- GodwinDMHoangHCrocombeLABellEDental practitioner rural work movements: a systematic reviewRural Remote Health2014143282525074243
- KrugerETennantMShort-stay rural and remote placements in dental education, an effective model for rural exposure: a review of eight-year experience in Western AustraliaAust J Rural Health201018414815220690910
- SharifianNBedosCWoottonJEl-MurrIJCharbonneauAEmamiEDental students’ perspectives on rural dental practice: a qualitative studyJ Can Dent Assoc201581f2326679337
- LiberatiAAltmanDGTetzlaffJThe PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaborationBMJ2009339b270019622552
- SandersonSTattIDHigginsJPTools for assessing quality and susceptibility to bias in observational studies in epidemiology: a systematic review and annotated bibliographyInt J Epidemiol200736366667617470488
- von ElmEAltmanDGEggerMPocockSJGøtzschePCVandenbrouckeJPStrengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studiesBMJ2007335762480680817947786
- JüniPWitschiABlochREggerMThe hazards of scoring the quality of clinical trials for meta-analysisJAMA1999282111054106010493204
- BorensteinMHedgesLVHigginsJPRothsteinHRA basic introduction to fixed-effect and random-effects models for meta-analysisRes Synth Methods2010129711126061376
- DaviesHTCrombieIKTavakoliMWhen can odds ratios mislead?BMJ199831671369899919550961
- HayashinoYNoguchiYFukuiTSystematic evaluation and comparison of statistical tests for publication biasJ Epidemiol200515623524316276033
- SimJWrightCCThe kappa statistic in reliability studies: use, interpretation, and sample size requirementsPhys Ther200585325726815733050
- RohraAKPiskorowskiWAInglehartMRCommunity-based dental education and dentists’ attitudes and behavior concerning patients from underserved populationsJ Dent Educ201478111913024385531
- DeCastroJEMathesonPBPanagakosFSStewartDCFeldmanCAAlumni perspectives on community-based and traditional curriculaJ Dent Educ200367441842612749571
- JohnsonGBlinkhornAAssessment of a dental rural teaching programEur J Dent20126323524322904650
- JohnsonGBlinkhornAThe influence of a clinical rural placement programme on the work location of new dental graduates from the University of Sydney, NSW, AustraliaEur J Dent Educ201317422923524127764
- McQuistanMRMohamadAKuthyRAAssociation between dentists’ participation in charitable care and community-based dental educationJ Dent Educ201478111011824385530
- McFarlandKKReinhardtJWYaseenMRural dentists: does growing up in a small community matter?J Am Dent Assoc201214391013101922942149
- McMillanWJBarrieRBRecruiting and retaining rural students: evidence from a faculty of dentistry in South AfricaRural Remote Health201212185522449176
- ThammatachareeNSuphanchaimatRWisaijohnTLimwattananonSPutthasriWAttitudes toward working in rural areas of Thai medical, dental and pharmacy new graduates in 2012: a cross-sectional surveyHum Resour Health2013115324148109
- BurnsPBRohrichRJChungKCThe levels of evidence and their role in evidence-based medicinePlast Reconstr Surg2011128130531021701348
- AbuzarMABurrowMFMorganMDevelopment of a rural outplacement programme for dental undergraduates: students’ perceptionsEur J Dent Educ200913423323919824960
- FormicolaAJBailitHLCommunity-based dental education: history, current status, and futureJ Dent Educ20127619810622262554
- MashabiSMascarenhasAKImpact of community externships on the clinical performance of senior dental studentsJ Dent Educ20117510 SupplS36S4122012935
- PapageorgiouSNPapadopoulosMAAthanasiouAEAssessing small study effects and publication bias in orthodontic meta-analyses: a meta-epidemiological studyClin Oral Investig201418410311044