Abstract
Introduction
Over-the-counter (OTC) drugs are widely available and often purchased by consumers without advice from a health care provider. Many people rely on self-management of medications to treat common medical conditions. Although OTC medications are regulated by the National and the International Health and Drug Administration, many people are unaware of proper dosing, side effects, adverse drug reactions, and possible medication interactions.
Purpose
This study examined how subjects make their decisions to select an OTC drug, evaluating the role of cognitive heuristics which are simple and adaptive rules that help the decision-making process of people in everyday contexts.
Subjects and methods
By analyzing 70 subjects’ information-search and decision-making behavior when selecting OTC drugs, we examined the heuristics they applied in order to assess whether simple decision-making processes were also accurate and relevant. Subjects were tested with a sequence of two experimental tests based on a computerized Java system devised to analyze participants’ choices in a virtual environment.
Results
We found that subjects’ information-search behavior reflected the use of fast and frugal heuristics. In addition, although the heuristics which correctly predicted subjects’ decisions implied significantly fewer cues on average than the subjects did in the information-search task, they were accurate in describing order of information search. A simple combination of a fast and frugal tree and a tallying rule predicted more than 78% of subjects’ decisions.
Conclusion
The current emphasis in health care is to shift some responsibility onto the consumer through expansion of self medication. To know which cognitive mechanisms are behind the choice of OTC drugs is becoming a relevant purpose of current medical education. These findings have implications both for the validity of simple heuristics describing information searches in the field of OTC drug choices and for current medical education, which has to prepare competent health specialists to orientate and support the choices of their patients.
Introduction
Over-the-counter (OTC) drugs and current medical education
OTC drug use is an increasingly important element of everyday life; these drugs are becoming tightly woven into the self-care system for several common health problems.Citation1 Consumers place high value on no-prescription drug therapy. However, self-medicating patients can frequently need assistance from a learned intermediary to assure optimal integration of nonprescription drug therapy into the total care regimen. Clearly, it is important for both patients and health care providers to discuss OTC medications because there is evidence that patients can often be uncertain about the OTC medications that are being consumed. In this sense, one of the aims of contemporary medical education is to prepare medical specialists to meet with professional excellence the health needs of the population they serve and to give adequate support.Citation2
OTC medicines are often perceived as easy to choose by the consumer because they are freely available for self selection. OTC medicines were classified according to the World Health Organization, into 10 categories: analgesics, laxatives, antithrombotic agents, antacids, cough and cold preparations, antihistamines, dermatologicals, throat preparations, nasal preparations, and antidiarrheals.Citation3
In this context of free choice of OTC treatments, how do people make their decisions? Which are the psychological mechanisms and strategies used by subjects to select a specific drug?
In the present paper, we try to identify the kind of strategies and rules – the so called “heuristics”– adopted by subjects in selecting an OTC drug.
The role of heuristics
The term “heuristic” is of Greek origin meaning “to find out” or “to discover”. In the context of cognitive psychology, heuristics serve as guides in problem-solving processes. Heuristics guide problem solvers by helping them simplify choices regarding the numerous immensely complex and imperfectly understood factors that act simultaneously to shape problems.
As guidelines for problem solving, heuristics have proved to be surprisingly robust across a wide array of problem types and problem contexts,Citation4 proving remarkably accurate in both laboratoriesCitation5 and real-life contexts.Citation4 Successful problem solving is a function of how efficiently, rather than how strenuously, a problem solver works,Citation6 and heuristics enhance efficiency regardless of whether the problem is wellCitation7 or ill structured.Citation8 Some studies suggest that heuristics appear most useful in concrete situations.Citation4 In fact, heuristics can help produce results that are comparable to problem-solving strategies which take into account all available information and employ complex computational processes.
Fast and frugal heuristics are particular forms of heuristics developed by Gigerenzer and the ABC Group.Citation4
Fast and frugal approach
This approach is based on a reconceptualization of the rationality in which behavior is evaluated in terms of its adaptivity within the limits of time and knowledge imposed by the situation and the computational power of the decision maker.Citation5,Citation9 To behave adaptively is to act in ways that promote survival and reproduction, whether the actions are consistent with normative rules or not, and cognitive mechanisms are considered rational to the extent that they support such behavior. Todd and Gigerenzer define this concept of ecological rationality as “adaptive behavior resulting from the fit between the mind’s mechanism and the structure of the environment in which it operates”.Citation4 The basic premise of the fast and frugal heuristic approach is that much of human decision making and reasoning can be explained in terms of simple heuristics that operate within the limits of time, knowledge, and computation imposed on the individual. Fast and frugal heuristics do not compute quantitative probabilities or utilities, as in classical decision-making models, because these values require too much computation to serve as practical bases for decision making and often require knowledge (eg, costs, benefits, precise outcomes) that is unavailable in real-world tasks.Citation8 The aim of the fast and frugal heuristic approach is to develop models of cognition that are simultaneously plausible on psychological and ecological grounds, as well as being computationally specific.Citation10 Each heuristic is different, depending on the task for which it is designed and the precise steps involved,Citation11 but three basic features characterize all fast and frugal heuristics: the search rule, the stopping rule, and the heuristic principles for making the decision.Citation12 The “search rule” defines the principle by which the heuristic directs its search for alternative choices and for information to be used in evaluating the alternatives. The search rule must not involve extensive observation or computation. The “ stopping rule” comprises the principles that specify when and how the search procedure should be stopped. The stopping rule is the basis for satisfying processes,Citation13 and thus must operate within the time limits imposed by the task environment. To be robust, a stopping rule is simple and relies on relatively little knowledge and information, which may be scarce in the task environment. The “heuristic principles” for decision making comprise the procedures used to choose from decision alternatives that have either been presented by the task or generated by the decision maker. These are computationally simple, requiring little combination or elaboration of the information obtained through search.Citation12,Citation14
In the last 2 decades, cognitive psychologists have widely argued that people rely on simple strategies when making judgments and simple and complex decisions in many everyday-life situations.Citation15,Citation16 When people are faced with a decision, simple or complex, it is often hard to consider all the available alternatives and to gather and process all the information regarding these options according to a criterion of perfect rationality. The recent literature shows that people generally do not consider all the cues, even when making more complex decisions like how to administer their own savings or how to invest money, or when making decisions in the workplace.Citation9 In fact, in real-life situations such as these, people often make decisions quickly, based on little information and in a very short time. Limited knowledge and time, and urgency, heavily influence the decision-making process of people in several contexts.Citation10,Citation11
In the present paper, we try to evaluate the use of such heuristics in the medical field of OTC drug selection. This field is quite new in the literature, and we attempted to give a new perspective by examining both the information-search patterns appearing in heuristic models and the descriptive validity of information-search patterns, analyzing two very typical scenarios in everyday contexts of OTC drug selection.
Purpose
In this paper, we describe the use of heuristics in the fast and frugal manner which, like those examined by Gigerenzer and his colleagues, are used to determine the selection and the purchase of an OTCCitation11 drug.To do this, we analyzed a dataset of 70 subjects’ information-search and decision-making behavior regarding the intake of these drugs. We addressed two issues: first, using a process analysis of information-search behavior, we examined whether search behavior shows the characteristics of a simple heuristic (ie, few cues searched, stopping rule for search, and lexicographic search order). Lexicographic order is an order function – a way of sorting information. It is generally a simple and useful method of sorting information in a very systematic and regular way. The rules of sorting are those used in dictionaries (from which the name originates). Second, we examined how well a simple heuristics can describe the judgment process and determine the choice.
Subjects and methods
Our analysis was based on semi-structured tests devised in Java language with 70 subjects (range of age: 24–78 years) conducted as part of a larger qualitative study on the meaning of “personal self care” in the autonomous Province of Trento (Northern Italy).Citation17 Research Ethics Committee approval was granted for the study by the Italian ASL (Italian Primary Care Trust) of the Province of Trento. For this study, the 70 participants were purposively sampled from the six main local ASL departments of Trento, varying in terms of locality, size, gender, and age group (). Participants were interviewed face to face in their local ASL offices. The intention was to analyze subjects in a naturalistic environment with the most realistic treatment choice. Tests were conducted by three social scientists trained in qualitative research (two of whom are authors of this article, SR and MM). Participants signed an informed consent to declare their participation to this experiment.
Table 1 Characteristics of participants
Participants were not remunerated. They voluntarily participated in the tasks and showed great enthusiasm, viewing their participation as a contribution to the quality of their medical assistance.
The research project as a whole was developed in two steps (see below).
Test description
The data treated here consist of test results which track information lookups and decisions in a hypothetical situation in which participants were asked to pretend to assume an OTC drug. The computer-administered treatment tasks were performed at different branch locations of the ASL. The interviewer read the instructions to each participant and also explained the aim of the test. Each experimental session lasted approximately 30 minutes. Tests were conducted on a touch-screen-based interface programmed in Java language in order to facilitate the interaction with dynamic information provided by the computer.
Each subject was placed in front of the touch-screen and trained on how to manage each single task. A personal computer ran a Java Virtual Machine which recorded all the data.
Each test consisted of two different phases, each composed of different trials that gave a situation where the subject had pain in their body and they needed to take a drug. The subjects were given the chance to implement a search of different OTC drug features and to identify those most relevant to make their preferred choice.
Test phase 1: pair-wise treatment choice
Subjects were asked to choose 1 of the following 2 scenarios according to their past experience:
Scenario 1 – you have a cold and you decide to take an OTC drug.
Scenario 2 – you have pain (eg, headache, joint pain) in your body and you decide to take an OTC drug.
They were also asked to answer the following question: “In your past experience have you suffered more frequently from cold or pain?”
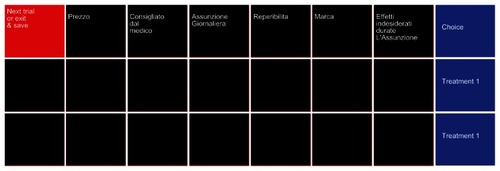
The task began by asking participants to choose between two hypothetical anonymous OTC drugs (for pain or flu in relation to the selected scenario), later extending the number of possible choices to 12. When asked to choose between two treatments, subjects were invited to explore a 6 × 2 matrix displaying in each of the two rows the two alternative treatments (Treatment 1, Treatment 2), and in each column, six treatment features: price, doctor’s advice, daily dose, availability, brand, and side effects. There were no constraints on how participants should look up feature information, even if there was a constraint on the number of possible features looked up. Of the 12 features, they could look up only six. The test began with a black matrix on the screen, initially hiding all the information content. Information popped up in a “flipping cards” fashion when the subject touched the display. Subjects were asked to explore those features that they considered helpful for identifying their preferred treatment (see ).
Figure 1 Test Phase 1 – Pair-wise treatments comparison.
Test phase 2: extended information search – drug market exploration
Participants were asked to explore the medical information they considered necessary for choosing their OTC drug. Drugs were labeled with two widespread disorders: pain and cold. Subjects chose one of these two disorders according their experience. The information provided was arranged in a 7 × 6 matrix, displaying the feature profile of a treatment in each row; namely, price, doctor’s advice, daily dose, availability, brand and side effects for six different treatments typically purchased in Italian pharmacies for pain and cold as reported by ISTAT (Italian National Institute of Statistics) in 2010.
Once again, the test began with a black matrix on the screen, hiding all information content. Pertinent information about a hypothetical “drug market” popped up when subjects touched the display. Participants were instructed to uncover those entries that they considered necessary for making their choices. No restrictions were imposed.
Participants performed one exploration trial and were subsequently invited to continue the test by selecting their favorite treatment from the presented treatment categories.
Results
Characteristics of participants are given in . Out of the 70 participants included in the analysis, eight were aged between 22 and 36 years, 23 were aged between 37 and 49 years, 21 were aged between 50 and 64 years, and 18 were older than 65 years. There were 43 men and 27 women. Thirty-eight out of the 70 were employed, and 20 participants had longstanding illness.
We investigated decision strategies by considering three factors: the overall amount of information that subjects needed for making their decisions, the type of information (features or cues) that they considered before choosing the treatment, and the approach they followed in the information-search process. The results are presented in two parts, one concerning information search and the other concerning the strategies adopted by participants across the JDM process.
Part 1
Information search
In examining the approach followed by participants in exploring medical information, we started by considering how much information a subject needed in order to make a decision. We investigated the information-search processes occurring both in Test Phase 1 (pair-wise treatment comparison) and in Test Phase 2 (extended information search – drug market exploration).
In Test Phase 1, 86% (60 out of 70 subjects) of participants looked at all six pieces of information. In Test Phase 2, participants considered, on average, less than half of the available information (30%, 21 out of 70 subjects), revealing a clear preference for smaller information sets to act upon. Subjects probably focused on those subsets of medical products that they were familiar with and used, without paying attention to the differences and similarities between the drugs.
The medical task with the context of “Cold” was performed by 36 subjects, whereas the medical task with the context of “Pain” was performed by 34 subjects. A balance between the two situations was maintained during the experiment.
For the Cold group, the cue of highest interest was “side effects” (in average 41% of the available information was gathered), followed by “doctor’s advice”. The object of highest interest by far was Aspirin (in average 36% of the available information was gathered).
For the Pain group, the cue of highest interest was again “side effects” (in average 35% of the available information was gathered), followed by “doctor’s advice”. The objects of highest interest by far were Moment and Voltaren (in average 33% of the available information was gathered).
These main differences are also visible in the analysis by sex and age. The women, but not the men, considered the availability of the product to also be important.
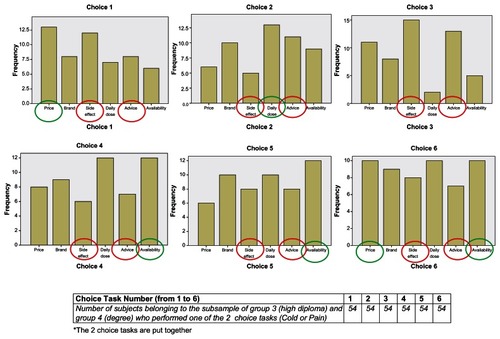
No differences were found in the analysis by sex: in the male group, the cues of highest interest were “side effects” (average 27%, 12 out of 43 subjects) and “doctor’s advice” (average 19%, 8 subjects out of 43). In the female group, the cues of highest interest were “side effects” (average 21%, 6 out of 27 subjects) and “doctor’s advice” (average 17%, 5 out of 27 subjects). Similarly, analysis by age group reflects that “side effects” and “ doctor’s advice” were the cues of highest interest independently of age. Finally, in relation to the variable “education”, the cues “side effects” and “doctor’s advice” always represented the most important information requested for the school attendance group 1 (elementary school) and group 2 (junior high school), whereas for group 3 (high school) and group 4 (degree), these cues represented important information ( marked in red), but the cues’ exploration was wider in the different trials, and other cues (price, daily dose, availability) ( marked in green) were considered relevant in the process of choice, as shown in .
Figure 2 Histograms of clicked cues in school attendance groups 3 and 4 in the first six choices.
Information search over time
In Test Phase 1, participants sequentially explored, at most, six different pieces of information dealing with the treatment features in 65 trials. Therefore, we analyzed data according to the 12 exploration steps denoted by tCitation1 … tCitation12. This sequential analysis revealed results consistent with those represented in and : information concerning advice, side effects, and daily dose are looked up first (see the bold numbers in ).
Table 2 Frequency of clicked cues and objects for Cold context
Table 3 Frequency of clicked cues and objects for Pain context
Table 4 Information exploration over time (t) in Test Phase 1 for Cold group
In this part, we focused the analysis on the type of illness only (cold or pain) because the number of analyses is quite high and the aim of this paper is to highlight the use of fast and frugal heuristics and how they work in people’s minds. The differences using by the analysis shown the independent variables (eg, for the school attendance groups) were not so impressive; these will be described specifically in a future paper.
In , we present the means computed per trial. With regards to the Cold group, reveals that at time (t)1, both “side effects” and “doctor’s advice” were looked up in 41% of the cases. At t2, the “side effects” were looked up in 44% and “doctor’s advice” in 35% of the cases. At t3, “side effects” were looked up in 30%, and “daily dose” in 20% and “doctor’s advice” in 29% of the cases. With regards to the Pain group (), at t1, both “side effects” and “doctor’s advice” were looked up in 43% of the cases. At t2, “side effects” was looked up in 41% and “doctor’s advice” in 37% of the cases. The same preferences as for the Cold group were maintained at t3 (side effects = 21%, doctor’s advice = 33%, daily dose = 18% of cases). This information search analysis revealed that within the first three times (t1, t2, and t3), “side effects” and “doctor’s advice” were the most explored treatment features. From t4 onwards, no strong preference for any of the remaining features appeared. During t1, t2, and t3, the preferred exploration path was side effects ≥ doctor’s advice ≥ daily dose. shows the aggregate view looking at the total number of cue lookups in the total pool of all participants over the 12-step time path for both groups. In both groups, the cues “side effects” (70% for the Pain group, 84% for the Cold group) and “doctor’s advice” (70% for the Pain group, 81% for the Cold group) were the most requested, followed by the question how often the drug must be taken. The subjects from the Pain group were less active in their search for information.
Figure 3 Information gathered for each cue over time in Test Phase 1 for Pain group (on the left) and Cold group (on the right).
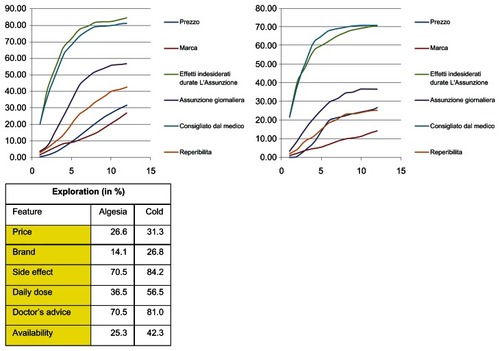
Table 5 Information exploration over time (t) in Test Phase 1 for Pain group
We estimated a Markov transition matrix with empirical probabilities of moving from one treatment feature to another in the six-step information-search process (see and ). A Markov analysis looks at a sequence of events, and analyzes the tendency of one event to be followed by another.Citation18 A Markov process is useful for analyzing dependent events; that is, events whose likelihood depends on what happened last.Citation19 So, a Markov chain is a random process with the property that the next state depends only on the current state. Using this analysis, you can generate a new sequence of random but related events, which will look similar to the original. With respect to the Pain group, at the beginning (start position) the features most likely to be explored were “side effects” or “doctor’s advice” (43%). The feature after risk most likely to be explored is “price” (37%) and again “side effects” (12%). The next feature most likely to be explored after price is “brand” (36%) and then “availability” (18%) (see the bold numbers in ).
Table 6 Transition probabilities (in%) among features observed in Test Phase 1 in Pain group
Table 7 Transition probabilities (in%) among features observed in Test Phase 1 in Cold group
Regarding the Cold group, at the start position, the features most likely to be explored were the same: “side effects” or “doctor’s advice” (41%). The feature after risk most likely to be explored was “price” (46%) and then “brand” (36%) and, in the next step, again, “side effects” (40%) (see the bold numbers in ).
Transition probabilities analysis between features shows that subjects in both groups normally start by looking either at doctor’s advice or side effects and that gathering information cue-wise is quite common (see the high values in the main diagonal).
Payne’s analysis of information exploration
Payne et alCitation20 proposed an approach to information search to explain the decision process of people in different contexts. They identified two types of exploration paths: feature-wise and global-wise. A feature-wise path corresponds to a subject focusing on just one feature and exploring it across treatment options. A global-wise path corresponds to a subject exploring features belonging to just one treatment at a time.
Data collected in Test Phase 2 showed that 62% of subjects in the Pain group (23 out of 35) and 93% (33 out of 36) of subjects in the Cold group adopted a treatment-wise path; they focused their attention on information pertaining to a single treatment at a time. Protocol analysis revealed that most of those participants began their explorations based on the treatments they had already experienced in real life (eg, Moment for Pain or Aspirin for Cold). The other participants explored the available information by adopting mixed strategies: some of them exhaustively explored the information dealing with risk by adopting a cue-wise approach, whereas others gathered information across all the treatments without revealing a predominant approach.
Overlapping information index and order preservation index
We investigated the path of information search to answer the following questions: Did subjects look at identical information for both treatments? Did subjects explore treatment features by following a well established common order?
We adopted a within-subject approach through introducing two indices characterizing participants’ information search. We noticed that in our study, participants did not necessarily collect overlapping information on different treatments before making choices. When considering treatments A and B (Test Phase 2), participants did not check the same features for A and B respectively before choosing. Such measures of systematic search, as the two indices we introduced, are not commonly mentioned in the literature, although they are certainly relevant for describing information usage and decision processes.
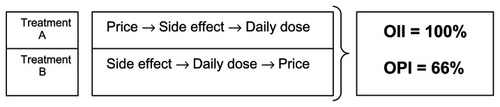
The two specific measures are: the overlapping information index (OII) and the order preservation index (OPI). OII is defined as the percentage of identical features looked up for both treatments across participants. OPI indicates the percentage of overlapping features explored in identical order. shows the two types of measures.
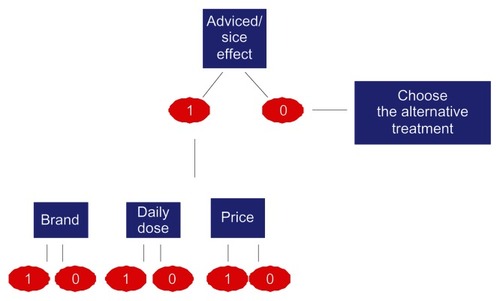
Figure 4 Decision heuristic predictions tree.
As shown in , the OII is 100%, since three out of the three features are looked up for both treatments. For both examples, the OPI is equal to 66.6%, because two out of the three overlapping features are looked up in the same order. Participants were classified according to their OII in two groups:
Figure 5 Overlapping information index (OII) and order preservation index (OPI) measures.
High overlapping information index (HOI) group – participants show an OII higher or equal to 50%;
Low overlapping information index (LOI) group – participants show an OII lower than 50%.
OPI and OII were highly correlated (r = 0.98), which means that participants belonging to the HOI group preserved their exploration order across explorations and focused their attention on a smaller set of medical features. This fact suggests that the selection of the considered information set is connected with the exploration approach and with the treatment representation space and, thus, with the decision mechanism. highlights that a part of our sample looked for coincident information for both treatments and followed the same sequential order across cues.
Table 8 Subjects with the highest overlapping information index and order preservation index calculated in Test Phase 1 (Cold group)
Data from the Pain group and from the Cold group are speculative. shows that the more subjects gathered identical information from both treatment options, the more closely they preserved the same exploration order. The exploration order covers an important role in the process of treatment choice: as much higher is HOI, as much higher is the OPI and lower the number of explored features. This reveals a preference for frugality, and thus shows the use of one cognitive heuristic (namely, the “Less is more” heuristic). Individuals who consider many of the cues often perform worse than individuals who recognize fewer of the cues, who rapidly focus their attention on only the relevant elements. Citation16 Thus less searched information is quite often associated with a more structured exploration both for typology and for modality.Citation11
The aggregated data () shows relationships between the participants’ considerations of specific medical features and their decisions in the treatment task. Data reveal that across all the subjects’ decisions in the Pain group, price was selected in 43 cases for both treatments and was discriminating (as different values) in 23 cases. In 17 of these cases (73%), the participants preferred the cheaper treatment. The brand of the treatment was selected for both treatments in 20 cases and was discriminating in nine of these. In five of these cases (55%), the participants preferred the unbranded generic drug. In the Cold group, subjects more often explored the information globally: price was selected 58 times and was discriminating in 47 (81%) cases, whereas brand was selected in 48 cases and was selective in 18 of these (37%).
Table 9 Relationships between information search and decision in Test Phase 1 for Pain group and Cold group
Part 2
The judgment process: a within-subject analysis
To understand to what extent a decision tree is able to capture a single subject’s choice rule, we introduce some definitions. We define the “cue profile” of treatment as a binary vector of 1s and 0s according to whether cue values are “positive” or not and ordered by the sequence: side effects, doctor’s advice, daily dose, availability, brand, and price. Based on the fast and frugal heuristic model, treatment features were all transformed to binary values to simplify their comparison.Citation8 The convention for assigning the values 1 or 0 to a cue reflects the preferences revealed by participants in the interview. If, for instance, “side effects” was medium or low, it was assigned the value 1. Similarly, if “availability” was medium or short, its value was 1, and if “price” and “daily dose” were medium or low, they were also assigned the value 1. If the treatment was suggested by a physician, this cue is assigned a 1, otherwise 0, and if the treatment was not a generic drug, then this cue is assigned a 1, otherwise 0.
The heuristic that best modeled our data lexicographically examines only the one cue that was explored most, namely risk, and processes all the remaining cues by means of a tallying rule. Tallying is a heuristic that can be described by a linear model with weights equal to one for each treatment feature. In this context, tallying means counting the number of 1s for both treatments and choosing the treatment with a higher score. For instance, if treatment A has a cue profile (011111) and B has a cue profile (100000), then B is preferred because the first cue is treated lexicographically. As an example, if A is a treatment with a cue profile (100101) and B is a treatment with a cue profile (100100), treatment A is chosen over treatment B because its profile contains more 1s after the first entry.
The tree in predicts about 78% of the observed treatment decisions in the task on Phase 1 and 2. One of its key features is that for most subjects there is no compensating trade-off for high-risk treatments or for nonsuggested treatment by an expert. High-risk treatments and nonsuggested treatment were eliminated from consideration in the lexicographic formulation depicted in . The second key feature is that beyond this lexicographic step, participants adopt a simple tallying rule that counts 1 for each cue value that matches their system of preferences, or otherwise 0, and choose the treatment with the higher score. In other words, rather than weighting different features differentially, the model suggests that subjects simply count the number of features to determine which treatment dominates another.
Discussion
The aim of this study was to investigate how subjects make medical decisions for selecting an OTC drug. We analyzed participants’ behavior in an information-search task and examined whether information search was simple and whether a heuristic that predicts a simple decision-making process was also accurate at describing information search. For this study, we designed naturalistic environments based on two health problems commonly experienced by people: pain and cold. The study consisted of two tests focused on the building blocks of a decision process; namely, information search and decision rule. In Test Phase I we let participants choose between two treatments; they to looking up at most six possible feature variables. In Test Phase II were limited, by contrast, they had to choose between six types of treatment and could consult all 36 pieces of information available.
We observed that in Test Phase II they consulted less than half of the information at their disposal. Fast and information- frugal heuristics explained the information search and decision behavior of most participants, thus reflecting a no compensatory-lexicographic hierarchy of features (side effects, doctor’s trust, and drug frequencies, in that order). The first two features were systematically explored: side effects (70% of the time in the pain-virtual situation; 84% of the time in the cold-virtual situation) and doctor’s advice (70% of the time for the pain-virtual situation; 81% of the time for the cold-virtual situation). A simple combination of a fast and frugal tree and a tallying rule predicted more than 78% of subjects’ decisions.
A significant proportion of participants (93% in the Cold group, 62% in the Pain group) used an HOI strategy and explored a specific set of few overlapping features for pairs of treatment alternatives. Trust was a mediator for strategy selection for a treatment choice. This provides new empirical insight on people’s search and use of information when making simple medical decisions. Both the lexicographic and the tallying strategies have been extensively examined by the ABC group and both are considered simple in their categories, namely trees and linear models,Citation21,Citation22 although the lexicographic rule is more frugal in terms of requiring few resources. The tallying rule is less “finely tuned” than the lexicographic one, because it does not discriminate between profiles having the same number of 1s, independent of where in the cue profile the 1s are. Furthermore, the tallying rule quite often makes the same choices as the lexicographic one.
Simple heuristics originally introduced by Gigerenzer et alCitation4 have been recognized for their precise specification of information search–stop, decision-making processes as well as their psychological plausibility. This study broadened the body of evidence indicating that simple heuristics can capture human decision making and influence relevant context as health and medical decisions.
Conclusion
This is an initial study, and the present findings require further explanation. First, it might be possible to compare our results investigating the role of other features which can be discriminatory in the information-search process (eg, to more deeply investigate the role of the participant’s trust in the general practitioner’s level of expertise, to better explore the influence of demographic differences like sex, age group, and education level in the decision making process). Second, the information-search process could be evaluated with other new scenarios (eg, using only unbranded generic drugs, evaluating only one brand, exploring the level of loyalty for some brands). Evidence suggests that people tend to search for consistent information to support their choices, perhaps to increase confidence in their decisions, especially when they have no great familiarity with the type of information.Citation23 In addition, as Pineda et alCitation24 have found when a task is perceived to be important or when the decision maker perceives him/herself to be effective, greater information is searched. Third, it would be possible to investigate the influence of the packaging and the labeling (eg, colors, shapes, design) in the process of choice in order to investigate how the heuristics work with these specific cues and give new hints for the pharmaceutical market.
There are several avenues for future investigation which have been highlighted not only for the cognitive research and the decision-making literature but also for medical education and practice. First, the quantity and quality of information have the potential to influence the ability of individuals to judge and participate in decisions concerning their treatment.Citation25,Citation26 The doctor, being the first who knows the health status of his/her patients, is the one who initiates the transmission of necessary information and the correct use and choice of medication.Citation2 The other health specialists (eg, the pharmacist) at the time of dispensing should continue the flow of information initiated by the physician during the consultation, ensuring that the guidance given was well understood by the patient. Second, the training to cooperate, along with the entire team of health professionals, will help to overcome problems of communication and obstacles, so that the patient, feeling secure and confident, will more readuly accept information and proposals, keeping higher expectations regarding treatment, and this will make more accurate a fast and frugal strategy of choice.Citation27 Finally, future researchers in medical education should work together with cognitive and decision-making researchers not only to identify the process and the rules behind the subjects who select an OTC drug but also to collaborate with public health policy makers who could focus on strategies to improve the education of society regarding the appropriate use of OTC drugs.
Acknowledgments
We want to thank the ASL of Trento and the Board of Executives of Cassa Rurale Giudicarie Valsabbia Paganella for their full support for conducting this research. We also thank Marcel Jentsch from the Max Planck Institute for Human Development of Berlin for his valuable help in programming and designing interactive interfaces.
Disclosure
The authors declare that they have no competing interests.
References
- CovingtonTNonprescription drug therapy: issues and opportunitiesAm J Pharm Educ200670613717332863
- LeeMANonprescription medicines and the North American Pharmacist Licensure ExaminationAm J Pharm Educ200670613817332864
- WHOWHO Drug Information200317145183
- GigerenzerGToddPMfor the ABC Research GroupSimple Heuristics That Make Us SmartOxfordOxford University Press1999
- OrbellJDawesRMA cognitive miser theory of cooperator advantageAm Polit Sci Rev199185515528
- AnokhinAPAge increases brain complexityElectroencephalogr Clin Neurophysiol19969963688758971
- AndersonJRProblem solving and learningAm Psychologist1993483544
- ChiMTHGlaserRProblem solving abilitySteinbergRJHuman Abilities: An Information Processing ApproachNew YorkWH Freeman1985227250
- TietzRSemi-normative theories based on bounded rationalityJ Econ Psychol199213297314
- SlegersDWBrakeGLDohertyMEProbabilistic mental models with continuous predictorsOrgan Behav Hum Decis Process2000819811410631070
- GigerenzerGBounded rationality: models of fast and frugal inferenceSwiss J Econ Statistics1997133201218
- ToddPMFast and frugal heuristics for environmentally bound mindsGigerenzerGSeltenRBounded Rationality: The Adaptive ToolboxCambridge, MAMIT Press20015170
- RichardsonRCHeuristics and satisfyingBechtelWGrahamGA Companion to Cognitive ScienceOxford, UKBlackwell1998566575
- MartignonLSchmittMSimplicity and robustness of fast and frugal heuristicsMinds Machines19999565593
- EngelCGigerenzerGHeuristics and the lawDahlem workshopCambridge, MAMIT Press2006 report 94
- GilovichTGriffinDKahnemanDHeuristics and Biases: The Psychology of Intuitive JudgmentCambridge, UKCambridge University Press2002
- Max Planck Institute for Human DevelopmentAdaptive Behavior and Cognition Available from: http://www.mpib-berlin.mpg.de/en/forschung/abc/index.htmAccessed Dec 23 2010.
- ResnickSIAdventures in Stochastic ProcessesBostonBirkhäuser1992
- TaylorHMKarlinSAn Introduction to Stochastic Modeling3rd edNew YorkAcademic Press1998
- PayneJWBettmanJRJohnsonEJFast and frugal heuristics: the tools of bounded rationalityKoehlerDHarveyNHandbook of Judgment and Decision-MakingOxford, UKBlackwell20046289
- MartignonLHoffrageUFast, frugal, and fit: simple heuristics for paired comparisonTheory Decis2002522971
- KatsikopoulosKVMartignonLNaïve heuristics for paired comparison: some results on their relative accuracyJ Math Psychol200650488494
- OskampSThe relationship of clinical experience and training methods to several criteria of clinical predictionPsychol Monogr Gen Applied196276128
- PinedaRCLernerLDMillerMCPhillipsSJAn investigation of factors affecting the information-search activities of small business managersJ Small Bus Manag1998366071
- RoumieCGriffinMROver-the-counter analgesics in older adults. A call for improved labeling and consumer educationDrugs Aging2004248549815182214
- EastonKComplementary medicines: attitudes and information needs of consumers and healthcare professionalsSydneyNational Prescribing Service Ltd2007
- ClarkDLaytonDShakirSMonitoring the safety of over the counter drugsBMJ200132370670711576964