
Abstract
Facial flushing affects the work and life of patients. The specific pathogenesis and conditions of facial flushing may be complicated. A 47-year-old perimenopausal woman was presented to the Pain Management with a 4-month history of facial flushing. The patient didn’t have any history of special illness or history of allergies. Treatments with methylprednisolone, thalidomide, hydroxychloroquine drugs or sympathetic blockages (stellate ganglion block) were unable to effectively improve the symptoms. We believed that the facial flushing might be associated with the anxiety. After two weeks of venlafaxine medication, the symptoms were 90% relieved. We found that venlafaxine effectively improved flushing that may be related to anxiety.
Keywords:
Introduction
Facial flushing affects the work and life of patients, and its specific pathogenesis and conditions may be complicated.Citation1 Here we introduce the diagnosis and treatment process of a case of bilateral flushing.
Case Presentation
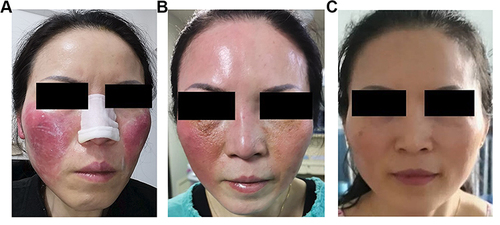
A 47-year-old perimenopausal woman was presented to the Pain Management with a 4-month history of facial flushing. She was obviously anxious. The facial flushing in her face occurred in both sides with postural changes, thermal stimulation and mood changes. One month ago, the symptoms of this patient were aggravated. Symptoms including skin burning sensation and sleep difficulty appeared. The patient was unable to sleep flat and slept only 2–3 hours per day (). In addition, the patient didn’t have any history of special illness or history of allergies. A variety of tests were done with her body, including autoimmunity antibody test, skull MRI test, however, nothing abnormal was found. What’s more, treatments with drugs (methylprednisolone, thalidomide, hydroxychloroquine, glycyrrhizic anhydride tablets, ketotifen) or 10 times sympathetic blockages (stellate ganglion block) were unable to effectively improve the symptoms (). We invited dermatology, rehabilitation, hematology and other departments for consultation and multidisciplinary cooperation, and invited experts from higher-level hospitals for consultation, but no definite cause was found. We discussed the condition with the psychologist again, and finally we believed that the facial flushing might be associated with the anxiety. Venlafaxine inhibits the reuptake of serotonin and norepinephrine. We discussed the use of venlafaxine with the hospital pharmacy department and informed the patient. Then, venlafaxine was used. Miraculously, the facial flushing was markable improved in the following days. After two weeks of medication, the symptoms were 90% relieved. The patient was satisfied with the treatment, and the mood state improved significantly. Finally, the facial flushing of the patient was disappeared after taking venlafaxine for three months ().
Figure 1 The facial flushing Changes during treatment. (A) bilateral facial flushing before therapy; (B) state after stellate ganglion block; (C) facial flushing was markable improved by venlafaxine.
Discussion
Perimenopausal women are prone to anxiety, and there may be abnormalities in sympathetic nerve function and vasomotor function.Citation2,Citation3 In addition, Jenifer et al found that venlafaxine may improve female hot flashes by regulating skin capillary perfusion.Citation4 In fact, venlafaxine is a commonly used norepinephrine reuptake inhibitor and serotonin modulator, which can effectively improve anxiety and depression.Citation5
Rosacea is a chronic, inflammatory skin disease that affects cheeks, nose, chin, and forehead. Rosacea is characterized by episodes of exacerbation and remission. The diagnosis of rosacea is based on clinical features and careful history taking. The differential diagnosis includes seborrheic dermatitis, flushing disorders, lupus erythematosus, etc.Citation6 A recent systematic reviews showed that rosacea may predispose patients to develop depression and anxiety.Citation7 In this case, the patient’s facial redness has consulted to the dermatology department, and we invited dermatology, rehabilitation, hematology and other departments for consultation and multidisciplinary cooperation. Considering the patient’s extreme anxiety and the good treatment effect of venlafaxine, as well as the follow-up situation, we believed that facial flushing caused by anxiety, but do not rule out rosacea. In addition, beta-blockers propranolol, carvedilol and clonidine were recommended first-line treatment in rosacea flushing.Citation6,Citation8 Venlafaxine inhibits the reuptake of serotonin and norepinephrine. Following treatment with venlafaxine, there was a reduction in flushing and endothelial dependent perfusion response in postmenopausal women.Citation4 We agree that rosacea may also benefit from venlafaxine. This is very interesting and deserves further study.
In this case report, we found that venlafaxine may improve bilateral flushing by improving patient anxiety. However, its specific mechanism remains to be explored.
Conclusion
In conclusion, we found that venlafaxine effectively improved facial flushing that may be related to anxiety.
Data Sharing Statement
The original data and materials are available from the corresponding author on reasonable request.
Ethical/Copyright Statement
Written informed consent was provided by the patients to have the case details and any accompanying images published. The ethics committee of Zigong First People’s Hospital approved this consent process and approved to publish the case details. There is no Ethical/Copyright concern.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
Acknowledgments
The authors thank the patient for her cooperation.
Additional information
Funding
References
- Mc CO, Reynolds JV. Images in clinical medicine. Intermittent facial flushing and diarrhea. N Engl J Med. 2014;371(3):260. doi:10.1056/NEJMicm1314969
- Muslić L, Jokić-Begić N. The experience of perimenopausal distress: examining the role of anxiety and anxiety sensitivity. J Psychosom Obstet Gynaecol. 2016;37(1):26–33. doi:10.3109/0167482X.2015.1127348
- Avis NE, Crawford SL, Greendale G, et al. Duration of menopausal vasomotor symptoms over the menopause transition. JAMA Intern Med. 2015;175(4):531–539. doi:10.1001/jamainternmed.2014.8063
- Sassarini J, Krishnadas R, Cavanagh J, et al. Venlafaxine alters microvascular perfusion, [¹²³I]-beta-CIT binding and BDI scores in flushing postmenopausal women. Maturitas. 2014;77(3):267–273. doi:10.1016/j.maturitas.2013.12.003
- Rickels K, Gallop R, Cleary S. The course of adverse events in venlafaxine XR treatment in generalized anxiety disorder. J Clin Psychopharmacol. 2019;39(3):258–260. doi:10.1097/JCP.0000000000001027
- van Zuuren EJ, Solomon CG. Rosacea. N Engl J Med. 2017;377(18):1754–1764. doi:10.1056/NEJMcp1506630
- Chang HC, Huang YC, Lien YJ, Chang YS. Association of rosacea with depression and anxiety: a systematic review and meta-analysis. J Affect Disord. 2022;299:239–245. doi:10.1016/j.jad.2021.12.008
- Zhang H, Tang K, Wang Y, Fang R, Sun Q. Rosacea Treatment: review and Update. Dermatol Ther. 2021;11(1):13–24. doi:10.1007/s13555-020-00461-0