
Abstract
Cutaneous mucinosis is a rare disease that manifests as an excessive accumulation of mucin in the skin that forms waxy papules or plaques. We report a case of a 44-year-old male psoriatic patient who developed generalized cutaneous mucinosis after 11 months of biological treatment. The patient had a history of psoriasis for 20 years and had been treated with narrow-band UVB phototherapy, methotrexate, or acitretin intermittently. He was started on etanercept after he was diagnosed with psoriatic arthritis, and 11 months later, he complained of swelling in his extremities and myxoid cysts on his fingers. Etanercept was then discontinued due to loss of efficacy and widespread skin lesions. However, the lesions subsided spontaneously after 6 months without specific systemic treatment.
Introduction
Cutaneous mucinoses are a group of rare conditions involving an excessive accumulation of mucin in the skin. Usually, they are divided into primary, in which mucin deposition is the major histologic feature resulting in clinically distinctive lesions (eg, scleromyxedema, lichen myxedematosus, scleredema, cutaneous focal mucinosis, digital mucous cyst, self-healing juvenile cutaneous mucinosis, cutaneous mucinosis of infancy and other miscellaneous mucinoses); and secondary, in which mucin simply represents an associated histologic finding as in diseases like basal cell carcinoma, lupus erythematosus, dermatomyositis, Degos disease, and granuloma annulare, etc.Citation1 Histological mucin deposition can be associated with various inflammatory or neoplastic cutaneous disorders.Citation2 However, few reports of cutaneous mucin deposition in patients with psoriasis were found. Herein, we present a unique case of a psoriatic patient who developed generalized cutaneous mucinosis during treatment of etanercept and resolved spontaneously.
Case Report
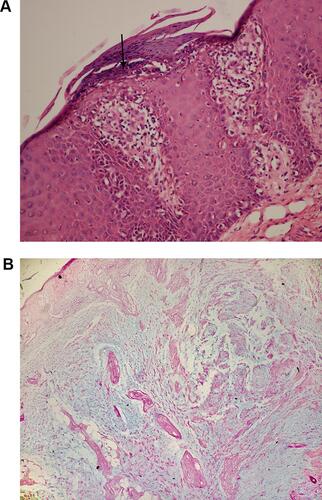
A 44-year-old Chinese male patient with a 20-year history of psoriasis and a 1-year history of psoriatic arthritis presented with erythroderma, non-pruritic, non-tender lesions on the upper trunk and extremities, abscesses with mucoid discharge on the joints and arthralgia for 1 month. He had been treated with etanercept (25mg, subcutaneously twice per week) after being diagnosed with psoriatic arthritis. Before etanercept, he received 78 sessions of narrow-band UVB phototherapy, methotrexate (discontinued due to elevated liver enzymes after 1 year), and acitretin (discontinued by himself after 2 years). Past medical history was unremarkable. Eleven months after initiating etanercept, the above-described lesions and multiple affected joints were observed on the body. Etanercept was then discontinued due to gradual loss of efficacy and the extensive lesions. Skin examination revealed erythroderma with thickened skin, well-demarcated, brownish lichenification on the back, swelling of extremities and some small joints, lichenification on the knees and toes, and sunken scars on the right leg. Myxoid cysts, which could spontaneously break open, were found on the arms and finger joints (). Biopsy of the skin near the abscess on the right shin showed marked hyperkeratosis with parakeratosis and Munro micro-abscesses formation in the epidermis. Acanthosis, irregular elongation of rete ridges, and dilation of papillary blood vessels could be seen (). Alcian blue stain showed mucus cells and excessive mucin deposition in the dermis (). Based on clinical and histopathological findings, a diagnosis of generalized cutaneous mucinosis was established.
Figure 1 Erythroderma and thickened skin, with lichenification on some parts of the back (A). Swelling of the legs, lichenification on the knees and toes, and sunken scars on the right leg (B). Myxoid cyst, erythema, and scales were noted on the patient’s fingers (C). Swelling of metacarpophalangeal joint of left thumb with psoriatic involvement on each nail (D).

Figure 2 Pathological section showing hyperkeratosis with parakeratosis and Munro micro-abscess (arrow) formation in the epidermis (Hematoxylin and Eosin, ×400) (A). Alcian blue stain showing excessive mucin deposition in the dermis (Alcian blue, ×200) (B).
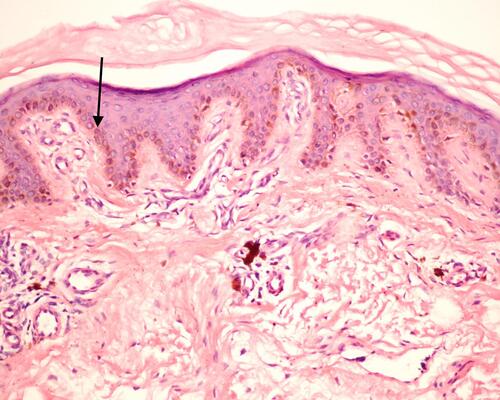
Laboratory tests showed normal liver, kidney, and thyroid function. The patient received topical corticosteroid ointments twice daily, which gave little clinical improvement within 1 month. However, to our surprise, at a 6-month follow-up, he returned with complete resolution of the lesions and swelling of joints and extremities, leaving hyperpigmented spots throughout the body ( and ). The patient denied any systemic treatment. Another skin biopsy was then taken from the right arm’s pigmented lesion, which showed no mucin deposition in the dermis (). The psoriasis lesions and arthralgia reappeared a few months later, while the mucinous lesions did not reoccur.
Figure 3 Complete resolution of the lesions leaving hyperpigmented spots throughout the body after 6 months (A). Complete regression of skin, nail lesions, and the swelling joint (B).
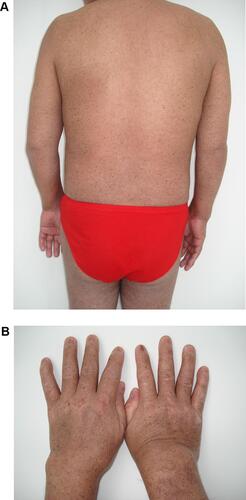
Figure 4 Pathological section showing pigmentation on the basal layer (arrow), and pigmentophages found in the dermis. No mucin deposition was noted (H&E, ×200).
Discussion
Cutaneous mucinosis is a heterogeneous group of disorders with an abnormal accumulation of mucin, which can be subdivided into primary and secondary. The pathogenesis and etiology of cutaneous mucinosis are not well established.Citation3 Mucin is a component of the dermal extracellular matrix mainly composed of the glycosaminoglycan hyaluronic acid (HA) and is produced by fibroblasts in the skin or within the hair follicles.Citation1 Mucin deposition can be found as a secondary manifestation in many diseases such as mycosis fungoides, basal cell carcinoma, lupus erythematosus, and so on.Citation1 However, cutaneous mucinosis associated with psoriasis is very rare in literature. The presented case describes the extremely rare coexistence of generalized cutaneous mucinosis, erythrodermic psoriasis, and psoriatic arthritis.
Etanercept is a tumor necrosis factor-alpha (TNF-α) antagonist, which was approved in the United States for treating psoriatic arthritis (2002)Citation4 and moderate-to-severe plaque psoriasis (2004).Citation5 Common cutaneous adverse events including injection site reactions, eczematous lesions, psoriasiform eruptions, drug-induced lupus erythematosus, vasculitis, cutaneous infections, and cutaneous malignant neoplasms.Citation6 Literatures about cutaneous mucinosis associated with biological treatment are scarce. Lesiak et alCitation7 reported a case of a 66-year-old woman who developed cutaneous focal mucinosis after a 2-month treatment of ustekinumab and had failed two TNF inhibitors before ustekinumab. The authors attributed the mucin deposition to the 1.5 years of exposure to TNF inhibitors. In another case,Citation8 the patient had a very similar treatment course like that in Lesiak’s case and presented with lichen myxedematosus. An additional case in the French language also suggested TNF inhibitors as a potential cause of the patient’s multiple lesions of cutaneous focal mucinosis.Citation9
Although the etiopathogenesis of the disease is unknown, it is implicated that cytokines, such as interleukin-1, TNF, transforming growth factor-β, or interferon-γ (IFN-γ) may play a role in the stimulation of HA synthesis by dermal fibroblasts or dendritic cells.Citation7,Citation8 The possibility of anti-TNFα biological therapy may have an impact on mucin formation could not be excluded. A possible explanation is that etanercept, which is a TNF inhibitor, may indirectly activate fibroblasts to produce mucin by reducing the amount of active TNF. The reduction of active TNF makes skin dendritic cells increase the production of IFN-α, which likely activates lymphocytes and thus stimulates fibroblasts to produce mucin.Citation10 Siewert et alCitation11 may have confirmed this hypothesis by reporting that a patient receiving IFN-α con-1 for chronic hepatitis C treatment developed cutaneous mucinosis at the injection sites. Another pathological mechanism that might cause excessive mucin production is the lack of inhibitory effect of TNF-α on skin dendritic cell populations.Citation12
In our case, it is hard to understand that both psoriatic erythroderma and mucinous lesions dramatically regressed after stopping etanercept and with only intermittent topical steroids treatment. Few case reports describing the coexistence of erythroderma and mucinosis were found. FujimuraCitation2 described an 81-year-old Japanese patient with erythroderma (not psoriatic erythroderma) overlapped with widespread mucin deposition. The authors concluded that generalized mucinosis is secondary to erythroderma. Tay et alCitation13 reported a patient with a 12-year history of long-term psoriatic erythroderma treated with corticosteroids, methotrexate, and mercaptopurine was discovered to have papular mucinosis on the trunk and upper limbs. In this case, the authors felt that the papular mucinosis is perhaps a chance association. There is no established therapeutic modality for generalized mucinosis. Multiple treatments including retinoids, plasmapheresis, high-dose intravenous immunoglobulin, topical and intralesional hyaluronidase, topical, intralesional, and systemic corticosteroids, and psoralen plus ultraviolet A (PUVA) have been tried based on case reports or experiences.Citation3 Although both the erythroderma and generalized mucinosis may respond to topical steroids, the healing of the patient’s generalized mucinosis may be mainly due to the remission of erythroderma.
In summary, to the best of our knowledge, it is the first case of generalized cutaneous mucinosis developed during the anti-TNF-α treatment of psoriasis. The underlying mechanism is needed to be understood. Biologic agents are more and more widely used in dermatologic practice; thus, new possible adverse reactions should be noted.
Ethics Statement
Informed consent for publication of the case report and associated images was obtained from the patient. Institutional approval was not required to publish the case details.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Rongioletti F, Rebora A. The new cutaneous mucinoses: a review with an up-to-date classification of cutaneous mucinoses. J Am Acad Dermatol. 1991;24(2 Pt 1):265–270. doi:10.1016/0190-9622(91)70040-9
- Fujimura T, Okuyama R, Nakagawa S, Terui T, Aiba S. Generalized mucinosis in a patient with erythroderma. Dermatology. 2006;212(4):366–369. doi:10.1159/000092288
- Jackson EM, English JC. Diffuse cutaneous mucinoses. Dermatol Clin. 2002;20(3):493–501. doi:10.1016/S0733-8635(02)00017-7
- U.S. Food & Drug Administration. Product Approval Information - Licensing Action. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2002/etanimm011502L.htm. Accessed March 29, 2022.
- Papp KA. Etanercept in psoriasis. Expert Opin Pharmacother. 2004;5(10):2139–2146. doi:10.1517/14656566.5.10.2139
- Moustou AE, Matekovits A, Dessinioti C, Antoniou C, Sfikakis PP, Stratigos AJ. Cutaneous side effects of anti-tumor necrosis factor biologic therapy: a clinical review. J Am Acad Dermatol. 2009;61(3):486–504. doi:10.1016/j.jaad.2008.10.060
- Lesiak A, Włodarczyk M, Sobolewska A, et al. Can biologic treatment induce cutaneous focal mucinosis? Postep Dermatologii i Alergol. 2014;31(6):413–416. doi:10.5114/pdia.2014.40944
- Garber C, Rosmarin D, Nguyen B, et al. Cutaneous mucinosis in a patient taking ustekinumab for palmoplantar psoriasis. Dermatol Online J. 2017;23(3):5.
- Duparc A, Gosset P, Lasek A, Modiano P. Mucinose cutanée focale multiple: rôle des anti-TNF alpha? Ann Dermatol Venereol. 2010;137(2):140–142. doi:10.1016/j.annder.2010.01.001
- Nestle FO, Conrad C, Tun-Kyi A, et al. Plasmacytoid predendritic cells initiate psoriasis through interferon-alpha production. J Exp Med. 2005;202(1):135–143. doi:10.1084/jem.20050500
- Siewert E, Weyers W, Dietrich CG, Geier A, Lammert F, Matern S. Cutaneous mucinosis and skin necrosis complicates interferon alfacon-1 (consensus interferon) treatment of chronic hepatitis C. Eur J Med Res. 2005;10(2):63–67.
- Aeberli D, Oertle S, Mauron H, Reichenbach S, Jordi B, Villiger PM. Inhibition of the TNF-pathway: use of infliximab and etanercept as remission-inducing agents in cases of therapy-resistant chronic inflammatory disorders. Swiss Med Wkly. 2002;132(29–30):414–422.
- Tay CH, Khoo OT. Papular Mucinosis in Chronic Psoriatic Erythroderma: report of a Case. Arch Dermatol. 1970;102(3):304–308. doi:10.1001/archderm.1970.04000090066010