
Abstract
Background
Carbon dioxide therapy, better known as carboxytherapy, relates to percutaneous infusion of medical carbon dioxide with therapeutic approaches, and its use in the treatment of localized fat has demonstrated good results. Gynoid lipodystrophy, also known as cellulite, affects 80%–90% of women after puberty, especially in the buttocks and thighs. Its etiology is complex and involves multifactorial aspects. Its treatment and evaluation require the use of new technologies (more effective and low-cost approaches). The objective was to investigate the effectiveness of carboxytherapy in the treatment of cellulite in the areas of buttocks and posterior thigh.
Patients and methods
Ten women, 29±6.1 years, were selected and all of them received eight treatment sessions, with an interval of 7 days between sessions. Standardized digital photographs were used to assess the severity of cellulite, and panoramic images were collected by ultrasound diagnosis. The evaluations were performed before the first treatment (baseline) and 7 days after the last treatment session of carboxytherapy.
Results
After the treatment, there was a significant reduction (P=0.0025) of the cellulite from degree III to degree II, and this improvement had correlation with the improvement in the organization of the fibrous lines and the disposal of adipose tissue lines of the treated regions observed through the panoramic ultrasound images diagnosis.
Conclusion
Carboxytherapy is an effective technique of treatment of cellulite in the buttocks region and posterior thighs of healthy women.
Introduction
Cellulite refers to a change that gives the skin a wavy and irregular appearance, and it affects 80%–90% of women after puberty. Numerous treatments have been proposed such as balanced diet, physical activity, massage, topical products, radiofrequency, therapeutic ultrasound, and light emitting diode therapy, among others.Citation1 Carbon dioxide (CO2) therapy, commonly known as carboxytherapy, refers to the administration of CO2 with therapeutic proposals. The technique originated in France in 1932, and originally the treatment was carried out percutaneously (through the skin) by the so-called heated carbonated water baths or the application of water-saturated CO2 directly to the skin of patients. The technique was used for arteriopathy and ulcer treatments.Citation2,Citation3 The results encouraged further studies, leading to the expansion of indications of new treatments. After the development of new technologies, the application was no longer topical and involved passing the CO2 to be infused directly into the subcutaneous tissue, ensuring faster and better results. Sequential studies described the effectiveness of the carboxytherapy treatment of localized adiposities; demonstrated measurable reductions in circumference regions of the abdomen, thigh, and/or knee; and showed histological evidence of the effect of gas leakage, showing its possible lipolytic effects.Citation3,Citation4 Ferreira et alCitation5 described the increase in collagen remodeling induced by intradermal injections of CO2. In another study, Abramo et alCitation6 showed that after the controlled infusion of CO2, vasodilation of the microcirculation skin was observed, accompanied by an increase of peripheral blood flow and an increase in skin temperature at the injection site (on average 3.48°C). Cellulite affects, especially, the buttocks and thighs; its etiology is multifactorial and involves complex issues, and its treatment and evaluation require the use of new methodologies.Citation7–Citation11 The lipolysis caused by carboxytherapy seems to be caused by temperature increase and local blood flow and have been demonstrated in previous studies; however, clinical studies are still required, with good analysis techniques that prioritize their effects on cellulite.Citation2–Citation6
This study aimed to verify the effectiveness of controlled infusion of CO2 in the treatment of cellulite in gluteal and posterior thigh bilaterally.
Materials and methods
This study began with a sample of 12 candidates and finished with ten of them with an average age of 29±6.1 years and body mass index (BMI) of 25.5±3.3 kg/m2. Inclusion criteria were healthy women, aged 20–35 years, BMI <29.9 kg/m2, with regular menstrual cycle, and presence of cellulite of gluteal and posterior thigh bilaterally as classified in degrees of severity II and III as in the current classification of celluliteCitation12.
This study was approved by the Research Ethics Committee: União das Instituições de Serviço, Ensino e Pesquisa – UNISEPE (CAAE: 02242112.9.0000.5490) and all subjects signed informed consent forms. The treatment was performed in the Clinical Laboratory of the Center for Education and Advanced Training CEFAI (Amparo, SP, Brazil). Volunteers were excluded if they were in aesthetic treatment; had had some kind of treatment in the gluteal region and thighs for a period leading up to 6 months before the start of this study; if they were pregnant or had had a recent pregnancy (<6 months); if they had cardiovascular problems, metabolic disorders, respiratory disorders, immunosuppression, kidney and liver failure, and skin lesions at the treatment site; or if they had diabetes mellitus. In assessing weight and height, the volunteers wore only underwear without shoes.
A classical mechanical stadiometer (model 110 CH; Welmy, SP, Brazil) was used. The BMI was evaluated by applying the formula BMI = weight in kilograms divided by the square of the height in meters (kg/m2).Citation13–Citation15 Body fat percentage of each volunteer was measured with Biodynamics (Model 310E; TBW, SP, Brazil).
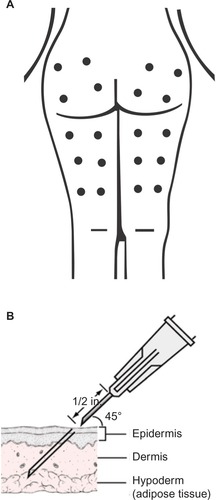
All volunteers received directions about the treatment steps and procedures to be performed. The treatment protocol consisted of eight sessions with an interval of 7 days. The evaluations were performed before the first treatment (baseline) and 7 days after the last treatment session. The total time between the baseline and the posttreatment reevaluation was ~2.5 months. After analysis of the area, ten points were selected for the infusion of CO2 (four in the gluteal area and six in the posterior thigh) as shown in . The treated areas were inspected and constantly monitored during all sessions. With a proper pen, points equidistant from each other were marked, 12 cm apart from each other, in places where the infiltration of CO2 was held. The antisepsis was performed with alcoholic chlorhexidine at 0.5%. At each selected points, 80 mL of gas with a flow rate of 80 mL/min was infused. The needle was positioned at 45° (inferior angle), and a subcutaneous puncture was made with a depth of ~10 mm ().
Figure 1 (A) Points of CO2 infusion; (B) position and angulation of needle placement for infusion, depth of ~10 mm (30 G × 1/2 inch size needle).
After the application of the gas, the skin of the treated area was inspected. The equipment used in this study was ARES Car-boxytherapy (IBRAMED, Indústria Brasileira de Equipamentos Médicos EIRELI, ANVISA 10360310032), and the medicinal CO2 used was from White Martins Gases Industriais Ltda (São Paulo, Brazil). Cellulite grades were determined by clinical inspection of the patient’s skin, and standardized digital photographs with a digital camera (Canon EOS Rebel T3i, Canon USA Inc., Melville, NY, USA) were taken at baseline and 7 days after the proposed treatment. All patients were photographed in standing positions in three views: rear view, right side, and left side. The focus of the image was in the gluteal cleft with a focal length of 1 m, and the muscles of the photographed areas were relaxed. Seven days after the last CO2 infiltration, new photographs were taken. The images were offered to independent evaluators together with the criteria for the verification aspect of the severity of cellulite. The stage of severity of cellulite according to what is generally accepted was used. Nürnberger and Müller describe different grades or stages of severity based on clinical presentation from 0 (zero) to III (three); 0= there is no alteration of the skin surface (visible without changes); I= the skin of the affected area is smooth while the subject is standing or lying, but the alterations to the skin surface can be seen by pinching the skin or with muscle contraction (visible changes with skin clamping or muscle contraction); II= the orange peel aspect of the skin or mattress appearance is evident when standing, without the use of any manipulation of the skin pinching or muscle contraction (visible without manipulation); and III= the alterations described in grade or stage II, are present together with raised areas and nodules (visible changes associated with nodules).Citation12 To minimize trends, reviews of the photographs were partially blind, ie, the evaluators received them in pairs without identifying which one represented the subjects before or after treatment. All the volunteers participating in the study underwent diagnostic ultrasound that was performed before and after the proposed treatment. All the volunteers underwent diagnostic ultrasound examination using a linear transducer (frequency 6–18 MHz) (MyLab™25 Gold; Esaote, Italy), and VPan software (Esaote, Italy) was used for the construction of panoramic images. All panoramic images were taken in the standing position. The probe was slipped at a slow and regular speed in the distal/proximal direction along the areas. Panoramic images were analyzed qualitatively considering the hyperechoic areas. Bright echoes represent highly reflective structures (white = dermis and fibrotic septa) and hypoechoic areas represent sparse echoes, reflection, or intermediate transmission (gray = adipose tissue and skeletal muscle).
The paired Student’s t-test was used for statistical analysis, with an alpha level of 5% (P<0.05) being considered significant.
Results
The volunteers were numbered 1–10, and evaluations were performed at baseline and 7 days after the last treatment session. shows the anthropometric values before and after the infusion of CO2. There were no significant changes in anthropometric measures of weight (P=0.10), BMI (P=0.20), and body fat percentage (P=0.73), at baseline and after the treatment.
Table 1 Mean and standard deviation of the average of our patient population (age, body weight, BMI, and body fat percentage) at baseline and after treatment (7 days after the last carboxytherapy session).
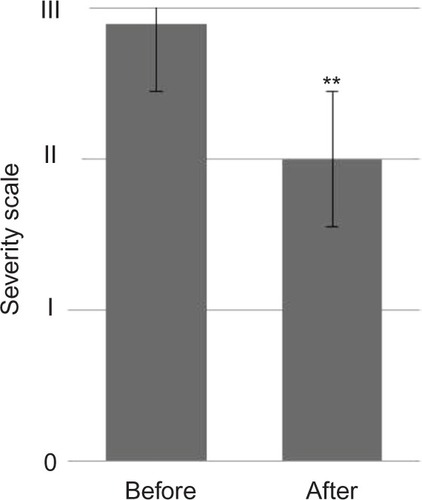
shows a statistically significant reduction (P=0.0025) in the aspect of cellulite; the images were handed over to three independent evaluators, and assessments of the photographs were partially blind according to generally accepted classification of cellulite.
Figure 2 Cellulite degree evaluation according to generally accepted classification of cellulite, baseline (before) and 7 days after the last carboxytherapy session. Note: **P=0.0025.
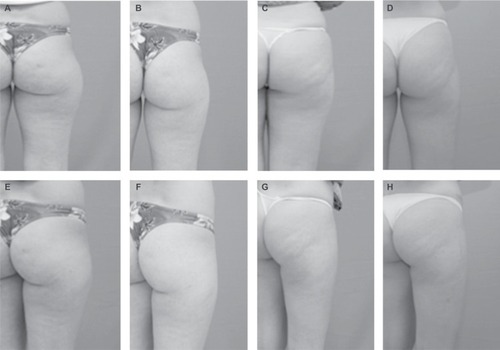
shows comparative photographic register of the aspect of cellulite at baseline and 7 days after the last carboxytherapy session.
Figure 3 Comparative photographic register of the aspect of cellulite. Notes: (A, C) Rear view of gluteus and posterior right thigh at baseline; (B, D) rear view of right gluteus 7 days after the last carboxytherapy session; (E, G) right side view at baseline; and (F, H) rear view of the right gluteus after the last session of carboxytherapy.
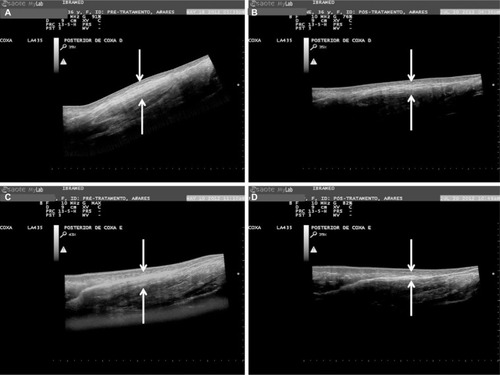
In the panoramic image analysis performed by the ultrasound diagnosis, reduction of adipose tissue lodged between the skin and the muscles of the treated regions was verified, as seen in and . Qualitative analysis describes morphological improvement with respect to the subcutaneous tissue, fibrotic septa, and aspects of the dermis-related cellulite. The morphological improvement with respect to the subcutaneous tissue, fibrotic septa, and associated dermis aspect of the cellulite can also be seen.
Figure 4 Comparative panoramic images of gluteal region.
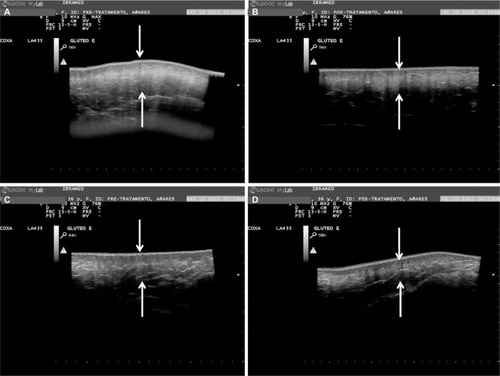
Figure 5 Comparative panoramic images of the posterior thigh.
Discussion
Cellulite is a multifactorial disorder and has a high prevalence in young adult women and despite no morbidity causes great dissatisfaction and negative influence on quality of life.Citation1 The pathophysiology of cellulite was described as an aesthetically unpleasant disorder for most women after adolescence. It is a complex problem that includes changes involving the microcirculation, lymphatic system, extracellular matrix, and adipocytes. It affects certain body areas with more emphasis, such as thighs and buttocks.Citation8 Studies also describe the pathophysiology involving a hyperactivity of fibroblasts stimulated by estrogen, which increases the synthesis of glycosaminoglycans and collagen that increase interstitial osmotic pressure and water retention. A decrease in the capillary osmotic pressure in relation to the interstitial osmotic pressure generates edema and reduction in drainage with subsequent hyperpolymerization and formation of micronodules and fibrosclerotic collagen. Symptoms include edematous adiposity, incipient cellulite, or changes in the skin relief measured by the clinical severity.Citation9,Citation16,Citation17 Adipose tissue can be divided anatomically into two layers by a layer of fibrous tissue called Camper’s fascia.Citation8 The areolar layer has fibrous septa arranged in a peculiar vertical architecture that connect the dermis filled by large globular adipocytes; below, the lamellar layer septa has more horizontal axis and the fat lobes are flattened. Adipocytes are specialized cells in the storage of fats.Citation8–Citation11,Citation16–Citation19 In 2004, it was demonstrated for the first time that the hypodermic infiltration of CO2 as an alternative measure to be associated with liposuction procedures was effective in treating localized adiposity or skin irregularities, resulting from the surgical procedure. Since then, the method has been used with increasing frequency in the treatment of different forms of lipodystrophies, as well as in aesthetic medicine. In this area, its main indications are in fighting cellulite in localized fat and sagging.Citation20 Other studies show that controlled administration of medical CO2 into the subcutaneous tissue induces hypercapnia and decreases local pH, which elicits a strong vasodilator response through the relaxation of the pre-arteriolar smooth muscle on the site.Citation2,Citation6,Citation25 Histological features in the repair process showed the proliferation of newly formed small blood vessels and fibroblasts.Citation21 The tissue stretching during infusion induces a subclinical inflammation, which triggers the repair and tissue regeneration processes that induce the activation of macrophages, fibroblasts, and endothelial cells that stimulate neovascularization and remodeling of the extracellular matrix. Among the diseases that may need carboxytherapy are peripheral artery disease and microangiopathy, psoriasis, varicose, and diabetic ulcers. This technique has also been frequently used for the treatment of cosmetic changes such as localized fat, cellulite, facial skin rejuvenation, alopecia, dark circles, and striae.Citation2,Citation4,Citation20,Citation22–Citation26 In a study by Abramo et al,Citation6 after the infusion of CO2, there was an average temperature increase of 3.48°C in the skin of the treated site. In addition, skin biopsies before and after treatment were evaluated by histology, and the authors observed that the diameter of the vessels increased by 3.24 times after treatment. Brandi et alCitation4 described the effectiveness of carboxytherapy in the treatment of localized fat through measurable reductions in the circumference regions of the abdomen, thigh, and/or knee and showed histological findings of the effects of CO2 gas infiltration on the subcutaneous adipose tissue and their possible lipolytic effects. Corroborating these findings, a standardized study involved 15 volunteers subjected to car-boxytherapy sessions on the anterior wall of the abdomen for 3 consecutive weeks. Two sessions per week at intervals of 2–3 days between each session were made, with infused fixed volume of 250 mL of CO2 per 100 cm2 of treated surface. Tissue biopsies were collected before and after treatment and analyzed by flow cytometry, which showed a significant reduction in the number and change in the morphology of the adipocytes in the treated area.
The objective of the study was to verify the effectiveness of carboxytherapy in the treatment of cellulite. During the treatment period, there were no significant changes in the body weight or BMI, as shown in Table 2. Photographic images captured in a standardized manner were analyzed by three independent evaluators and were partially blind. The visual inspection of photographic records of the areas treated with carboxytherapy showed statistically significant (P=0.0025) changes regarding the aspect of improvement of the degree of severity, as shown in . All volunteers showed improvement of skin appearance after carboxytherapy sessions, suggesting decreased tensile forces on the skin and possible redistribution of vertical forces (vector forces) in the septum (). With regard to the safety of the carboxytherapy treatment, important studies report that the use of CO2 for contrast angiography attests to the safety of this gas and have shown that it is not likely to promote clots. CO2 can be used with intravascular bolus injections of up to 100 mL and continuous flows between 20 and 30 mL/s without adverse reactions.Citation27 In this study, 80 sessions with carboxytherapy were performed and no volunteer had any sort of significant adverse effects, but reported only mild transient discomfort, tolerable during treatment. One volunteer had two small bruises that resolved spontaneously, which suggests that carboxytherapy can be a safe technique. The treatment was tolerable for all the patients.
Noninvasive assessment techniques have been used to evaluate the cellulite and its posttreatment results, among which stand out the magnetic resonance imaging (MRI) and diagnostic ultrasound. Researchers, using microimages of the MRI, correlate the anatomy of the subcutaneous tissue to the typical changes in the cellulite at different degrees of severity;Citation28 other researchers also used MRI to study the cellulite and its treatment with lymphatic drainage.Citation29 However, the development of software that allows the use of panoramic images captured by diagnostic ultrasound is more inexpensive. Del Pino et alCitation19 used this method to observe the results of the treatment of cellulite with nonablative radiofrequency. In this study, panoramic images taken by diagnostic ultrasound were used to evaluate the results of the treatment of cellulite with carboxytherapy. These images allowed the registration of large anatomical areas and the access of the subdermal structures, especially fibrotic regions of septa. All images were collected and evaluated, and the comparative differences can be clearly seen in and . The analysis of the structural aspect of cellulite allowed the observation of a significant improvement in the organization of fibrous lines observable by hyperechoic area (whitish structures of fibrotic septa) compared to pictures taken before treatment, also noting hypoechoic areas of adipose tissue. These results support the findings described by LeeCitation25 in a compilation of clinical outcomes over 4 years (2004–2008) in 110 patients using carboxytherapy in the treatment of localized fat and cellulite; despite the methodological limitations of this study, the author concluded that carboxytherapy is a technique that demonstrates effectiveness for treating both localized fat and cellulite. The degrees of reduction of cellulite and possible reshaping of septa in this study likely occurred by the action of CO2 on the microcirculation and tissue perfusion, described in the subcutaneous tissue. Studies showed that local application of CO2 can promote improvement of peripheral circulation, increasing tissue perfusion and oxygen partial pressure by reflex vasodilation, and stimulate the neoangiogenesis.Citation12 In the study, after the treatment of carboxytherapy, there was a significant reduction (P=0.0025) of the cellulite from degree III to degree II, and this improvement showed correlation with the improvement in the organization of fibrous lines and the disposal of adipose tissue lines of treated regions observed through the panoramic ultrasound image diagnosis. Another factor that may contribute to the effectiveness of carboxyther-apy in the treatment of cellulite is the decrease in the density and shape of adipocytes in the treated area as demonstrated in the study by Costa et al,Citation24 since the accumulation of localized fat could contribute to increased local tissue compression, favoring the traction of fibrotic beams and herniation of adipocytes in the dermis causing the appearance of the orange peel skin depressions, a characteristic feature of cellulite disorder.
Conclusion
This pilot study showed that carboxytherapy may be used to improve the degree of severity of cellulite in the subcutaneous tissue at the buttocks and posterior thighs of healthy women. Further studies with a larger number of patients will be needed to more fully characterize the full clinical potential of carboxytherapy and its mechanism of action.
Acknowledgments
The authors thank Ms Alexandra Paioli for English language and grammatical technical support.
Disclosure
Renata Michelini Guidi and Estela Sant’Ana are researchers at IBRAMED Indústria Brasileira de Equipamentos Médicos EIRELI. The other authors report no conflicts of interest in this work.
References
- SchonvvetterBSoaresJLMBagatinELongitudinal evaluation of manual lymphatic drainage for the treatment of gynoid lipodystrophyAn Bras Dermatol201489571271825184909
- VarlaroVManzoGMugnainiFCarboxytherapy: effects on microcirculation and its use in the treatment of severe lymphedemaBlood20078113
- CorassaJMPereiraFLCPenhaMRCorassaMPUso da carboxiterapia no tratament o de distúrbios vasculares : resultados preliminares [Use of carboxitherapy in the treatment of vascular disorders: preliminary results]Revista de Angiologia e Cirurgia Vascular20068 Portuguese
- BrandiCD’AnielloCGrimaldiLCarbon dioxide therapy in the treatment of localized adiposities: clinical study and histopathological correlationsAesthetic Plast Surg200125317017411426306
- FerreiraJCTHaddadATavaresSANIncrease in collagen turnover induced by intradermal injection of carbon dioxide in ratsJ Drugs Dermatol20087320120618380201
- AbramoACOliveiraTTLedo-SilvaMCOliveiraELElevação da temperatura cutânea após a infusão controlada de dióxido de carbono [Increase of the skin temperature after infusion-controlled carbon dioxide]Rev Bras Cir Plástica2009243257261 Portuguese
- Sant’AnaEMCMarquetiRDCLeiteVLRevisão fibro edema gelóide (celulite): fisiopalogia e tratamento com endermologia [Gynoid lipodis-trophy: pathophysiology and treatment with endermologie. A review]Fisioterapia Especialidades200713035 Portuguese
- RawlingsAVCellulite and its treatmentInt J Cosmet Sci200628317519018489274
- RossiABRVergnaniniALCellulite: a reviewJ Eur Acad Dermatol Venereol200014425126211204512
- QuerleuxBCornillonCJolivetOBittounJAnatomy and physiology of subcutaneous adipose tissue by in vivo magnetic resonance imaging and spectroscopy: relationships with sex and presence of celluliteSkin Res Technol20028211812412060477
- RosenbaumMPrietoVHellmerJAn exploratory investigation of the morphology and biochemistry of cellulitePlast Reconstr Surg19981017193419399623840
- HexselDMazzucoRCelluliteTostiAHexselDUpdate in Cosmetic DermatologyMumbaiSpringer-Verlag Berlin Heidelberg20132132
- SeidellJCFlegalKMAssessing obesity: classification and epidemiologyBritish Medical Bulletin19975322382529246834
- AnuuradEShiwakuKNogiAThe new BMI criteria for Asians by the regional office for the Western Pacific Region of WHO are suitable for screening of overweight to prevent metabolic syndrome in elder Japanese workersJ Occup Health20034533534314676412
- JamesPTLeachRShayeghiMThe worldwide obesity epidemicObesity Research200194228S233S11707546
- TerranovaFBerardescaEMaibachHCellulite: nature and aetiopatho-genesisInt J Cosmet Sci200628315716718489272
- KhanMHVictorFRaoBSadickNSTreatment of cellulite. Part I. PathophysiologyJ Am Acad Dermatol201062336137020159304
- De LorenziDRSBassoEFagundesPDOSacilotoBPrevalência de sobrepeso e obesidade no climatérioRev Bras Ginecol e Obs2005278479484
- Del PinoMERosadoRHAzuelaAEffect of controlled volumetric tissue heating with radiofrequency on cellulite and the subcutaneous tissue of the buttocks and thighsJ Drugs Dermatol20065871472216989185
- PaoloFNeferFPaolaPNicolòSPeriorbital area rejuvenation using carbon dioxide therapyJ Cosmet Dermatol201211322322822938007
- Maia-FigueiróTLOdashiroANMenezesGPSemi-quantitative histological analysis of the effect of intense pulsed light (IPL) and carbon dioxide (CO2) intradermic injection on fibroblast and collagen proliferation in the skin of Wistar ratsJ Cosmet Dermatol Sci Appl20120203164173
- IrieHTatsumiTTakamiyaMCarbon dioxide-rich water bathing enhances collateral blood flow in ischemic hindlimb via mobilization of endothelial progenitor cells and activation of NO-cGMP systemCirculation2005111121523152915795362
- PiazzollaLPLouzadaLLScoralickFMMartinsMEde SousaJBPreliminary experience with carbon dioxide therapy in the treatment of pressure ulcers in a bedridden elderly patientJ Am Geriatr Soc201260237837922332686
- CostaCSOtochJPSeelaenderMCLAvaliação citométrica dos adipócitos localizados no tecido subcutâneo da parede anterior do abdome após infiltração percutânea de CO2 [Cytometric evaluation of abdominal subcutaneous adipocytes after percutaneous CO2 infiltration]Rev Col Bras Cir20113811523 Portuguese21537738
- LeeGSKCarbon dioxide therapy in the treatment of cellulite: an audit of clinical practiceAesthetic Plast Surg201034223924320111965
- BrandiCGrimaldiLNisiGThe role of carbon dioxide therapy in the treatment of chronic woundsIn Vivo201024222322620363999
- SimãoJRGuillaumonATEstudo angiográfico de fístula arteriovenosa utilizando gás carbônico como meio de contrante [Arteriovenous fistula angiography using carbon dioxide as contrast medium]Radiol Bras2004376397403 Portuguese
- MirrashedFSharpJCKrauseVMorganJTomanekBPilot study of dermal and subcutaneous fat structures by MRI in individuals who differ gender, BMI, and cellulite gradingSki Res Technol2004103161168
- MeyerPFMartinsNMMartinsFMMonteiroRAde MendonçaKMPPEffects of lymphatic drainage on cellulitis assessed by magnetic resonanceBrazilian Arch Biol Technol200851Special issue221224