
Abstract
Background
Hand dermatitis or hand eczema (HD) is one of the most common dermatologic conditions. Lesions, scaling, pruritus and pain are chronic and relapsing. Improved HD has been reported with the probiotic composed of Lactobacillus acidophilus CL1285, Lactobacillus casei LBC80R and Lactobacillus rhamnosus CLR2 (Bio-K+).
Purpose
Investigation of the therapeutic potential of this probiotic as the sole systemic treatment for adults with nonacute HD.
Subjects and methods
A single-center study documented clinical ratings and patient-reported outcomes in adults with chronic HD. The probiotic was taken orally for 12 weeks, adjunctive to standard topical treatments and preventative measures.
Results
Most of the 30 subjects with mild to severe HD were compliant with the probiotic. Around 22 of the 30 subjects were able to complete the study, and of these subjects, an improvement was noted in 19. One required systemic therapy, and one subject was not able to tolerate the probiotic and therefore discontinued the study. 23% of the subjects achieved clear or almost clear hands by the end of 12 weeks. Pruritus, which was a common complaint at baseline, was improved with 59% of symptomatic patients within 2 weeks.
Conclusion
It is feasible and safe to administer Bio-K+ for HD. Clinicians saw an improvement in most subjects’ hands, and cases of significant improvement in dermatitis were documented. Pruritus was the most rapidly relieved symptom, as reported by patients.
Introduction
Advances in molecular methods over the past decade have revealed that the human microbiomes of the gastrointestinal tract and the skin are determinants of allergic diseaseCitation1 and skin homeostasis.Citation2 Manipulation of these microbial communities is now an emerging treatment axis in dermatology.Citation3–Citation5 Compared to other systemic treatments, the relative safety and tolerability of orally ingested probiotic microorganisms makes them attractive for long-term prevention of acute cutaneous statesCitation3 although their use has outpaced the collection of clinical data.Citation6 The expected therapeutic effects for mature illness, even in common conditions, are largely unknown and scarcely documented in a research setting.
Hand dermatitis or hand eczema (HD) is one of the most common dermatological conditions affecting 10% of the population with dryness, erythema and scaling on the hands coupled with pruritus and pain.Citation7–Citation9 Although HD is often the result of multiple exogenous and endogenous causes, a higher incidence of HD is associated with certain occupations (occupational dermatitis), such as those involving frequent “wet work” or contact with irritants and allergens (ie, hairdressers, nurses, etc)Citation10–Citation12 HD is a fluctuating condition where hands are transiently or chronically (CHD) affected by lesions. The clinical goals are to prevent progression to an acute clinical state and to manage symptoms, rather than cure the condition.Citation12–Citation14 Lesions on the hand are of concern to patients, but intense and constant symptoms of pain and pruritus are a major driver for patients to seek medical help.Citation15 Even with proper skin hygiene, acute states of HD can occur and will necessitate potent topical treatments, phototherapy or systemic corticosteroids.Citation11,Citation14 These carry an important burden of adverse effects and cannot be used for long term. There is a continued need for tolerable preventative treatments.
Consumers of a probiotic available over the counter in Canada and the United States composed of Lactobacillus acidophilus CL1285, Lactobacillus casei LBC80R and Lactobacillus rhamnosus CLR2, known as Bio-K+® (Bio-K Plus International Inc, Laval, QC, Canada)Citation16 have reported improved HD.Citation17 The efficacy and safety of this probiotic formulation have been studied quite extensively in diarrhea prevention.Citation18,Citation19 To document better and to understand the nature of these improvements, an exploratory, single-center, open-label trial was designed to describe the clinical effects with this probiotic and evaluate its feasibility as the sole systemic treatment for adults with chronic HD, adjunctive to standard topical treatments and preventative measures.
Subjects and methods
Study participants
Thirty subjects were enrolled at one study center in St. John’s, Newfoundland and Labrador (NL), Canada, from September 2009 to November 2010. All research procedures performed in the study were in strict accordance with the study protocol, which had full ethics approval from the central ethic committee of the Research Review Board (Waterloo, ON, Canada).
Male and female subjects over 18 years of age with mild to severe HD for ≥6 months and willing to comply with treatment and prevention guidelinesCitation12 were included in this study. Female patients of childbearing potential were required to have a negative pregnancy test at baseline and used a reliable contraceptive method throughout the study duration.
A dermatologist excluded those affected by skin conditions other than eczema on their hands; had infected lesions on the hands requiring medical treatment, or had known exogenous causes of HD, dyshidrotic or hyperkeratotic eczema. Subjects were not permitted to use systemic treatments for their dermatitis such as a corticosteroid, nonsteroidal anti-inflammatory drug, immunomodulator, biologic (antibodies, fusion proteins, etc), oral primrose oil or traditional Chinese herbal therapies. Subjects were excluded from the study if they had previously received a heart valve replacement, had a serious illness within the 4 weeks preceding the study or presented with a medical condition that in the opinion of the investigator would adversely affect their safe participation in the study or affect the conduct of the study. Also, subjects with a history of substance abuse or a history of poor compliance with medical treatment were excluded.
At screening, a dermatologist performed a thorough examination and completed a checklist of inclusion and exclusion criteria confirming the eligibility of each subject. All eligible subjects received consent forms at least 24 hours prior to their first visit. During their baseline visit, subjects were provided with a full study explanation and answers to any questions before providing their written informed consent to study participation.
Interventions
Subjects took one enteric-coated capsule daily of a commercially available probiotic containing 30 billion colony-forming units (CFUs) of L. acidophilus CL1285, L. casei LBC80R and L. rhamnosus CLR2 (Bio-K+® 30 Billion; Bio-K Plus International Inc,). Patients were instructed to refrigerate the product and take 1 capsule after breakfast each day for 12 weeks.
At each study visit, the subjects were reminded to follow standard preventative measures to avoid worsening of HD, which includes using a soap-free cleanser; applying a skin moisturizer and avoiding common irritants, harsh cleansers and very hot water.Citation19,Citation20 Anti-itch products and over-the-counter hydrocortisone creams were permitted, but the use of systemic treatments for their dermatitis was not permitted.
Outcomes
The primary outcomes in this study documented the physician- and patient-reported changes in intensity, area affected by irritation and symptoms of pain and pruritus on the hands. The secondary outcomes relate to the feasibility of this treatment regimen in terms of tolerability, safety and the need for higher potency treatments.
Assessments
Demographic information (ie, age, sex, height, weight, etc) and the HD status were recorded at baseline. To aid recall at each interview, subjects kept a daily diary of their general well-being and any adverse effects. A telephone interview was performed at day 7 to ensure compliance with the study protocol and address any questions. The extent and severity of each subject’s HD was assessed at baseline and at 2, 4, 8 and 12 weeks of treatment. Subjects who withdrew early were contacted by a study team member to determine the reason for withdrawal and its relatedness to the treatment.
Clinical assessment was performed by one of the two physicians who conducted the study. The Physician’s Global Assessment (PGA) of overall HD severityCitation21 has been widely used for studies on HD and other types of dermatitis. The PGA considers five states of HD (severe, moderate, mild, almost clear and clear) based on seven observed features (erythema, scaling, hyperkeratosis/lichenification, vesiculation, edema, fissures and pruritus/pain) present on the palm or dorsum of both hands. A state of almost clear or clear at 12 weeks, as a result of a minimum two state changes, was considered a meaningful improvement of HD. The modified Total Lesion Symptom Scale (mTLSS) is a validated tool for HDCitation22 to quantify the seven features of HD (0 = none, 1 = mild, 2 = moderate and 3 = severe) for a maximum score of 21 for each hand. Symptoms of pruritus and pain were scored by a physician based on interview questions with the subject. Some subjects were diagnosed with HD only on one hand. For those subjects, ratings were not collected for the healthy hand.
When subjects reported itchy skin, they further specified the frequency with a 5-point scale (1 = >10% of the day, 2 = only after hand is wet, 3 = >30% of the day, 4 = most of the time and 5 = continuously). The presence of pain was reported by subjects using a 5-point scale (1 = strongly disagree to 5 = strongly agree).
At the end of the 12-week treatment clinicians and subjects reflected on the treatment period. Clinicians estimated the overall percentage improvement for each hand: no change (0%), slight (1–25%), minimal (26–50%), moderate (51–74%) or significant change (75–100%). Subjects completed a defined schedule of questions related to their current skin condition and its evolution during treatment.
Statistical analyses
Paired sample t-test or repeated measure ANOVA were performed using Statistical Package for the Social Sciences 18.0 at Technical University, Delft, Netherlands, and the Newfoundland and Labrador Centre for Health Information, St. John’s, NL, Canada. mTLSS scores were treated as a continuous variable. The testable hypothesis was that the skin condition and burden of symptoms would remain the same overall. The overall treatment effect for each hand was calculated with one-way repeated measures ANOVA. The first analysis tested the effect in per protocol (PP) subjects who had mTLSS data for all 5 time points and excluded individuals with early termination. The second analysis tested the effect in all intention-to-treat subjects using imputed values for early termination, carrying forward the last recorded mTLSS score throughout remainder of trial period. Paired sample t-tests tested differences in mTLSS scores between baseline and each time point for each hand.
The evolution of the skin’s condition and the presence of symptoms were treated as discrete variables. A significant change in the skin’s overall condition meant clinicians had scored a significant change (75–100%) for each affected hand. Lesions from either hand were considered in reporting the prevalence of lesions and incidence of new lesions. Pruritus was considered frequent if subjects rated itchiness >30% of the time on either hand. Pain was considered present if subjects reported pain on either hand. A McNemar’s test was performed to detect significant changes in discrete data over time using GraphPad QuickCalcs (GraphPad Software Inc).
Results
Baseline characteristics
A total of 32 patients were screened at the study center and consented to treatment. Two subjects were not included due to a screen failure. Thirty subjects received treatment, and 22 completed the study period of 12 weeks. Most subjects had HD on both hands at baseline; however, four subjects were only affected on one hand (two rights and two lefts).
The majority of the participants were female (68%), had a history of HD longer than 5 years (87%) and were experiencing frequent itchiness or painful hands (83%). All subjects were in good health with 7 participants (23%) reporting a tobacco smoking habit at baseline (mean of 5 packs/week). At the start of the study, 12 participants (40%) reported regular usage of a moisturizer for HD control ().
Table 1 Subject characteristics at baseline, N = 30
Primary outcomes
The PGA rated 12 subjects in a better state than baseline (55%) and 5 subjects (23%) in a clear or almost clear state at the end of the study, representing at least a two state improvement. For the majority of subjects, 19 of 22 (86%), clinicians estimated a slight, or better, improvement and significant improvement (75–100% change for each affected hand) in 6 subjects (27%). When asked about their hands at the end of the study, about half the subjects reported that their skin condition had improved overall, 10 (45%), or there were no new lesions on either hand, 11 (52%). Many fewer agreed that their hands were free from irritation, 6 (27%).
Although variability of mTLSS scores remained high throughout the study, there was a statistically significant treatment effect of Bio-K+ to reduce the lesion symptom score for each hand in subjects with complete data sets (right hand, F = 2.8, P = 0.027, left hand, F = 3.4, P = 0.011) and when missing data were imputed (right hand, F = 2.8, P = 0.027, left hand, F = 3.5, P = 0.010). Pairwise comparisons showed that scores were significantly lower than baseline at days 14, 28 and 56, for the right and left hands, but not at day 84 ().
Table 2 Paired t-test for differences in mTLSS scores for each hand
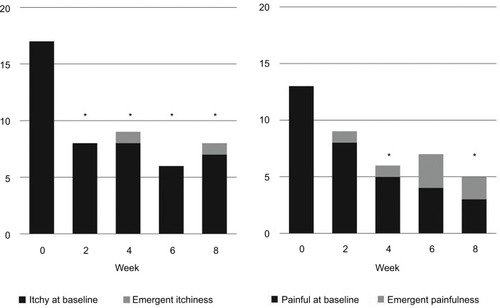
Frequent itchiness (>30% of the day) was reported by fewer subjects at every follow-up visit, dissipating for 10 of 17 and emerging for 1 in 5 by the end of the study, . Painfulness of the hands was also reported in fewer subjects at each visit, dissipating for 10 of 13 and emerging in 2 of 9 by the end of the study.
Figure 1 Number of subjects with stable or emergent itchiness (>30% of the time) and painfulness of the hand (per protocol subjects, N = 22).
Secondary outcomes
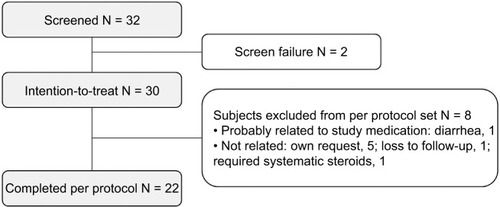
A consort flow diagram for this study is shown in . Of the 30 subjects who took the probiotic daily, all but one was able to tolerate it. One subject withdrew from the study after 4 weeks because of diarrhea that was probably related to the study medication. One subject experienced a worsening of eczema within the first 2 weeks and withdrew from the study to initiate systemic corticosteroid treatment. Five others withdrew consent before the end of the study, and one was lost to follow-up. The baseline profile of the 22 subjects (73%) who completed the study PP was not markedly different than the intention-to-treat population ().
Figure 2 Consort flow diagram.
Discussion
This is one of the first study that is documenting the effects of a probiotic for CHD, a common skin condition. There are numerous studies of probiotics in the treatment of children with atopic dermatitis, AD, and relatively fewer studies in adults.Citation6,Citation23 Atopy increases the risk for HD,Citation9,Citation24 and about one in three subjects in this study had a history of AD. But subjects with known allergic and exogenous triggers were excluded from this study, delineating a population of commonly seen patients where few treatment options remain.
With no comparator arm, it is not possible to determine if changes were specific to the probiotic treatment. Still, much was learned from this chronic population. First, we could confirm that it was feasible for most of the HD patients to take this probiotic as a capsule once daily within the recommended regimen of preventative measures. Although eight subjects withdrew from the study over the course of 12 weeks, there was no noticeable difference in terms of age, sex or history of symptom burden between those recruited into the study and those who completed PP. CHD is a condition that waxes and wanes, which can moderate a research participant’s motivation. The discontinuation rate (27%) was higher than planned but within the expected range for this type of study. A Cochrane review of emollients and moisturizers in eczema looked at a similar patient population who were seeking strategies to avoid acute dermatitis. The incidence of subjects experiencing a flare while taking a moisturizer was 13%, and the likelihood of study discontinuation ranged from 4% to 25%.Citation25 All but one participant in our study were able to manage their HD without escalating to systemic therapies and thus avoid the adverse effects that come with them. One subject was unable to tolerate the treatment due to gastrointestinal symptoms, which subsided after discontinuation.
The study was designed to explore the evolution of HD symptomatology in a cohort of typical, chronic patients using a variety of dermatology rating instruments. The state of irritation on the hands ranged from mild to severe at the start of the study and fluctuated from month to month. The testable hypothesis for these refractory subjects was that their skin condition and burden of symptoms would remain the same overall. The mTLSS is a precise and validated tool to quantify the affected area, intensity of irritation and symptom burden in HD.Citation22 Repeated measures statistical testing of this continuous variable confirmed that there was a significant, albeit small improvement overall. Missing data from subjects who discontinued early introduces a potential bias to this type of analysis if they left due to a high symptom burden. To account for this, the analyses were also performed imputing the last observation for missing data but these yielded equivalent results. From a practical point of view, the high variability between subjects and within subjects made this an impractical tool for a small observational study.
As noted in the Canadian Hand Dermatitis Management Guidelines, multiple therapies have been investigated for the treatment of hand eczema.Citation12 The efficacy of these ranges from no improvement to improvement up to 70% using topical steroids. Studies of oral alitretinoin in subjects with severe CHD observed that 48% of patients achieved a state of clear or almost clear hands at 24 weeks using the PGA, compared to 17% placebo.Citation22 In the physician’s impression, most subjects, 86%, in this study had some form of improvement with 12 weeks of treatment, and 23% attained a state of clear or almost clear rated by the PGA. There was a good agreement between the PGAand patient-reported outcomes. Still, many subjects remained symptomatic and continued to have visible dermatitis. It was not possible to determine which baseline features predicted a meaningful improvement. It could be that Bio-K+ benefited only a subgroup within this diverse population based on endogenous features or their existing intestinal microbiota.
For more than 80% of subjects with symptoms of frequent itchiness and painful hands at baseline, symptoms dissipated more than would have been predicted by chance and normal distribution. In particular, improvements in itchiness were remarkable. After only 2 weeks of treatment, more than half of the subjects had improved and there were no new emergent cases. Still, there were subjects with frequent itchiness that persisted through treatment, suggesting there could be different etiologies of pruritus or compatibility to treatment. Matsumoto et al saw significant improvements in itchiness symptoms for adult subjects with AD compared to placebo with the probiotic Bifidobacterium animalis subsp lactis LKM512.Citation26 In that study, there was a correlation between the production of a bacterial metabolite and kynurenic acid and decreased pruritus. Future studies with Bio-K+ should aim to determine if metabolites in the blood and stool predict symptomatic changes.
Scientific awareness of the role of the gut microbial community in the development and symptomatology of AD is quite advanced, while the role and function of the skin micro-biota is still being elucidated.Citation1,Citation2 In theory, the direct application of living microbes to the skin should lead to a more potent response,Citation1 yet few clinical cases or interventional studies of topical applications have been reported.Citation2 The majority of probiotic studies in dermatology have looked at the oral route of administration, targeting the intestinal tract.Citation3,Citation6,Citation23 Although the exact mechanism of probiotics at distant sites is currently unknown, it is likely that the microbes remain in the gastrointestinal tract where they positively influence local inflammation that can translate into systemic effects too.Citation1,Citation5 For example, a probiotic formulation containing Lactobacillus salivarius LS-01 improved atopic symptoms in adults and also led to reduced immune reactivity during pollen season.Citation27 But the efficacy of probiotics in treating skin conditions, and other medical applications, seems to be strain and dose specific,Citation3 and these may even act via differing mechanisms.Citation5 Preclinical studies in a murine model of AD hint that Bio-K+ exerts a different systemic effect than corticosteroids. After repeated challenges to oxazolone, topical clobetasol reduced skin inflammation and epidermal proliferation as expected, whereas the effects of orally ingested Bio-K+ were more narrow.Citation28 The probiotic resulted in an equivalent reduction in epidermal proliferation, but no other immunological or dermal effects. Although these studies demonstrated that if taken orally this probiotic led to distal changes and altered the pathology of dermatitis differently than topical corticosteroid, we are left with many unanswered questions about the mechanism of action.
Conclusion
This small study presents an encouraging account in CHD and confirms that it is safe to study Bio-K+ alongside standard preventative measures. Future clinical research should seek to demonstrate an effect of this probiotic above and beyond standard preventative measures and to determine its compatibility with other systemic treatments. The role of the microbiome in skin health is evolving quickly,Citation1,Citation4 as is our understanding of how probiotics act at distant sites.Citation1,Citation5 A better understanding of the mechanism of action on dermatitis symptoms will help identify which subjects are most likely to benefit from this particular probiotic.
Acknowledgments
Bio-K Plus International Inc. owns and manufactures the study product (Bio-K+®) and was the sponsor of the study.
Disclosure
WPG and ASH received research funding as clinical investigators for this study from Bio-K Plus International Inc. NS is an employee of Bio-K Plus International Inc. The authors report no other conflicts of interest in this work.
References
- HuangYJMarslandBJBunyavanichSO’MahonyLLeungDYMuraroAFleisherTAThe microbiome in allergic disease: current understanding and future opportunities—2017 PRACTALL document of the American Academy of Allergy, Asthma and Immunology and the European Academy of Allergy and Clinical ImmunologyJ Allergy Clin Immunol201713941099111028257972
- FriedrichADPazMLLeoniJGonzález MaglioDHMessage in a bottle: dialog between intestine and skin modulated by probioticsInt J Mol Sci2017186E106728598354
- Fuchs-TarlovskyVMarquez-BarbaMFSriramKProbiotics in dermatologic practiceNutrition201632328929526707956
- LyndeCWAndriessenABertucciVThe skin microbiome in atopic dermatitis and its relationship to emollientsJ Cutan Med Surg2016201212826492918
- ReidGAbrahamssonTBaileyMHow do probiotics and prebiotics function at distant sites?Benef Microbes20178452153328726511
- KimSOAhYMYuYMChoiKHShinWGLeeJYEffects of probiotics for the treatment of atopic dermatitis: a meta-analysis of randomized controlled trialsAnn Allergy Asthma Immunol2014113221722624954372
- MedingBJärvholmBIncidence of hand eczema—a population-based retrospective studyJ Invest Dermatol2004122487387715102075
- DiepgenTLAgnerTAbererWManagement of chronic hand eczemaContact Dermatitis200757420321017868211
- ThyssenJPJohansenJDLinnebergAMennéTThe epidemiology of hand eczema in the general population—prevalence and main findingsContact Dermatitis2010622758720136890
- SkoetRZachariaeRAgnerTContact dermatitis and quality of life: a structural review of the literatureBr J Dermatol2003149345245614510974
- AgnerTAndersenKEBrandaoFMEECDRGHand eczema severity and quality of life: a cross-sectional, multicentre study of hand eczema patientsContact Dermatitis2008591434718537992
- LyndeCGuentherLDiepgenTLCanadian hand dermatitis management guidelinesJ Cutan Med Surg201014626728421084020
- BourkeICoulsonIEnglishJBritish Association of Dermatologists Therapy Guidelines and Audit SubcommitteeGuidelines for the management of contact dermatitis: an updateBr J Dermatol2009160594695419302065
- CoenraadsPJHand eczemaN Engl J Med2012367191829183723134383
- Van CoevordenAMWilliamsHCSvenssonÅDiepgenTLElsnerPCoenraadsPJInterventions for hand eczema. (Protocol)Cochrane Database Syst Rev20023CD004055
- AuclairJFrappierMMilletteMLactobacillus acidophilus CL1285, Lactobacillus casei LBC80R, and Lactobacillus rhamnosus CLR2 (Bio-K+): characterization, manufacture, mechanisms of action, and quality control of a specific probiotic combination for primary prevention of Clostridium difficile infectionClin Infect Dis201560Suppl 2S135S14325922399
- GaoXWMubasherMFangCYReiferCMillerLEDose response efficacy of a proprietary probiotic formula of Lactobacillus acidophilus CL1285 and Lactobacillus casei LBC80R for antibiotic-associated diarrhea and Clostridium difficile-associated diarrhea prophylaxis in adult patientsAm J Gastroenterol201010571636164120145608
- GoldsteinEJCJohnsonSJMaziadePJEvansCTSniffenJCMilletteMMcFarlandLVProbiotics and prevention of Clostridium difficile infectionAnaerobe20174511411927988389
- BerndtUWigger-AlbertiWGabardBElsnerPEfficacy of a barrier cream and its vehicle as protective measures against occupational irritant contact dermatitisContact Dermatitis2000422778010703628
- EnglishJSCOccupational dermatosesBurnsDABreathnachSMCoxNHGriffithsCEMTextbook of Dermatology7th edOxfordBlackwell Publishing200421.821.9
- CoenraadsPJvan Der WalleHThestrup-PedersenKConstruction and validation of a photographic guide for assessing severity of chronic hand dermatitisBr J Dermatol2005152229630115727642
- RuzickaTLyndeCWJemecGBEfficacy and safety of oral alitretinoin (9-cis retinoic acid) in patients with severe chronic hand eczema refractory to topical corticosteroids: results of a randomized, double-blind, placebo-controlled, multicentre trialBr J Dermatol2008158480881718294310
- RatherIABajpaiVKKumarSLimJPaekWKParkYHProbiotics and atopic dermatitis: an overviewFront Microbiol2016750727148196
- AgnerTAalto-KorteKAndersenKEEuropean Environmental and Contact Dermatitis Research Group. Classification of hand eczemaJ Eur Acad Dermatol Venereol201529122417242226371368
- van ZuurenEJFedorowiczZChristensenRLavrijsenAArentsBWMEmollients and moisturisers for eczemaCochrane Database Syst Rev20172CD01211928166390
- MatsumotoMEbataTHirookaJAntipruritic effects of the probiotic strain LKM512 in adults with atopic dermatitisAnn Allergy Asthma Immunol2014113220921624893766
- DragoLToscanoMDe VecchiEPiconiSIemoliEChanging of fecal flora and clinical effect of L. salivarius LS01 in adults with atopic dermatitisJ Clin Gastroenterol201246SupplS56S6322955359
- ShipNMilletteMMilletteEBoutinYGulliverWInvestigating the therapeutic potential of the probiotic Bio-K+ for hand dermatitis in a clinical population and a mouse model [abstract]J Int Soc Microbiota20174117 Available from: https://doi.org/10.18143/jism_v4i1Accessed April 16, 2018