
Abstract
Traction alopecia (TA) affects one-third of women of African descent who wear various forms of traumatic hairstyling for a prolonged period of time. The risk of TA is increased by the extent of pulling and duration of traction, as well as the use of chemical relaxation. The frequent use of tight buns or ponytails, the attachment of weaves or hair extensions, and tight braids (such as cornrows and dreadlocks) are believed to be the highest risk hairstyles. TA can also occur in the setting of religious and occupational traumatic hairstyling. In its later stages, the disease may progress into an irreversible scarring alopecia if traumatic hairstyling continues without appropriate intervention. The most common clinical presentation includes marginal alopecia and non-marginal patchy alopecia. A clue to the clinical diagnosis is the preservation of the fringe sign as opposed to its loss in frontal fibrosing alopecia (FFA). Dermoscopy can be helpful in the diagnosis and can detect the ongoing traction by the presence of hair casts. Histopathology can distinguish TA from alopecia areata, FFA, and patchy central centrifugal cicatricial alopecia. Currently, there is no cure. Therefore, it is imperative that clinicians educate high-risk populations about TA and those practices that may convey the risk of hair loss.
Introduction
The prevalence of traction alopecia (TA) remains high in communities that practice tight braiding of the hair and, especially, when “relaxer” chemical treatments are used to straighten hair of the African type.Citation1 In fact, one-third of women of African descent are affected.Citation2 It is now generally agreed upon that the extent of pulling and the duration of traction increase the risk of TA and that treated hair may be less resistant to traction.Citation3
In the early stage, patients typically present with patches of non-scarring hair loss along the area of the scalp that is undergoing tension. The hair loss can occur at any area of the scalp depending on the configuration of the hairstyle. Broken hairs and pustules within the follicles are often appreciated.Citation4
In its later stages, the disease may progress into an irreversible scarring alopecia if traumatic hairstyling continues without appropriate intervention. Patients may also report tenderness, itching, paresthesias, and headache.Citation5
In this review, we summarize the current literature about TA and discuss how to improve upon patient education, prevention, and care.
History
The entity today known as TA has been independently identified and described many times. In 1907, Trebitsch,Citation6 an Austrian dermatologist, reported a characteristic marginal temporoparietal alopecia among Greenlandic women who wore their hair in a traditional tight coiffure arranged on the crown of the head () but absent among Greenlandic women whose hair was arranged in looser, European styles. He attributed this alopecia to native hairstyling practices and termed this entity “alopecia Groenlandica.”Citation6 Hjorth,Citation7 studying this same population in 1957, noted a symmetrical baldness or thinning beginning at the hairline and accompanied by follicular atrophy with patchy areas of perifolliculitis. Interestingly, he noted the retention of “a thin straggling strip of hair” at the distal margin of the zone of alopecia as a characteristic of this disorder.Citation7 This is reminiscent of the “fringe sign” reported by Samrao et al in 2011.Citation8 In the years following Trebitsch’s initial description, many other investigators reported syndromes of hair loss attributable to excessive chronic traction.
Figure 1 Painting “Greenland Mother” by W Langdon Kihn (1898–1957), showing a Greenlandic Inuit woman holding her baby. Note that her hair is worn in a tight coiffure arranged at the top of her head. Traumatic marginal alopecia can be appreciated, as was described by Trebitsch in 1907 as “alopecia Groenlandica.” From: National Geographic, October 1949, page 486. Public access.
In 1931, Aramaki reported a similar syndrome of marginal alopecia in Japan, which he attributed to traditional hairstyles of that country and which he termed alopecia atrophica symmetrica temporalis.Citation9 Other investigators in that country described syndromes of marginal TA that were primarily frontal or parietal in origin, with the distribution of alopecia differing with traditional hair styles in the different regions of Japan.Citation9 Saboraud described frontal alopecia among French peasant women who wore their hair in tight chignons on the top of the head, which he termed alopecia liminaire frontale, though he did not attribute the hair loss to traction per se.Citation7 Balina, an Argentine, was the first to propose a link between the initial stages of the disease with inflammation, pustules, and crusting and the later atrophic sequelae reported by Saboraud. He was also among the first to discern that mechanical traction was the cause of hair loss in these patients.Citation10,Citation11
For most of the 20th century and into the present, research into TA has focused on its predominance amongst women of African descent due to very tight braiding and aggressive chemical and thermal treatment of hair. In 1941, Spencer published a series of four African-American women presenting with bilateral temporal alopecia, all of which endorsed a history of having worn their hair in very tight braids.Citation11 In 1958, Savill described an interaction between new brush technology and permanent hairstyling techniques that resulted in traction alopecia in a series of English patients.Citation12
Epidemiology
Prevalence
There is a paucity of data concerning the prevalence of traction alopecia among the general population. The data may be underreported based on cultural acceptance of the normality of hair loss associated with certain hairstyles. For that reason, investigation of the effects of cultural practices on TA risk is of essential importance.
One study of black adults presenting to a general dermatology clinic in London found traction alopecia to have a prevalence of 1.0%.Citation13 Another investigator reported TA to have a prevalence of 37% among women presenting to a primary care center in Cape Town, South Africa.Citation14 An industry study of African women volunteers found a prevalence of 33%.Citation2 It is likely that the prevalence of TA ranges widely between populations with similar levels of genetic risk due to differences in hairstyling practices.
In conclusion, it is clear that the prevalence of TA is highest among women, including children, of African descent, due to both mechanical characteristics of the curved African hair follicle and cultural hairdressing practices. TA is much more common among women than men.Citation15
Association with specific hair morphology
The hair of persons of African descent is uniquely distinct from the hair of persons originating in European and Asian populations.Citation16 There are several factors that make African hair more susceptible to chronic mechanical trauma.
On transverse sections, the African hair shaft has an elliptical or “kidney-like” shape, whereas the hair of Caucasians and Asians has a uniformly circular shape on transverse sections.Citation17
The African hair shaft has an asymmetrical position.Citation17 The African hair follicle is curved at its insertion into the dermis and exhibits retro-curvature at the level of the follicular bulb. This is thought to be responsible for the helical morphology of the African hair follicle.Citation18,Citation19
The follicular bulb is asymmetrically curved resembling a golf club.
The hair follicle is helically shaped with each concave and convex turn contributing to geometric points of weakness.Citation18,Citation19
The axial asymmetry and helical shape lead to the presence of geometric points of weakness, which make African hair more susceptible to breakage during combing and to the development of TA secondary to tight hairstyles that subject the hair shaft to prolonged mechanical trauma.Citation17
Association with chemical relaxation
Certain hairstyles convey a particularly high risk of TA. The frequent use of tight buns or ponytails, the attachment of weaves or hair extensions, and tight braids (such as cornrows and dreadlocks) are believed to be the highest risk hairstyles. The risk of these hairstyles contributing to TA is increased when the patient has undergone chemical relaxation of their hair.Citation1 Chemical relaxation of the hair through interruption of disulfide bonds weakens the hair shaft, and the experience of a “stinging” association during the relaxing process has been identified as predicting a higher risk of future TA. Only 18.9% of patients suffering TA denied ever experiencing painful symptoms during or following hairdressingCitation3,Citation20 Among patients who continue to wear high-risk hairstyles and repeatedly use chemical relaxers, the prevalence of TA increases over time. In a study at a South African school, the prevalence of TA in schoolgirls was found to be 8.6% among first-year students and 21.7% among those girls in the last year of school.Citation21
Geographic variations
Risk factors for TA appear to be similar between African and African-American populations.Citation22 The association between TA and practices that weaken the hair shaft or subject it to high levels of traction supports the hypothesis that TA is primarily caused by mechanical force.Citation21
Traumatic hair styles
TA has been associated with numerous types of hairstyling related to cultural, religious, and occupational practices. summarizes the different traumatic hairstyles and their associated patient population(s).
Table 1 Summary of traumatic hairstyles and their associated patient populations
Cultural practice
People of African descent wear many types of hairstyles that put them at increased risk for developing TA. The hairstyles most commonly associated with TA in this patient population include braids, including cornrows, weaves, and dreadlocks.Citation23 Khumalo et al reported an increase risk of developing TA in Africans who combine these traumatic hairstyles in the setting of chemically relaxed hair.Citation3,Citation21 Chemically relaxed hair is a commonly practiced styling technique producing a more straight and soft appearance and can be achieved through different processes. Lye relaxers contain sodium hydroxide and non-lye relaxers contain guanidine hydroxide, both of which use the hydroxide molecule to cleave the disulfide bond in the hair fiber.Citation1 These chemical straighteners reduce the tensile strength of the hair follicleCitation24 and increase hair brittleness,Citation25 which contribute to hair loss when compounded by mechanical stress of traumatic styling. However, the traction exerted on the hair root by these traumatic hairstyles is enough to cause alopecia in a background absent of chemical relaxers.Citation26 These hairstyles are utilized in this patient population because they contribute to hair manageability, flexibility, and appearance while also providing a means for celebration of cultural heritage.Citation23
Similarly, Samrao et alCitation8 reported on the increased risk of developing traction alopecia in Hispanic women who wore their hair in a tight ponytail for many years. The association was seen in Hispanic women with long, thick hair and presented with areas of hair loss primarily on the frontal and temporal scalp but also, less frequently, on the vertex and occipital scalp.
Religious practice
The literature has noted TA in association with religious practices. Sikhism is a religion originating in the Punjab region of India, which prohibits its men and women followers from cutting their hair to convey respect for God’s creation of man as he was intended. As a child, ranging from 11 to 16 years of age, the Sikh men participates in a ceremony called “dastaar bandi” in which he tries on his first turban. From this time onward, the Sikh men will tightly twist all of his hair into a knot that sits on the frontal scalp.Citation27 Then he will wrap a turban tightly around the hair to cover the top of the head which will be worn for 24 hours before being removed so the hair can be combed.Citation28 Karimian-Teherani et al reported on two formerly Sikh brothers who wore turbans since childhood who moved to Austria aged 12 and 19 years and removed their headgear after rescinding the religion. They presented with sharply demarcated band-like scarring alopecia localized to the frontal hairline.Citation29 Submandibular alopecia can also occur as the Sikh men tie their beards into tight knots that sit on the chin.Citation28 Moreover, turban-wearing is commonplace in Islamic countries and has become increasingly popular in Turkey over the last three decades.Citation30 In a passage from the Qur’an (7: 31), Muhammad exhorts, “O Children of Adam! Wear your beautiful apparel at every time and place of prayer” and therefore, the bare head is considered among the “acts which betray self-respect,” or khawarim al-muru’ah. The turban that Turkish women wear is different from that of the Sikh men, consisting of two layers, the first of which is securely wrapped around the hair and head with the second layer wrapped on top of the first. In the study conducted by Polat, Turkish women who wore their turban for less than 10 years were noted to have frontal alopecia, whereas Turkish women who wore their turban for more than 10 years were noted to have extension of hair loss into the fronto-parietal and fronto-temporal regions.Citation30
Occupational practice
Trüeb reported on three women who presented with localized occipital alopecia in the context of twisting the hair into tight bun, proposing “chignon alopecia” as a new entity.Citation31 Similarly, TA in a ballerina who wore her hair in an uncomfortably tight bun to dance class 4 days a week for 13 years presented with symmetrical temporal patches of hair loss.Citation32 To cover up the patches of hair loss, the ballerina began wearing a 1.5-pound hairpiece every day for 2 years, subjecting her to greater traction and resulting in aggravation of hair loss. Additionally, in a report studying 143 South Korean nurses, seven developed localized parieto-occipital alopecia at the site where the cap was attached to the scalp by two bobby pins for 8 hours a day with a 9.8 years average duration of cap wearing.Citation5
Children and adolescents
In the study by Wright et al, 201 caregivers of African girls aged 1–15 years reported that within the past 12 months, 81% wore ponytails, 67% wore braids, and 49% wore cornrows.Citation22 There was a significant risk of developing hair thinning along the hairline in the girls who wore cornrows within the last 12 months, which had a stronger association after controlling for use of chemical relaxers.Citation22 Oftentimes, children of African descent will attach plastic beads and barrettes to their braids, which add additional traction. Samrao et al reported that Hispanic women who presented with TA began wearing tight ponytails in childhood or their teenage years.Citation8
Sikh boys wear their hair and turbans very tightly to avoid loosening while playing, increasing the degree of traction on the hair shaft beginning in adolescence.Citation33 As previously mentioned, the two formerly Sikh men presenting in Austria had sharply demarcated scarring alopecia of the frontal hairline at the age of 12 and 19 years.Citation29
Pathogenesis
The hair loss seen in TA is thought to be caused by the exertion of excessive pulling forces, leading to mechanical damage of the hair follicles.Citation3 The damage induces an inflammatory response, which presents as perifollicular erythema with pustules and/or papules in areas of traction.Citation34 Chronic and repeated traction causes repeated follicular damage and eventually hair loss.Citation3
Clinical features and diagnosis
The earliest clinical sign of TA is perifollicular erythema that develops into a folliculitis characterized by perifollicular pustules and papules.Citation8,Citation35 In its later stages, the disease evolves into a scarring alopecia with decreased follicular markings.Citation8 The most common sites of hair loss are the frontal and temporoparietal areas, although any area of the scalp can be affected depending on the hairstyle worn ().Citation35 Marginal traction alopecia refers to hair loss and thinning that is seen along the frontal and temporoparietal margin of the hairline.Citation36 Marginal TA is often accompanied by a strip of thin hair at the distal end of the patch of alopecia that is referred to as “the fringe sign” ().Citation8 Non-marginal, or patchy, alopecia is another variant of TA that refers to patches of hair loss and thinning that occur on less commonly affected areas of the scalp that can occur secondary to hair wefts, hair pins, or clips. For example, chronic use of hair wefts, which are a component of weaves, have been described to cause a “horseshoe” pattern of hair loss.Citation36 Additionally, submandibular alopecia has been reported in Sikh men who tie their beard hair in a tight knot on their chin.Citation28
Figure 2 Biopsy-proven traction alopecia involving the frontal and parietal scalp.

Figure 3 Marginal traction alopecia in patient with braids.

Trichoscopy of patients with both marginal and non-marginal distributions of TA will demonstrate 1) reduced hair density with absence of follicular openingsCitation37 or 2) absence of hairs with preserved in-brown-outlined follicular openings that correspond on pathology to the pigmented basal cell layer of follicular infundibulum (). If there are any hairs remaining in the patches, they are exclusively of vellus origin. Patches of acute TA can present with broken hairs at different length in similarity to trichotillomania (). Numerous hair casts, yellowish-white cylinders that accumulate around traumatized hair shafts, may be appreciated on dermatoscopy at the border of the area of hair loss (). They slide easily along the hair shaft and correspond on pathology to the desquamated root sheaths. Their presence indicates the persistence of mechanical traction on the affected hair shafts.Citation37,Citation38
Figure 4 Trichoscopy of alopecic patch in traction alopecia shows only individual hairs with preserved marking of follicular openings outlined in brown that correspond to the pigmented basal cell layer of the infundibula.
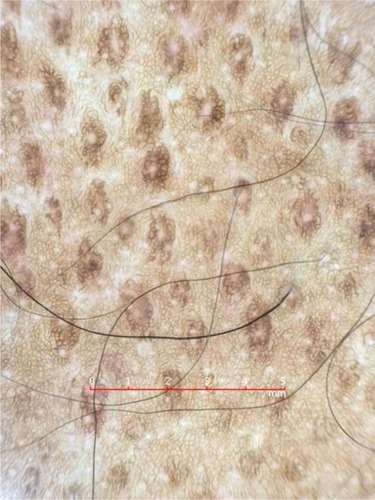
Figure 5 Trichoscopy of acute traction alopecia demonstrates black dots and broken hairs at different length. In this example, the patient is presented with marginal hair loss after removal of a glued wig.

Figure 6 Trichoscopy of traction alopecia demonstrates cylindrical hair casts along several hair shafts.

Histopathology
Early TA is rarely biopsied because patients usually seek help late when the patches are devoid of hairs and they see no regrowth. The features are similar to those in trichotillomania and consist of increased catagen/telogen count (telogen escape of traumatized follicles), pigment casts, and trichomalacia.
Late TA
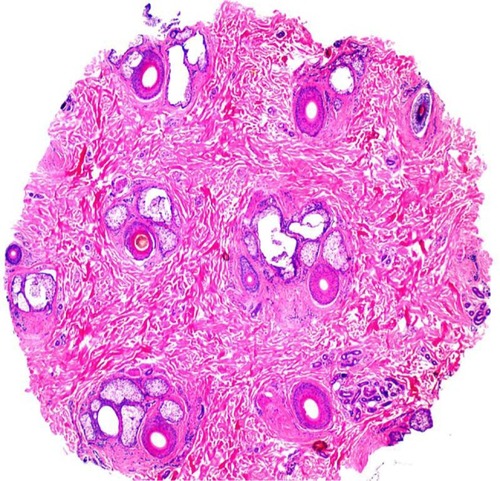
As the disease progresses into a scarring alopecia, there is an appreciated loss of terminal hair follicles or “follicular drop out”Citation8,Citation39 (). The terminal hair follicles appear to be replaced by fibrotic fibrous tracts. The vellus hairs are intact, resulting in a decreased ratio of terminal to vellus-sized hair.Citation8 There is preservation of the sebaceous glands and no perifollicular inflammatory infiltrateCitation29 ().
Figure 7 Histology of traction alopecia. On horizontal sections at the level of the low follicular level, there is altered follicular architecture due to areas of follicular drop out. There are only four follicles (hematoxylin and eosin, ×2).
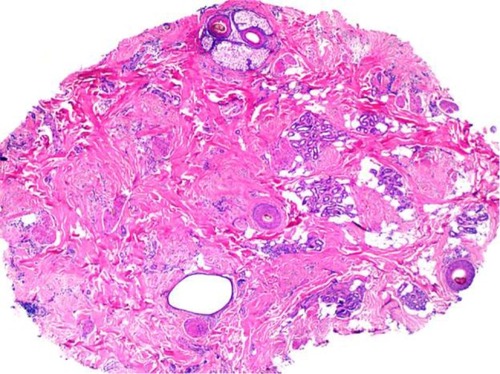
Figure 8 Histology of traction alopecia. On horizontal sections at the level of the isthmus, there is an overall preserved follicular architecture but significantly reduced follicular density (total of nine follicles). The terminal: vellus ratio is 2:1. The sebaceous glands are mostly preserved (hematoxylin and eosin, ×2).
Differential diagnosis
In its early stage, patients with TA typically present with patches of non-scarring hair loss along the area of the scalp that is undergoing tension, which can mimic trichotillomania and alopecia areata by the presence of non-scarring alopecia and broken hairs. In the late stage, there are smooth hairless patches with follicular drop out, which need to be distinguished from scarring alopecias such as frontal fibrosing alopecia (FFA) and patchy central centrifugal cicatricial alopecia (CCCA). Distinctive features on clinical examination, trichoscopy, and pathology allow for the correct diagnosis ().
Table 2 Summary of the distinguishing clinical, trichosopic, and pathologic findings in patients with patchy alopecias
Management
Chronic TA may, in its later stages, develop into an irreversible scarring alopecia not remediable to therapy. Therefore, it is imperative that clinicians educate high-risk populations about TA and those practices that may convey the risk of hair loss. Mirmirani and Khumalo proposed two slogans, “Tolerate pain from a hairstyle and risk hair loss” and “No braids or weaves on relaxed hair,” in order to bridge patient–provider knowledge gaps in the avoidance of traction alopecia.Citation40 Because most cases of traction alopecia can be reversed,Citation23 if the appropriate interventions are taken at an early stage of the disease; clinicians must be vigilant and proactive in their care of patients who may be at risk. The key to management at any stage in the disease course is the relief of traction exerted upon the hair shaft by the loosening of traumatic hairstyles. Avoidance of chemical and thermal treatment of hair is also recommended, as well as the avoidance of combining traumatic hairstyling with chemically and thermally treated hair.Citation35 The earliest clinical sign of TA is perifollicular erythema, which may be followed by the development of folliculitis characterized by pustules and papules.Citation8,Citation41 Initial medical management is directed at combating these inflammatory effects through the use of topical and intralesional corticosteroids applied to the margin of hair loss, as well as oral and topical antibiotics for their anti-inflammatory properties.Citation21,Citation25,Citation35 There are several reports in the literature showing promising results for topical minoxidil in the treatment of advanced TA. Khumaloand Ngwanya reported two cases of women suffering late stage TA who experienced hair regrowth at 3 months and significant hair regrowth after 6 and 9 months, respectively, with the topical application of 2% minoxidil.Citation42 Same patients had previously experienced no response with 1–2 years of abstention from traumatic hairstyling practices. Additionally, Callender et al reported anecdotal success with topical minoxidil in a subset of TA patients.Citation23 Further study is required in order to determine the optimal duration and concentration of minoxidil therapy in the treatment of TA. Although there are no reports on the use of 5% minoxidil in traction alopecia, it may be considered as an alternative therapeutic option. Latanoprost has not been studied in TA.
The advanced stages of TA, characterized by scarring and follicular atrophy, are less amenable to medical therapy, but surgical treatment through hair transplantation may be an option for some patients. Successful hair transplantation for patients with advanced TA has been documented with multiple techniques, including punch grafting with rotation flaps,Citation43 micro (1–2 follicular unit grafts), and mini (3–4 follicular unit grafts) grafting.Citation44 Ozcelik reported a case of a 23-year-old woman with a 5-year history of wearing an extremely tight ponytail every day in order to elevate her eyebrows who presented with bilateral temporal scarring alopecia and underwent one session of micro- and mini-graft transplantation. At 1-year follow-up, the patient had 90%–95% survival of hair at the recipient site with a natural direction of hair growth and reported satisfaction with cosmesis.Citation44 With hair transplantation, it is important to counsel the patient on realistic outcomes and likelihood of multiple sessions in order to achieve cosmetically favorable outcomes.
It is of paramount importance that clinicians educating and treating patients with TA remain sensitive and aware of the cultural importance of potentially harmful hairstyling practices.
Future goals
Further research is required to identify the exact pathogenic mechanism of TA including the role of stem cells and genetic factors in the development of the disease.
Effective education on prevention, creating community support, and disseminating awareness about TA and risky hairstyling practices among those populations at risk. This is particularly true for the parents of young children who wear traumatic braids and cornrows with/without attached plastic accessories from a very young age.
Improved means of detecting those individuals who may be developing TA will allow earliest effective dermatological intervention.
Randomized clinical trials will help to develop an evidence base for effective treatment algorithms.
While behavioral therapy has shown favorable results in trichotillomania, its value in the management of TA has not studied. Because certain hairstyles are important for cultural identity, public education initiatives targeting the populations with high risk would be the optimal intervention.
Disclosure
The authors report no conflicts of interest in this work.
References
- KhumaloNJessopSGumedzeFEhrlichRHairdressing and the prevalence of scalp disease in African adultsBr J Dermatol2007157598198817725667
- LoussouarnGEl RawadiCGenainGDiversity of hair growth profilesInt J Dermatol200544s16916187948
- KhumaloNPJessopSGumedzeFEhrlichRDeterminants of marginal traction alopecia in African girls and womenJ Am Acad Dermatol200859343243818694677
- HeathCRTaylorSCAlopecia in an ophiasis pattern: traction alopecia versus alopecia areataCutis201289521321622768432
- HwangSMLeeWSChoiEHLeeSHAhnSKNurse’s cap alopeciaInt J Dermatol199938318719110208613
- TrebitschRDie Krankheiten der Eskimos in West-GrönlandWiener Klin Wochenschr19072014041408
- HjorthNTraumatic marginal alopecia; a special type: alopecia groenlandicaBr J Dermatol195769931932213460178
- SamraoAPriceVHZedekDMirmiraniPThe “Fringe Sign” – a useful clinical finding in traction alopecia of the marginal hair lineDermatol Online J201117111
- KrstićAKonstantinovićSŽunićMIlić-KrstićBTraction alopecia due to traditional hair stylesOrfanosCEMontagnaWHair ResearchBerlinSpringer1981390391
- CostaOGTraumatic marginal alopecia due to traction on the hairBr J Dermatol19465811–12280286
- SpencerGAAlopecia liminaris frontalis: comment on causation and report of four casesArch Dermatol Syphilol194144610821085
- SavillAThe nylon brushBr J Dermatol1958708–929629913572718
- ChildFFullerLHigginsEDu VivierAA study of the spectrum of skin disease occurring in a black population in south-east LondonBr J Dermatol1999141351251710583057
- KhumaloNPJessopSEhrlichRPrevalence of cutaneous adverse effects of hairdressing: a systematic reviewArch Dermatol2006142337738316549718
- KhumaloNPThe “fringe sign” for public education on traction alopeciaDermatol Online J201218916
- LindelofBForslindBHedbladMAKaveusUHuman hair form. Morphology revealed by light and scanning electron microscopy and computer aided three-dimensional reconstructionArch Dermatol19881249135913633415278
- HerskovitzIMitevaMCentral centrifugal cicatricial alopecia: challenges and solutionsClin Cosmet Investig Dermatol20169175181
- BernardBAHair shape of curly hairJ Am Acad Dermatol2003486 SupplS120S12612789164
- ThibautSBernardBAThe biology of hair shapeInt J Dermatol200544Suppl 12316187946
- HaskinAAguhCAll hairstyles are not created equal: what the dermatologist needs to know about black hairstyling practices and the risk of traction alopecia (TA)J Am Acad Dermatol201675360661127114262
- KhumaloNJessopSGumedzeFEhrlichRHairdressing is associated with scalp disease in African schoolchildrenBr J Dermatol2007157110611017553035
- WrightDRGathersRKapkeAJohnsonDJosephCLHair care practices and their association with scalp and hair disorders in African American girlsJ Am Acad Dermatol201164225326220728245
- CallenderVDMcMichaelAJCohenGFMedical and surgical therapies for alopecias in black womenDermatol Ther200417216417615113284
- BolducCShapiroJHair care products: waving, straightening, conditioning, and coloringClin Dermatol200119443143611535384
- McMichaelAJHair and scalp disorders in ethnic populationsDermatol Clin200321462964414717404
- GrimesPESkin and hair cosmetic issues in women of colorDermatol Clin200018465966511059374
- JamesJSaladiRNFoxJLTraction alopecia in Sikh male patientsJ Am Board Fam Med200720549749817823469
- KanwarAJKaurSBasakPSharmaRTraction alopecia in Sikh malesArch Dermatol19891251115871587
- Karimian-TeheraniDEl shabrawi-CaelenLTanewATraction alopecia in two adolescent Sikh brothers – an underrecognized problem unmasked by migrationPediatr Dermatol201128333633821371118
- PolatMEvaluation of clinical signs and early and late trichoscopy findings in traction alopecia patients with Fitzpatrick skin type II and III: a single-center, clinical studyInt J Dermatol201756885085528369851
- TrüebR“Chignon alopecia”: a distinctive type of nonmarginal traction alopecia”Cutis19955531781797634850
- SamraoAChenCZedekDPriceVHTraction alopecia in a ballerina: clinicopathologic featuresArch Dermatol2010146891893520713832
- SinghGTraction alopecia in Sikh boysBr J Dermatol19759222322331148120
- FoxGNStausmireJMMehreganDRTraction folliculitis: an under-reported entityCutis20077912630
- LawsonCNHollingerJSethiSUpdates in the understanding and treatments of skin & hair disorders in women of colorInt J Womens Dermatol201731S21S3728492036
- AhdoutJMirmiraniPWeft hair extensions causing a distinctive horseshoe pattern of traction alopeciaJ Am Acad Dermatol2012676e294e29523158648
- TostiAMitevaMTorresFVincenziCRomanelliPHair casts are a dermoscopic clue for the diagnosis of traction alopeciaBr J Dermatol201016361353135520716211
- ScottMJJrRoenigkHHJrHair casts: classification, staining characteristics, and differential diagnosisJ Am Acad Dermatol19838127326186702
- SperlingLCScarring alopecia and the dermatopathologistJ Cutan Pathol200128733334211437938
- MirmiraniPKhumaloNPTraction alopeciaDermatol Clinics2014322153161
- ScottDADisorders of the hair and scalp in blacksDermatol Clin1988633873953048821
- KhumaloNNgwanyaRTraction alopecia: 2% topical minoxidil shows promise. Report of two casesJ Eur Acad Dermatol Venereol200721343343417309495
- EarlesRMSurgical correction of traumatic alopecia marginalis or traction alopecia in black womenJ Dermatol Surg Oncol198612178823941194
- ÖzçelikDExtensive traction alopecia attributable to ponytail hairstyle and its treatment with hair transplantationAesthetic Plast Surg200529432532716044234