
Abstract
Atopic dermatitis (AD) is a chronic inflammatory skin disease that greatly impacts patient quality of life. Type 2 cytokine interleukin (IL)-13 is integral to the pathogenesis of AD. Tralokinumab is a fully human IgG4 monoclonal antibody that specifically targets IL-13, preventing downstream signaling of inflammatory pathways that may contribute to AD. Tralokinumab was US Food and Drug administration (FDA) recently approved for the treatment of moderate to severe AD on December 28, 2021. In our review, we will explore the efficacy and adverse effects (AEs) of tralokinumab for the treatment of patients with moderate to severe AD. A PubMed search for key articles on the emerging clinical data of tralokinumab was performed. Six randomized controlled trials of tralokinumab identified improvements in disease severity measures, including Investigator’s Global Assessment (IGA) scores and Eczema Area Severity Index 75 (EASI75) scores. Four of these studies demonstrated improvements in quality of life measures with tralokinumab, including pruritus scores, sleep interference scores, Dermatology Life Quality Index, SCORing Atopic Dermatitis (SCORAD), Patient Oriented Eczema Measure, and The Short Form 36 Health Survey (SF-36v2) scores. One study identified a similar immune response in patients taking tralokinumab to those taking the Tdap and meningococcal vaccines. Upper respiratory infection, conjunctivitis, and headaches were the most common adverse events. The varying criteria to assess changes in AD disease severity across different studies is a limitation of this review. Tralokinumab is another promising biologic option for the treatment of moderate to severe AD, which may reduce disease burden and improve patient quality of life.
Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin disorder with an estimated prevalence of 2.1–4.9% of adults in North America.Citation1 AD is associated with pain, sleep disruption, anxiety, and depression and may contribute to a substantial disease burden among patients.Citation2 New treatments for AD target the inflammatory pathways driving its pathogenesis, improving the physical and mental well-being of patients.Citation2
The type 2 cytokine, interleukin (IL)-13, is a key factor in the pathogenesis of AD and is implicated in skin barrier disruption, inflammation, increased risk of skin infections, itch signaling, and epidermal hyperplasia.Citation1 Elevated IL-13 levels are associated with greater AD severity; reductions in IL-13 levels correlate with treatment response and improved clinical outcomes.Citation3 Tralokinumab is a fully human IgG4 monoclonal antibody that binds specifically to IL-13 and blocks downstream IL-13 signaling.Citation1 Tralokinumab was US Food and Drug administration (FDA) approved for the treatment of moderate to severe AD on December 28, 2021.Citation4 In this article, we review the efficacy and safety of tralokinumab for the treatment of moderate to severe AD.
Methods
PubMed and Google Scholar searches were performed using the key words tralokinumab, tralokinumab and atopic dermatitis, tralokinumab dermatology, tralokinumab efficacy, and tralokinumab adverse effects. Articles published between 2017 and 2022 were considered if they included efficacy or safety data related to tralokinumab for the treatment of AD. The authors prescreened abstracts from the search return to determine relevance to the topic. Additional articles were identified by reviewing reference lists from key articles.
Results
We identified seven randomized controlled trials assessing the efficacy and AEs associated with tralokinumab for the treatment of moderate to severe AD.Citation1–Citation3,Citation5–Citation8
Efficacy
Tralokinumab is effective in reducing the disease burden of patients with moderate to severe AD. In two 52-week, randomized, double-blind, placebo-controlled, Phase III trials (ECZema TRAlokinumab Trial No. 1 (ECZTRA 1) and ECZema TRAlokinumab Trial No. 2 (ECZTRA 2)), patients with moderate-to-severe AD were randomized to either subcutaneous tralokinumab 300 mg every two weeks or placebo.Citation1 In ECZTRA 1 and ECZTRA 2, more patients who received tralokinumab compared to placebo achieved an IGA score of 0 or 1 at week 16 (15.8% vs 7.1%, P=0.002 in ECZTRA 1; 22.2% vs 10.9%, P<0.001 in ECZTRA 2); and more patients on tralokinumab attained Eczema Area Severity Index 75 (EASI 75) compared to placebo, in both trials (25.0% vs 12.7%, P<0.001 ECZTRA 1 and 33.2% vs 11.4%, P<0.001 ECZTRA 2).Citation1
Patients treated with tralokinumab also had improvements in pruritus, sleep interference, Dermatology Life Quality Index (DLQI), SCORing Atopic Dermatitis (SCORAD) and Patient-Oriented Eczema Measure (POEM) scores, and response was maintained until week 52 without any rescue medication ().Citation1
Table 1 Efficacy and Safety of Tralokinumab for the Treatment of Moderate to Severe Atopic Dermatitis
In a phase IIb study, 204 healthy adults were randomized 1:1:1:1 to receive 45, 150, or 300 mg of subcutaneous tralokinumab, or placebo, every two weeks for 12 weeks with concomitant topical corticosteroids (TCS).Citation3 At week 12, the 300 mg tralokinumab group had a greater change from baseline in EASI score (−8.76 to −1.13; P = 0.01), a greater percentage of patients achieving an IGA score of 0/1 (26.7% vs 11.8%, P = 0.06), as well as greater improvements in SCORAD (−15.91 to −3.77; P = 0.002), DLQI (−6.00 to −1.02; P = 0.006), and Pruritus Numeric Rating Scale scores (NRS) (−1.88 to −0.41; P = 0.002), compared to placebo, respectively ().Citation3
In a multicenter, parallel, randomized, double-blind, placebo-controlled, phase III trial, 277 European patients with severe AD were randomized 1:1 to subcutaneous tralokinumab 300 mg or placebo every two weeks, plus TCS as needed for 26 weeks.Citation5 At week 16, more patients treated with tralokinumab plus TCS vs placebo plus TCS achieved EASI 75 (64.2% vs 50·5%, P = 0.018), including patients who had previously failed conventional therapy (57% vs 41%), and this further increased up to week 26.Citation5 Patients treated with tralokinumab plus TCS also reported greater improvements in DLQI (–11.2 vs –9.6; P = 0.009), POEM score, pruritus (45.5% vs 35.6%, P = 0.106) and sleep interference, compared to those treated with placebo plus TCS ().Citation5
Tralokinumab improved symptom severity at both early and extended time points. In a double-blind, randomized, placebo-controlled phase III trial, patients were randomized 2:1 to subcutaneous tralokinumab 300 mg or placebo every two weeks, with TCS as needed, over 16 weeks.Citation6 More patients treated with tralokinumab achieved an IGA score of 0 or 1 (38.9% vs 26.2%, P = 0.015) and EASI 75 (56.0% vs 35.7%, P < 0.001) at week 16, compared to placebo.Citation6 Among patients treated with tralokinumab twice weekly who responded at week 16, 89.6% maintained an IGA of 0/1 and 92.5% maintained an EASI 75 until week 32.Citation6 Among responders who were treated four times weekly with tralokinumab, 77.6% and 90.8% maintained an IGA score of 0/1 and an EASI 75 response at week 32, respectively.Citation6 Even among patients who did not achieve these changes in IGA and EASI 75 at week 16, 30.5% and 55.8% achieved these endpoints, respectively, at week 32 ().Citation6
Patients treated with tralokinumab also reported improvements in multiple aspects of their quality of life. In a phase IIb, randomized, double-blind, placebo-controlled, dose-ranging study in 204 adults with moderate-to-severe AD, patients received subcutaneous tralokinumab or placebo (1:1:1:1, 45 mg, n = 50; 150 mg, n = 51; 300 mg, n = 52) every two weeks for 12 weeks, along with a class three TCS cream or ointment at least once daily.Citation2 Patients treated with tralokinumab 300 mg had greater improved DLQI scores at week 12 compared to placebo (−6.00 to −1.02).Citation2 The Mental Component Summary (MCS), Physical Component Summary (PCS), and all eight domains of the Short Form 36 Health Survey (SF-36v2) also improved in patients treated with tralokinumab 300 mg compared to placebo. Sleep interference improved at week 12 compared to placebo among all doses of tralokinumab ().Citation2
Despite its ability to control inflammation through regulation of the IL-13 pathway, tralokinumab does not appear to have a clinically meaningful effect on immune response to vaccines. ECZema TRAlokinumab Trial No. 5 (ECZTRA 5) was a phase II, double-blind, randomized, placebo-controlled trial of 215 adults randomized 1:1 to either tralokinumab 300 mg or placebo every two weeks, for 16 weeks.Citation7 At week 12, all patients received Tdap (tetanus/diphtheria/pertussis) and meningococcal vaccines.Citation7 Tralokinumab treated patients produced a similar immune response to Tdap (91.9% vs 96.1%) and meningococcal (86.0% vs 84.2%) vaccines compared to placebo at week 16 ().Citation7
Adverse Effects
In the ECZTRA 1 and 2 trials, AEs were reported in 76.4% and 61.5% of tralokinumab patients at week 16, respectively, compared to 77.0% and 66.0% of patients receiving placebo.Citation1 Among the AEs reported in ≥ 5% in any treatment group, upper respiratory infection and conjunctivitis occurred more frequently in the tralokinumab groups, while dermatitis and skin infection occurred more often in the placebo groups.Citation1 Conjunctivitis occurred in ≤ 10% of patients treated with tralokinumab in the initial treatment periods and in < 9% of those in the maintenance periods.Citation1 Most of the cases of conjunctivitis were mild or moderate, and only one case led to patient withdrawal ().Citation1
Similarly, in a meta-analysis of five randomized, placebo-controlled trials of tralokinumab in adult patients with moderate-to-severe AD, the incidence of conjunctivitis was also higher with tralokinumab compared to placebo (7.5% vs 3.2%).Citation8 Most events were mild or moderate in severity and resolved during the trial in both treatment and placebo groups.Citation8 Two events led to discontinuation of tralokinumab.Citation8 An increased incidence of conjunctivitis was associated with more severe AD, a history of allergic conjunctivitis/atopic keratoconjunctivitis, and a number of atopic comorbidities regardless of treatment group.Citation6 Conjunctivitis has been observed in other studies of IL-4 or IL-13 inhibitors, but its etiology is still unknown.Citation1
In another study, the safety profile of tralokinumab in patients with AD was similar to that of asthma patients treated with tralokinumab.Citation3 Upper respiratory infections and headaches were the most common AEs; however, the majority of AEs were mild or moderate ().Citation3
Discussion
Tralokinumab has an acceptable efficacy and safety profile and provides early and sustained improvements in disease severity among patients with moderate-to-severe AD.Citation3 Clinical efficacy was greatest in participants treated with 300 mg of tralokinumab.Citation3 Tralokinumab presents another biologic option for the treatment of moderate to severe AD that, similar to dupilumab, exhibits improvements in EASI, SCORAD, pruritus, NRS, POEM, DLQI, and IGA and also targets the IL-13 proinflammatory pathway in adults () (). There are currently limited studies comparing tralokinumab to other systemic AD treatments, but the current data suggest tralokinumab improves subjective and objective measures of disease severity in AD patients.Citation1–Citation3,Citation9
Table 2 Mean Difference in Eczema Area and Severity Index, Patient-Oriented Eczema Measure, and Dermatology Life Quality Index for Systemic Treatments for Atopic Dermatitis
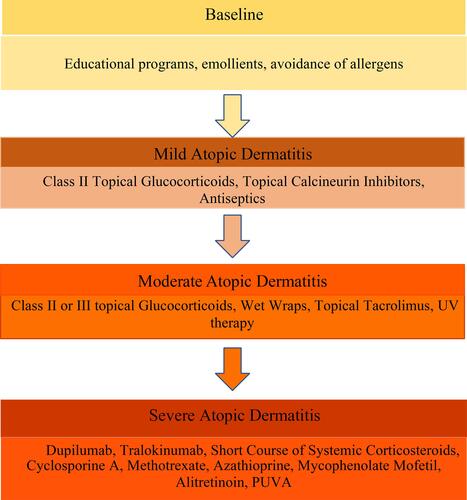
Figure 1 Treatment paradigm of atopic dermatitis modified from consensus based European guidelines for treatment of eczema (atopic dermatitis) in adults and children.
Tralokinumab has the additional benefits of decreasing S. aureus colonization, reducing the need for systemic treatment of skin infections, and decreasing the frequency of eczema herpeticum.Citation1 These added benefits may be due to tralokinumab’s ability to improve skin barrier integrity or its regulation of IL-13 leading to increased expression of antimicrobial genes.Citation1
Tralokinumab IGA and EASI responses were maintained over 36 weeks without active maintenance treatment or TCS, in the ECZTRA 1 and 2 trials, suggesting tralokinumab may induce remission of AD for some patients.Citation1 Some patients initially treated four times a week were able to maintain good disease control after stopping treatment, suggesting the possibility of less frequent maintenance dosing in some patients initially treated with a higher dose.Citation1
The objective improvements seen with tralokinumab treatment are clinically meaningful; patients treated with 300 mg tralokinumab two times a week had greater improvements in all 6 subscales of DLQI compared with placebo.Citation2 Among patients treated with tralokinumab 300 mg twice weekly, there were also improvements in both MCS and PCS and in all eight domains of SF-36v2.Citation2 Tralokinumab improves many aspects of patients’ health-related quality of life.Citation2
Conclusion
Tralokinumab improves IGA, EASI 75, SCORAD, and POEM scores comparable to other systemic AD treatments ().Citation1,Citation3,Citation5,Citation6 These improvements in symptom severity are apparent at both short and extended time points.Citation6 Tralokinumab’s improvements in objective clinical outcomes is paralleled by improvements in multiple aspects of patients’ quality of life.Citation2 Tralokinumab exhibits a good safety profile. Upper respiratory infection, conjunctivitis, and headaches are AEs commonly seen in patients treated with tralokinumab, but are usually mild to moderate.Citation1,Citation3,Citation8 Tralokinumab presents another promising biologic option for the treatment of AD which may directly target inflammatory pathways, reduce disease burden, and improve patient quality of life.
Disclosure
Dr. Steven R Feldman has received research, speaking and/or consulting support from Galderma, GSK/Stiefel, Almirall, Leo Pharma, Boehringer Ingelheim, Mylan, Celgene, Pfizer, Valeant, AbbVie, Samsung, Janssen, Lilly, Menlo, Merck, Novartis, Regeneron, Sanofi, Novan, Qurient, National Biological Corporation, Caremark, Advance Medical, Sun Pharma, Suncare Research, Informa, UpToDate and National Psoriasis Foundation. He is founder and majority owner of www.DrScore.com and founder and part owner of Causa Research, a company dedicated to enhancing patients’ adherence to treatment. Katherine A Kelly and Patrick O Perche have no conflicts of interest to disclose in this work.
Additional information
Funding
References
- Wollenberg A, Blauvelt A, Guttman-Yassky E, et al. Tralokinumab for moderate-to-severe atopic dermatitis: results from two 52-week, randomized, double-blind, multicentre, placebo-controlled phase III trials (ECZTRA 1 and ECZTRA 2)*. Br J Dermatol. 2021;184(3):437–449. doi:10.1111/bjd.19574
- Silverberg JI, Guttman-Yassky E, Gooderham M, et al. Health-related quality of life with tralokinumab in moderate-to-severe atopic dermatitis: a phase 2b randomized study. Ann Allergy Asthma Immunol. 2021;126(5):576–583.e4. doi:10.1016/j.anai.2020.12.004
- Wollenberg A, Howell MD, Guttman-Yassky E, et al. Treatment of atopic dermatitis with tralokinumab, an anti–IL-13 mAb. J Allergy Clinl Immunol. 2019;143(1):135–141. doi:10.1016/j.jaci.2018.05.029
- FDA approves adbry for treatment of moderate-to-severe atopic dermatitis [internet]. [ cited 2022 January 23]. Available from: https://www.pharmacytimes.com/view/fda-approves-adbry-for-treatment-of-moderate-to-severe-atopic-dermatitis. Accessed June 1, 2022.
- Gutermuth J, Pink AE, Worm M, Soldbro L, Bjerregård Øland C, Weidinger S. Tralokinumab plus topical corticosteroids in adults with severe atopic dermatitis and inadequate response to or intolerance of ciclosporin A: a placebo‐controlled, randomized, phase III clinical trial (ECZTRA 7). Br J Dermatol. 2021;186:440–452. doi:10.1111/bjd.20832
- Silverberg JI, Toth D, Bieber T, et al. Tralokinumab plus topical corticosteroids for the treatment of moderate-to-severe atopic dermatitis: results from the double-blind, randomized, multicentre, placebo-controlled phase III ECZTRA 3 trial*. Br J Dermatol. 2021;184(3):450–463. doi:10.1111/bjd.19573
- Merola JF, Bagel J, Almgren P, et al. Tralokinumab does not impact vaccine-induced immune responses: results from a 30-week, randomized, placebo-controlled trial in adults with moderate-to-severe atopic dermatitis. J Am Acad Dermatol. 2021;85(1):71–78. doi:10.1016/j.jaad.2021.03.032
- Wollenberg A, Beck LA, de Bruin Weller M, et al. Conjunctivitis in adult patients with moderate-to-severe atopic dermatitis: results from five tralokinumab clinical trials. Br J Dermatol. 2021;186:453–465.
- Drucker AM, Ellis AG, Bohdanowicz M, et al. Systemic immunomodulatory treatments for patients with atopic dermatitis: a systematic review and network meta-analysis. JAMA Dermatol. 2020;156:659. doi:10.1001/jamadermatol.2020.0796
- Silverberg JI, Simpson EL, Thyssen JP, et al. Efficacy and safety of abrocitinib in patients with moderate-to-severe atopic dermatitis: a randomized clinical trial. JAMA Dermatol. 2020;156(8):863. doi:10.1001/jamadermatol.2020.1406
- Fadlalmola HA, Albadrani MS, Elhusein AM, Mohamedsalih WE, Swamy VDS, Mamanao DM. Effectiveness and safety of abrocitinib in patients with moderate-to-severe atopic dermatitis: a systematic review and meta-analysis of randomized clinical trials. Dermatol Res Pract. 2021;2021:1–13. doi:10.1155/2021/8382761
- Reich K, DeLozier AM, Nunes FP, et al. Baricitinib improves symptoms in patients with moderate-to-severe atopic dermatitis and inadequate response to topical corticosteroids: patient-reported outcomes from two randomized monotherapy phase III trials. J Dermatol Treat;2020. 1–10. doi:10.1080/09546634.2020.1839008
- Guttman-Yassky E, Blauvelt A, Eichenfield LF, et al. Efficacy and safety of lebrikizumab, a high-affinity interleukin 13 inhibitor, in adults with moderate to severe atopic dermatitis: a phase 2b randomized clinical trial. JAMA Dermatol. 2020;156(4):411. doi:10.1001/jamadermatol.2020.0079
- Silverberg JI, Pinter A, Pulka G, et al. Phase 2B randomized study of nemolizumab in adults with moderate-to-severe atopic dermatitis and severe pruritus. J Allergy Clinl Immunol. 2020;145(1):173–182. doi:10.1016/j.jaci.2019.08.013
- Knox S, Mahr T. trial of nemolizumab and topical agents for atopic dermatitis with pruritus. Pediatrics. 2021;148(Supplement 3):S19–S19. doi:10.1542/peds.2021-053843Z
- Simpson EL, Parnes JR, She D, et al. Tezepelumab, an anti–thymic stromal lymphopoietin monoclonal antibody, in the treatment of moderate to severe atopic dermatitis: a randomized phase 2a clinical trial. J Am Acad Dermatol. 2019;80(4):1013–1021. doi:10.1016/j.jaad.2018.11.059
- Saeki H, Kabashima K, Tokura Y, et al. Efficacy and safety of ustekinumab in Japanese patients with severe atopic dermatitis: a randomized, double-blind, placebo-controlled, Phase II study. Br J Dermatol. 2017;177(2):419–427. doi:10.1111/bjd.15493