
Abstract
Introduction
The psychological impact of dandruff has been largely understudied.
Methods
In this cross-sectional study (N = 2116), we examined the consequences of self-perception of dandruff severity on mental health, quality of life, and sleep quality among Chinese adults. Additionally, we examined the moderating factors that influence these associations.
Results
Bivariate analyses revealed that greater self-perceived dandruff severity was associated with poorer mental health, lower quality of life, and reduced sleep quality. Furthermore, dandruff severity was positively correlated with appearance anxiety, feelings of helplessness, and perceived stigma. Individuals with more severe dandruff experienced increased teasing and ostracism and, subsequently, heightened psychological distress. Moderation analyses demonstrated that females were more adversely affected by dandruff than males, and those with comorbid skin conditions or a history of being teased and ostracized during adolescence due to dandruff experienced exacerbated negative outcomes.
Discussion
This study highlights the need for further research on the psychological consequences of self-perceived severity of dandruff and potential interventions to mitigate its impact.
Introduction
Dandruff is a common affliction of the human scalp.Citation1 A wide range of symptoms is associated with dandruff, the most common of which are visible skin flakes, itch, and dryness.Citation2,Citation3 Pityriasis sicca, frequently regarded as a mild form of dandruff, primarily manifests through dry, fine, non-inflammatory scaling of the scalp.Citation4 Seborrheic dermatitis, which has received more medical attention, is the same condition as dandruff, differing only in magnitude in terms of locality and severity.Citation5 The etiology of dandruff, pityriasis sicca, and seborrheic dermatitis involves three facets: sebum, the microbiome component Malassezia, and innate susceptibility.Citation6 Malassezia metabolism alters scalp surface sebaceous triglycerides to yield free fatty acids that have the potential to initiate inflammation and hyper-proliferation, leading to the aforementioned symptoms. Genetics, skin type, and lifestyle factors, such as diet, air quality, and stress, can also be contributing factors.Citation7,Citation8
While very few studies have specifically investigated the psychological burden associated with dandruff, research on seborrheic dermatitis and other chronic skin diseases such as acne, psoriasis, vitiligo, and atopic dermatitis more generally reveals that patients with dermatological conditions experience psychological distress, including depressive and anxiety symptoms, and decreased quality of life.Citation9–13
The psychological outcomes of skin conditions can stem from the negative impact of the condition on self and social evaluation.Citation14 The physical symptoms of dandruff, such as flaking and itching, can lead to distress and shame, as well as negatively impacting self-image. The visible nature of skin conditions, including dandruff, has been shown to be associated with perceived stigmatization and discrimination, as well as psychological distress.Citation15 In extreme cases, individuals with skin conditions may develop body dysmorphic disorder (BDD), characterized by a preoccupation with perceived appearance defects and repetitive behaviours aimed at concealing, changing, or checking them. BDD is associated with impairment in social functioning and decreased quality of life and self-esteem.Citation16,Citation17
Despite its high prevalence, about 50% of the general adult population worldwide,Citation18 very few empirical studies have explored the mental health impact of dandruff.Citation19 Dandruff differs from other dermatologic conditions in several meaningful ways. First, its onset often occurs during puberty, a time marked by increased importance of and sensitivity toward peer evaluation.Citation20 It is an empirical question as to the extent to which negative social evaluation or bullying caused or exacerbated by dandruff has a lasting impact on psychological wellbeing. Second, other chronic skin conditions such as psoriasis, and alopecia have received ample empirical attention as a medical condition, while some view dandruff as merely an annoyance and not a medical condition. However, as discussed above, its psychosocial consequences can be considerable.
Studies have consistently shown the impact of chronic skin conditionsCitation21 on quality of life and mental health. Emerging studiesCitation21 are also including poor sleep quality a potential outcome because sleep has been demonstrated to be associated with future health and mental health outcomes (eg, via inflammation).Citation22,Citation23 Healthy sleep is a protective factor against various downstream problems.Citation24–27 Contrarily, sleep disturbances can cause and exacerbate health outcomes, and vice versa.Citation28,Citation29 Studies have also found an association between chronic skin disease and sleep disturbances.Citation30–32 The influence of dandruff on sleep quality is yet to be examined.
Individual differences, including gender, comorbidity of other skin conditions, and history of teasing and ostracism due to dandruff, may impact the psychological sequelae of dandruff. Gender differences have been found in certain forms of psychological distress among skin condition patients, with women being more impacted than men.Citation12 The comorbidity of other dermatological conditions may exacerbate the psychological impact of dandruff, and individuals with a history of other skin conditions or teasing and ostracism due to dandruff may be more susceptible to negative psychological effects associated with dandruff. The experience of being teased or ostracized due to dandruff may have a lasting impact on an individual’s self-esteem and confidence, making them more vulnerable to the psychological distress associated with dandruff.
Current Study
The aim of this study was to examine the potential psychosocial consequences of dandruff among Chinese adults and to explore the moderating effects of three factors on its impact on mental health and psychological well-being. Specifically, we investigated the influence of gender, comorbidity of other skin conditions, and history of dandruff-based teasing and ostracism on the psychological sequelae of dandruff.
To achieve this aim, we examined several mental health and psychosocial variables that were identified in the literature on body image and dermatological conditions as potential sequelae of dandruff. We focused on three main outcomes, including quality of life, psychological distress, and sleep quality. The impact of chronic skin conditions on these outcomes has been well established in the literature.Citation21 Therefore, we included sleep quality as an outcome variable, given its prospective association with health and mental health outcomes.Citation28,Citation29
We hypothesized that those with more severe dandruff would have worse quality of life, psychological distress, and sleep quality. Furthermore, we examined the potential influence of dandruff on four psychosocial outcomes, including appearance anxiety, helplessness, stigma, and rejection sensitivity. We hypothesized that dandruff severity is associated with higher levels on these outcomes.
We also examined the potential moderating effects of gender, comorbidity of other skin conditions, and history of teasing and ostracism on the association between dandruff severity and the main mental health and quality of life outcomes. Based on past studies, we hypothesized that women would be more impacted by the increase in severity than men.Citation12 We also hypothesized that individuals with comorbid skin conditions or history of teasing and ostracism would experience a more significant negative impact on their mental health and psychological well-being.Citation22,Citation23 Finally, we hypothesized that those who were teased or ostracized as a teenager for dandruff would be more likely to perceive stigma as their dandruff severity increased.Citation15
Method
Participants and Procedure
Adult participants (ie, those 18 years old and above) were recruited from Beijing, Shanghai, and Guangzhou, three of the largest cities in China through an independent market research agency. Without a priori effect sizes to reference, we chose a conservative small effect size in our sample size calculation. For bivariate associations—r = 0.10, alpha = 0.05, power = 0.95—the required sample size was 1289. To detect the hypothesized (small) moderation effects—f2 = 0.02, alpha = 0.05, power = 0.95—776 participants were needed. The final sample size was 2116.
Participants were purposefully recruited, from a pool of panelists, through email, SMS, and WeChat; they were recruited based on a set of stratification criteria: i) a 1:1 split between females and males; ii) a 1:1:1 split between the three cities; iii) representativeness of different economic status; iv) a 2:1 split between local and non-local residents, based on China’s registry system (“Hukou”); and v) an even distribution across four levels of subjective dandruff severity (more details below; ). The questionnaire was delivered online, participants filled it out independently, and the data was stored on the server of the market research agency. Ethics procedures were approved and followed in accordance with Procter & Gamble’s Human Testing and R&D governance (Study 21–059505) prior to data collection. Data collection was performed in accordance with the guidelines and regulations of American Psychological Association and those of the Declaration of Helsinki. All participants gave written informed consent. Participants were compensated 15 to 42 RMB (approximately USD $2 to $5.8) for their time. The study was conducted in September 2021.
Table 1 Distribution of Sample Size Across Dandruff Severity (N = 2116)
Measures
Dandruff Severity
Two self-report measures were used to assess the subjective severity of dandruff. First, participants chose from eight descriptions of their dandruff severity the one most relevant to them (). These eight descriptions were categorized into four levels of severity: Severe, moderate, light, and not experiencing dandruff. Second, a single-item severity question that asks the participant to rate the severity of their current dandruff in the past seven days, ranging from 0 = “I do not have dandruff” to 3 = “I have severe dandruff.” These measures are similar to those used in previous studies.Citation33
Mental health was measured using five scales, one on general psychological distress, three on social anxiety, and one on perceived stress. The K6Citation34 is a widely used 6-item measure of general psychological distress. The established cutoffs are 0 to 7 = low psychological distress, 8 to 12 = moderate, and 13 and above = severe. A sample item of the K6 is “During the past 30 days, about how often did you feel worthless?” Social anxiety was measured using three scales: Social Interaction Anxiety Scale (SIAS-6) and Social Phobia Scale (SPS-6), both with six items each, and the Brief Fear of Negative Evaluation – Straightforward (BFNE-S), an 8-item measure. The established clinical cutoff is 7 and above for SIAS-6 and 2 for SPS-6.Citation35 A sample item for SIAS-6 is “I have difficulty making eye contact with others” and SPS-6 is “I get nervous that people are staring at me as I walk down the street.” The cutoff for BFNE-S is 25.Citation36 A sample item of the BFNE-S is “When I am talking to someone, I worry about what they may be thinking about me.” Perceived Stress Scale-10 (PSS), a 10-item measure, was included to assess perceived stress. PSS is not a diagnostic tool; no cutoff is available. A sample item for PSS is “In the last month, how often have you felt that things were going your way?” The internal consistency of the measures in the study was good (Cronbach’s alphas = 0.83 to 0.93).
Quality of Life
Two measures of quality of life (QoL) were included. First, the Farage Quality of Life (FQoL™)Citation37 was used to assess i) energy and vitality and ii) well-being. Higher score indicates higher quality. A sample item of the FQoL is “For the most part, over the past seven days, I have felt calm and peaceful.” Second, we included the Dermatology Life Quality Index,Citation38 a 10-item measure of dermatology-specific impact on QoL. The DLQI has established norms:Citation39 0 to 1 indicates that the condition had no effect at all on the participant’s life; 2 to 5 indicates that the condition had a small effect; 6 to 10 indicates moderate effect; 11 to 20 indicates very large effect; 21 to 30 indicates extremely large effect. In this study, the DLQI was adapted to refer to dandruff specifically. A sample item of the DLQI is “Over the past week, how much has your dandruff influenced the choses you wear?” The internal consistency of the two subscales of FQoL and of DLQI in the study was good (Cronbach’s alphas = 0.87 to 0.91).
Sleep Quality was measured using the widely cited Pittsburg Sleep Quality Index (PSQI).Citation40 The cutoff for good vs poor sleep quality is 5; those scoring 5 or below are considered good sleepers. A sample item of the PSQI is “During the past month, how often have you had trouble sleeping because you wake up in the middle of the night or early morning?” The internal consistency of the measures in the study was satisfactory (Cronbach’s alpha = 0.77).
Appearance anxiety was measured using the Appearance Anxiety Inventory (AAI),Citation41 which was developed for the diagnosis of body dysmorphic disorder. It is also used to measure the cognitive and behavioural aspects of body image anxiety in general. The clinical cutoffs of 14 or aboveCitation42 and 20 or aboveCitation43 have been suggested. In this study, we adopted the latter, ie, the more stringent threshold. A sample item for AAI is “I compare aspects of my appearance to others.” The internal consistency of the items in the study was good (Cronbach’s alpha = 0.91).
Dandruff helplessness was measured using an adapted version of the 6-item helplessness subscale of the Illness cognition questionnaire.Citation44 Sample items include “My dandruff frequently makes me feel helpless” and “My dandruff limits me in everything that is important to me.” The internal consistency of the items in the study was good (Cronbach’s alpha = 0.89).
Stigma specially related to dandruff was measured using a modified version of the 6-item stigmatization subscale of the Impact of Chronic Skin Disease on Daily Life scale.Citation45 Sample items include “Other people find me unattractive because of my dandruff” and “Other people think that my dandruff is contagious.” The internal consistency of the items in the study was good (Cronbach’s alpha = 0.88).
Rejection sensitivity refers to the extent to which a person is vigilant to potential cues of rejection or perceiving rejection in social relationships. It was measured using the Adult Rejection Sensitivity Questionnaire (A-RSQ).Citation46 The questionnaire provides the respondents with social scenarios for them to rate their degree of concern and expectancy of rejection. A sample item for A-SRQ is
You approached a close friend to talk after doing or saying something that seriously upset him/her. How concerned or anxious would you be over whether or not your friend would want to talk with you?
The internal consistency of the items in this study was good (Cronbach’s alpha = 0.93).
Comorbidity
A single-item on whether the participant currently suffers from other skin conditions was asked. The included conditions were acne, psoriasis, eczema, vitiligo, alopecia areata, and other (specify). The number of endorsed conditions was summed.
History of Dandruff-Based Teasing & Ostracism
Respondents were asked to report their experience of being teased or ostracized due to dandruff when they were teenagers. They were given six items of experience (eg, being teased/picked on, being avoided by others, being stared at) to respond on a 5-point Likert scale. The internal consistency of the items was good (Cronbach’s alpha = 0.91).
Statistical Analyses
First, we compared the dandruff group with the no-dandruff group on the mental health and psychosocial outcome measures using t-tests. Second, we compared the subgroups of dandruff severity using ANOVA. Whenever appropriate, effect sizes (Cohen’s d) of between-group differences are computed. We also examined the bivariate associations between the severity of dandruff and the outcome measures. Spearman’s r rank correlation coefficient was used when dandruff severity was involved owing to the non-normal distributed (due to purposeful sampling); otherwise, Pearson’s r was reported. Moderation effects were tested by multiple regression estimating the interaction between dandruff severity and the hypothesized moderators: gender, comorbidity, and history of teasing and ostracism. To avoid inflating Type-I error, for the test of moderators, we focused on K6 (psychological distress), DqoL (quality of life), and PSQI (sleep quality) as outcome variables. Finally, we tested the interaction effect between dandruff severity and history of dandruff-based teasing and ostracism on stigma. All the analyses were conducted using JMP and R.
Results
Descriptive and Bivariate Analyses
The average age of our participants was 33 (SD = 10). Most participants (87.2%) have received tertiary education, the remaining completed either high school (3.6%), junior high school (2.4%), or primary school (0.05%). As reported in , 27.2%, 27.3%, 30.1%, and 15.4% of participants were in the severe, moderate, light, and not experiencing dandruff severity categories, respectively. Similarly, 18.7%, 36.0%, 31.2%, and 14.0% of participants reported that they currently have severe, moderate, light, or no dandruff, respectively (). The two measures of dandruff severity were highly correlated (Spearman r = −0.90).
Main Outcomes
The between-group comparisons between those with or without dandruff and different severity of dandruff across the following variables are detailed in and , respectively. The correlations between variables are reported in .
Table 2 Summary Table Comparing Dandruff Vs No Dandruff Groups
Table 3 Summary Table Comparing Dandruff Levels Vs No Dandruff Groups
Table 4 Zero-Order Correlation Between Study Variables
Mental Health Outcomes
On average, those with dandruff were more psychologically distressed than those without, d = 0.48. More than half (54.5%) of those in the severe dandruff category met the cutoff for moderate psychological distress, whereas 39.9% of those with less severe dandruff met the cutoff. K6 scores were associated with both measures of dandruff severity, r = 0.24 to 0.26 ().
Across the three measures of social anxiety, adults with dandruff were more socially anxious than those without, d = 0.51 to 0.80. Most of those in the severe dandruff category met the clinical cutoff for social phobia according to both SIAS (63.5%) and SPS (89.4%). For BFNE-S, those with severe dandruff have an average BFNE-S of 21.1 (SD = 6.9), which is below the cutoff score of 25 that is indicative of clinically significant social anxiety.Citation36 The correlation between dandruff severity and social anxiety measures ranged from r = 0.22 to 0.35 (). Respondents with dandruff perceived more stress than those without, d = 0.54. The association between perceived stress and dandruff severity ranged from r = 0.23 to 0.25.
Quality of Life Outcomes
Adults with dandruff had worse QoL across both subscales of FqoL. The effect sizes of their difference were d = 0.40 and 0.65 for the energy and well-being domains, respectively. Among those with dandruff, the mean DLQI scores with light, moderate, and severe severity were 7.78 (6.16), 9.05 (5.79), and 12.80 (6.28), respectively. The two subscales of the FQoL and the DLQI were correlated with severity of dandruff among adults.
Sleep Outcomes
Participants with dandruff were poorer sleepers than those without, d = 0.95. The correlation between dandruff severity and sleep quality was r = 0.35 to 0.39.
Psychosocial Outcomes
Those suffering from dandruff were more anxious about their appearance than those without dandruff, d = 0.73. More than a quarter of participants (29%) in the severe dandruff category scored beyond the clinical cutoff for appearance anxiety (score ≥ 20). We also found a correlation between dandruff severity and appearance anxiety, ranging from r = 0.33 to 0.36. Participants in the dandruff category had a mean helplessness score of 11.48 (SD = 4.23). Helplessness was associated with dandruff severity with r = 0.21 to 0.27. Those who suffer from dandruff were also more sensitive to rejection, d = 0.32, but the correlation between dandruff severity and rejection sensitivity was small, r = 0.09 to 0.12. Stigma was also associated with dandruff severity, r = 0.20 to 0.26. Respondents who have dandruff also were more likely to have reported history of dandruff-based teasing and ostracism, d = 0.72. There was a small but significant association with dandruff severity, r = 0.14 to 0.24.
Moderation Analysis
Gender
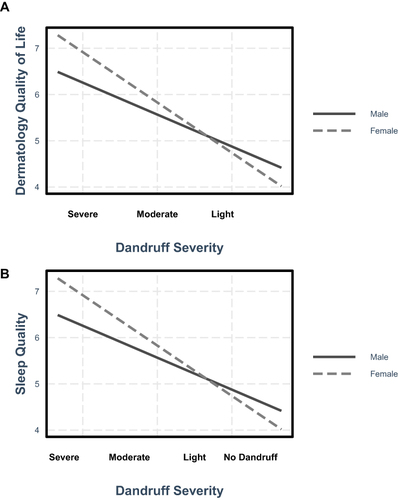
We examined whether the psychological impact of dandruff differed across genders, although no functional differences have been found in dandruff physiology across genders.Citation47 Main effect of gender was found in psychological distress (B = −1.21, SE = 0.23, p < 0.001), quality of life (B = −1.53, SE = 0.29, p < 0.001), and sleep quality (B = −0.26, SE = 0.11, p = 0.016). Women were more distressed and had lower quality of life and sleep quality than men. We also found significant interaction effects between gender and dandruff severity in DqoL (B = 0.37, SE = 0.18, p = 0.037) and sleep quality (B = 0.20, SE = 0.05, p < 0.001) (). Female participants’ quality of life and sleep were more impacted by their dandruff as the severity increases than their male counterparts. No moderating effect of gender was found on psychological distress.
Figure 1 Interaction between dandruff severity and gender on quality of life (A) and sleep quality (B).
Comorbidity
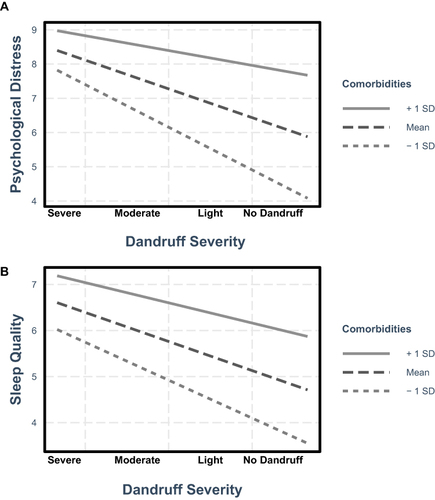
We examined whether suffering from other skin conditions exacerbated the impact of dandruff. We found that comorbidity had a robust main effect; having more skin conditions was associated with worse psychological distress (B = 1.39, SE = 0.16, b = 0.20, p < 0.001) and sleep (B = 1.04, SE = 0.07, b = 0.31, p < 0.001). We also found an interaction effect between dandruff severity and the number of other skin condition one suffers on psychological distress (B = 0.25, SE = 0.07, b = 0.08, p < 0.001) and sleep quality (B = 0.12, SE = 0.03, b = 0.07, p < 0.001) (). This suggests as one has more skin conditions, and the impact of dandruff severity on psychological distress and sleep quality increases. Comorbidity had a main effect on DLQI (B = 2.19, SE = 0.10, b = 0.28, p < 0.001). We did not find an interaction effect on DLQI, however.
Figure 2 Interaction between dandruff severity and comorbidities of other skin conditions on psychological distress (A) and sleep quality (B).
History of Dandruff-Based Teasing and Ostracism
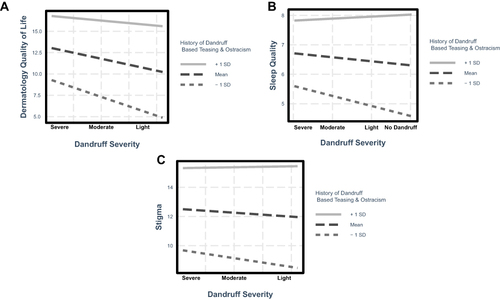
We examined the longer-term impact of dandruff and history of dandruff-based teasing and ostracism. Respondents who were teased for their dandruff as teenagers, regardless of their current dandruff severity, had poorer quality of life (B = 0.84, SE = 0.03, b = 0.67, p < 0.001) and sleep (B = 0.24, SE = 0.02, b = 0.48, p < 0.001), and perceived more stigma (B = 0.59, SE = 0.02, b = 0.77, p < 0.001). Three of the four tested interaction effects were also significant (quality of life: B = 0.08, SE = 0.02, b = 0.10, p < 0.001; sleep: B = 0.02, SE = 0.01, b = 0.07, p < 0.03; stigma: B = 0.03, SE = 0.01, b = 0.07, p < 0.01) (). Simple slope test showed that when history of dandruff-based teasing and ostracism was low (−1SD), worse dandruff severity was associated with worse sleep quality and more perceived stigma but not when history of dandruff-based teasing and ostracism was high (+1SD). When history of dandruff-based teasing and ostracism was high, sleep quality was poor and perceived stigma was high, regardless of dandruff severity. All other simple slope analyses reported above found significant slope at both +1SD and −1SD.
Figure 3 Interaction between dandruff severity and history of dandruff-based teasing and ostracism on dermatology quality of life (A), sleep quality (B), and stigma (C).
Discussion
In this study of a large sample of adults in mainland China, we found that those with dandruff tend to also have worse psychosocial outcomes than their dandruff-free counterparts across all the measures we examined. We also found that the self-perceived severity of dandruff was associated with most of the outcomes of interest, such that more severe dandruff conditions were associated with worse outcomes. Several important factors were identified to explain individual differences. These factors might be potential avenues for intervention that help mitigate the impact of dandruff.
Those with dandruff, especially those suffering from more severe self-perceived levels of dandruff, had lower quality of life, poorer mental health, and poorer sleep. Furthermore, they were also more anxious about their appearance. Generally, the more severe their perceived severity of dandruff, the worse off were people in these factors. Also, those with higher levels of dandruff severity were also feeling more helpless about their condition. They were also more likely to be more sensitive to rejection and have been teased for their dandruff while young.
We found that those who self-perceived to be experiencing more severe dandruff were also more likely to be suffering from higher degrees of dandruff-related stigma, social anxiety, perceived stress, sleep disturbances, and appearance anxiety. In fact, those who self-perceived to have severe dandruff have reached a level of appearance anxiety similar to those with diagnosable body dysmorphic disorder.Citation48 This subgroup also had a mean helplessness score of 12.8 (SD = 3.9), which is similar to patients with Rheumatoid Arthritis (M = 12.7).Citation44
These findings are generally aligned with those found among individuals suffering from other forms of chronic dermatological conditions, such as vitiligo.Citation49 This suggests that while dandruff is common and may be perceived as cosmetic and not medical, the psychological impact should not be underestimated, especially for those who self-perceived as suffering from severe dandruff.
Individual Differences
Beyond estimating the impact of dandruff, we examined factors that might explain between-individual differences in impact. We found that women’s quality of life was more impacted than men’s as their self-perceived dandruff severity increased. Similarly, female’s sleep was also more impacted than that of their male counterparts. This appears to be in line with the psychological literature on gender differences in appearance concerns.Citation50 One possibility is that their dandruff condition led to appearance anxiety, which in turn affected their sleep.Citation51 It should be noted, however, that the slopes of the model predicting quality of life and sleep quality of men were also statistically significant (). This suggests that men were also affected by the severity of their dandruff condition, albeit to a lesser extent than women.
We also saw that having other skin conditions can contribute to worse psychological outcomes. In other words, self-perceived dandruff severity and other skin conditions both contributed to poorer outcomes; dandruff remained an important factor after statistically controlling for comorbidity. The interaction effect between the number of comorbid skin conditions and dandruff severity was also statistically significant, suggesting that those who suffered more forms of skin condition were also more affected by their dandruff, especially in terms of psychological distress and sleep.
Those who were teased or ostracized for their dandruff when they were younger were also more impacted by their dandruff. This suggests that the influence of early social experience related to dandruff might have a longer-term impact. Indeed, there was a significant correlation between history of dandruff-based teasing and ostracism and current levels of rejection sensitivity (r = 0.40). It is likely that those who were teased for their dandruff when they were young became more sensitive to rejection; this is in line with what the literature suggests.Citation52 Our results highlight the importance of reducing teasing or ostracism, in addition to directly helping youth manage their dandruff.
Implications and Recommendations
In the short run, the above findings suggest that, first and foremost, the most direct way to help mitigate the impact of dandruff is to reduce its severity or perceived severity. Women, those suffering from other skin conditions and those who suffered from teasing or ostracism because of their dandruff, might need further support.
In the longer term, public health interventions might entail normalizing dandruff by highlighting its high prevalence and causes. However, when doing so, one should avoid introducing or reinforcing stereotypes. One strategy would be to identify and correcting existing relatively widespread beliefs about the cause of dandruff.
For those who cannot completely ameliorate the dandruff condition, we can focus on helping them to minimize the impact of dandruff. Some recommendations include introducing more adaptive ways of coping, amending erroneous perceptions about the condition, and promoting a healthy lifestyle in general (eg, improving sleep, diet, exercise). Healthy sleep (ie, sufficient amount and quality) might be a good starting point, given the found association between dandruff and poor sleep and the rich literature on the impact of poor sleep on mental health outcomes. Helping people improve their sleep might be a relatively effective and efficient angle in yielding improvement in dandruff and its downstream psychosocial outcomes.
Referencing the literature on other skin conditions, the social consequences of dandruff are the possible reasons why dandruff is a source of distress. In our study, social anxiety, rejection sensitivity, and history of teasing and ostracism were associated with higher levels of psychological distress and lower levels of quality of life. For those who were teased for dandruff, depending on the severity and other trauma-related symptoms, one can consider providing different levels of intervention, including self-help material on how to cope with emotional distress stemming from unpleasant memories, facilitating peer support programs (eg, support groups), and professionally delivered services.
In sum, based on this study and other relevant past studies, the impact of dandruff in part is exacerbated by psychological factors. As such, to reduce the impact, we can consider altering perception, attitude, beliefs, and behaviors, in addition to intervening medically. Culturally appropriate and accepted means would likely be better received and thus have more traction.
Strengths and Limitations
The findings provide a variable contribution to the dandruff literature in particular and the dermatitis literature in general. This study has a relatively large sample size; its purposeful sampling afforded the examination of important bivariate and the moderation analyses. This study also contributes valuable data from a non-WEIRD (ie, non-western, educated, industrialized, rich, democratic) population.Citation53
The study has several methodological shortcomings. First, the cross-sectional design renders the inferences tentative. We cannot draw conclusions about causal relationships.
Second, the questionnaire study relied on self-report. We did not include an objective measure dandruff severity. Participants’ responses may also be affected by recall bias, especially questions concerning earlier experience concerning dandruff and bullying. Third, the sampling strategy prevents us from generalizing our findings to other non-urban, less-affluent regions in China. Future research should consider using a longitudinal design, objective measures of dandruff severity, preferably corroborated by a dermatologist, and including an even more diverse sample.
Conclusion
This large-scale study identified a number of psychological outcomes related to dandruff and dandruff severity among mainland Chinese adults. It also found evidence for several key moderating factors that explain individual differences in outcome. The identified moderators provide valuable insights into how to potentially mitigate the impact of dandruff.
Disclosure
Christian Chan is a paid consultant of P&G Beauty. Tammy Smith, Zemiao He, and Carrie Garter are employees of P&G Beauty. This study was funded by P&G Beauty. The authors report no other conflicts of interest in this work.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due to the ownership of the data belongs to P&G Beauty but may be made available from the corresponding author on reasonable request.
References
- Schwartz JR, Cardin C, Dawson T. Dandruff and seborrheic dermatitis. In: Barran R, Maibach H, editors. Textbook of Cosmetic Dermatology. 3rd ed. New York: Taylor & Francis; 2005:259–272.
- Schwartz JR, DeAngelis YM, Dawson TL. Dandruff and seborrheic dermatitis: a head scratcher. Pract Modern Hair Sci. 2012;1:389–413.
- Schwartz JR, Messenger AG, Tosti A, et al. A comprehensive pathophysiology of dandruff and seborrheic dermatitis–towards a more precise definition of scalp health. Acta dermato venereol. 2013;93(2):131–137. doi:10.2340/00015555-1382
- Caspers AP. Pityriasis capitis (dandruff); a clinical evaluation of three remedies currently employed in the prophylaxis and treatment of a common scalp disorder. Can Med Assoc J. 1958;79(2):113–118.
- Faergemann J. Seborrheic dermatitis (dandruff). Cosmetic Science And Technology Series; 2000:197–202.
- DeAngelis YM, Gemmer CM, Kaczvinsky JR, Kenneally DC, Schwartz JR, Dawson TL. Three etiologic facets of dandruff and seborrheic dermatitis: malassezia fungi, sebaceous lipids, and individual sensitivity. J Invest Dermatol Symp Proc. 2005;10(3):295–297. doi:10.1111/j.1087-0024.2005.10119.x
- Sheth U, Dande P. Pityriasis capitis: causes, pathophysiology, current modalities, and future approach. J Cosmet Dermatol. 2021;20(1):35–47. doi:10.1111/jocd.13488
- Wikramanayake TC, Borda LJ, Miteva M, Paus R. Seborrheic dermatitis—looking beyond Malassezia. Experiment Dermatol. 2019;28(9):991–1001. doi:10.1111/exd.14006
- Evers AWM, Lu Y, Duller P, Van Der Valk PGM, Kraaimaat FW, Van De Kerkhof PCM. Common burden of chronic skin diseases? Contributors to psychological distress in adults with psoriasis and atopic dermatitis. Br J Dermatol. 2005;152(6):1275–1281. doi:10.1111/j.1365-2133.2005.06565.x
- Gupta MA, Gupta AK. Depression and suicidal ideation in dermatology patients with acne, alopecia areata, atopic dermatitis and psoriasis. Br J Dermatol. 1998;139(5):846–850. doi:10.1046/j.1365-2133.1998.02511.x
- Gupta MA, Gupta AK. Psychiatric and psychological co-morbidity in patients with dermatologic disorders: epidemiology and management. Am J Clin Dermatol. 2003;4(12):833–842. doi:10.2165/00128071-200304120-00003
- Kussainova A, Kassym L, Akhmetova A, et al. Vitiligo and anxiety: a systematic review and meta-analysis. PLoS One. 2020;15(11):e0241445. doi:10.1371/journal.pone.0241445
- Silvan M. The psychological aspects of vitiligo. Cutis New York. 2004;73(3):163–167.
- Worrall N, Taylor VM, Ricketts JP, Jones AP. Personal hygiene cues in impression formation. Percept Motor Skills. 1974;38(3_suppl):1269–1270. doi:10.2466/pms.1974.38.3c.1269
- Davern J, O’Donnell AT, Picardo M. Stigma predicts health-related quality of life impairment, psychological distress, and somatic symptoms in acne sufferers. PLoS One. 2018;13(9):e0205009. doi:10.1371/journal.pone.0205009
- Kelly MM, Brault ME, Didie ER. Psychosocial functioning and quality of life in body dysmorphic disorder. Body Dysmorphic Disorder. 2017;139–154(8):253–258.
- Kuck N, Cafitz L, Bürkner PC, Hoppen L, Wilhelm S, Buhlmann U. Body dysmorphic disorder and self-esteem: a meta-analysis. BMC Psychiatry. 2021;21(1):310. doi:10.1186/s12888-021-03185-3
- Borda LJ, Wikramanayake TC. Seborrheic dermatitis and dandruff: a comprehensive review. J Clin Invest Dermatol. 2015;3(2). doi:10.13188/2373-1044.1000019
- Godbehere A, McDonald L, Baines F, Sutherland CAM, Andrews TJ. A dissociation in judgements of confidence in people with dandruff based on self-reports compared to reports from other observers. Int J Cosmet Sci. 2017;39(4):457–464. doi:10.1111/ics.12400
- Schriber RA, Guyer AE. Adolescent neurobiological susceptibility to social context. Development Cogn Neurosci. 2016;19:1–18. doi:10.1016/j.dcn.2015.12.009
- Pärna E, Aluoja A, Kingo K. Quality of life and emotional state in chronic skin disease. Acta dermato venereol. 2015;95(3):312–316. doi:10.2340/00015555-1920
- Irwin MR. Why sleep is important for health: a psychoneuroimmunology perspective. Annual Review of Psychology. 2015;66(1):143–172. doi:10.1146/annurev-psych-010213-115205
- Irwin MR. Sleep and inflammation: partners in sickness and in health. Nat Rev Immunol. 2019;19(11):702–715. doi:10.1038/s41577-019-0190-z
- Goldstein AN, Walker MP. The role of sleep in emotional brain function. Ann Rev Clin Psychol. 2014;10(1):679–708. doi:10.1146/annurev-clinpsy-032813-153716
- Hoevenaar-Blom MP, Spijkerman AM, Kromhout D, van den Berg JF, Verschuren WM. Sleep duration and sleep quality in relation to 12-year cardiovascular disease incidence: the MORGEN study. Sleep. 2011;34(11):1487–1492. doi:10.5665/sleep.1382
- Pigeon WR, Bishop TM, Krueger KM. Insomnia as a precipitating factor in new onset mental illness: a systematic review of recent findings. Current Psychiatry Reports. 2017;19(8):1–11. doi:10.1007/s11920-017-0802-x
- Wong MM, Brower KJ, Zucker RA. Childhood sleep problems, early onset of substance use and behavioral problems in adolescence. Sleep Med. 2009;10(7):787–796. doi:10.1016/j.sleep.2008.06.015
- Franzen PL, Buysse DJ. Sleep disturbances and depression: risk relationships for subsequent depression and therapeutic implications. Dialog Clin Neurosci. 2022;2:1.
- Smagula SF, Stone KL, Fabio A, Cauley JA. Risk factors for sleep disturbances in older adults: evidence from prospective studies. Sleep Med Rev. 2016;25:21–30. doi:10.1016/j.smrv.2015.01.003
- Chang YS, Chiang BL. Sleep disorders and atopic dermatitis: a 2-way street? J Allergy Clin Immunol. 2018;142(4):1033–1040. doi:10.1016/j.jaci.2018.08.005
- Gupta MA, Gupta AK, Knapp K. Dissatisfaction with cutaneous body image is directly correlated with insomnia severity: a prospective study in a non-clinical sample. J Dermatological Treat. 2015;26(2):193–197. doi:10.3109/09546634.2014.883060
- Jeon C, Yan D, Nakamura M, et al. Frequency and management of sleep disturbance in adults with atopic dermatitis: a systematic review. Dermatol Ther. 2017;7(3):349–364. doi:10.1007/s13555-017-0192-3
- Turlier V, Viode C, Durbise E, et al. Clinical and biochemical assessment of maintenance treatment in chronic recurrent seborrheic dermatitis: randomized controlled study. Dermatol Ther. 2014;4(1):43–59. doi:10.1007/s13555-014-0047-0
- Kessler RC, Andrews G, Colpe LJ, et al. 2022 Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychological Medicine. 2002;32(6):959–976. doi:10.1017/S0033291702006074
- Peters L, Sunderland M, Andrews G, Rapee RM, Mattick RP. Development of a short form Social Interaction Anxiety (SIAS) and Social Phobia Scale (SPS) using nonparametric item response theory: the SIAS-6 and the SPS-6. Psychological Assessment. 2012;24(1):66–76. doi:10.1037/a0024544
- Carleton RN, Collimore KC, McCabe RE, Antony MM. Addressing revisions to the brief fear of negative evaluation scale: measuring fear of negative evaluation across anxiety and mood disorders. J Anxiety Disorders. 2011;25(6):822–828. doi:10.1016/j.janxdis.2011.04.002
- Farage MA, Nusair TL, Hanseman D, Sherman SN, Tsevat J. The Farage quality of life measure for consumer products: development and initial implementation. Appl Res Qual Life. 2010;5(1):1–25. doi:10.1007/s11482-009-9087-5
- Finlay AY, Khan G. Dermatology Life Quality Index (DLQI)—a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210–216. doi:10.1111/j.1365-2230.1994.tb01167.x
- Basra MK, Fenech R, Gatt RM, Salek MS, Finlay AY. The dermatology life quality index 1994–2007: a comprehensive review of validation data and clinical results. Br J Dermatol. 2008;159(5):997–1035. doi:10.1111/j.1365-2133.2008.08832.x
- Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
- Veale D, Eshkevari E, Kanakam N, Ellison N, Costa A, Werner T. The Appearance Anxiety Inventory: validation of a process measure in the treatment of body dysmorphic disorder. Behav Cogn Psychother. 2014;42(5):605–616. doi:10.1017/S1352465813000556
- Mastro S, Zimmer-Gembeck MJ, Webb HJ, Farrell L, Waters A. Young adolescents’ appearance anxiety and body dysmorphic symptoms: social problems, self-perceptions and comorbidities. J Obsessive Compuls Relat Disord. 2016;8:50–55. doi:10.1016/j.jocrd.2015.12.001
- Flygare O, Andersson E, Ringberg H, et al. Adapted cognitive behavior therapy for obsessive-compulsive disorder with co-occurring autism spectrum disorder: a clinical effectiveness study. Autism. 2020;24(1):190–199. doi:10.1177/1362361319856974
- Evers AW, Kraaimaat FW, van Lankveld W, Jongen PJ, Jacobs JW, Bijlsma JW. Beyond unfavorable thinking: the illness cognition questionnaire for chronic diseases. Journal of Consulting and Clinical Psychology. 2001;69(6):1026. doi:10.1037/0022-006X.69.6.1026
- Evers AW, Duller P, van de Kerkhof PC, et al. The Impact of Chronic Skin Disease on Daily Life (ISDL): a generic and dermatology-specific health instrument. Br J Dermatol. 2008;158(1):101–108. doi:10.1111/j.1365-2133.2007.08296.x
- Berenson KR, Gyurak A, Ayduk O, et al. Rejection sensitivity and disruption of attention by social threat cues. J Res Personality. 2009;43:1064–1072. doi:10.1016/j.jrp.2009.07.007
- Bacon RA, Mizoguchi H, Schwartz JR. Assessing therapeutic effectiveness of scalp treatments for dandruff and seborrheic dermatitis, part 2: the impact of gender and ethnicity on efficacy. J DermatolTreat. 2014;25(3):237–240. doi:10.3109/09546634.2012.719077
- Phillips KA, Menard W, Fay C, Pagano ME. Psychosocial functioning and quality of life in body dysmorphic disorder. Comprehensive Psychiatry. 2005;46(4):254–260. doi:10.1016/j.comppsych.2004.10.004
- Henning SW, Jaishankar D, Barse LW, et al. The relationship between stress and vitiligo: evaluating perceived stress and electronic medical record data. PLoS One. 2020;15(1):e0227909. doi:10.1371/journal.pone.0227909
- Quittkat HL, Hartmann AS, Düsing R, Buhlmann U, Vocks S. Body dissatisfaction, importance of appearance, and body appreciation in men and women over the lifespan. Frontiers in Psychiatry. 2019;10:864. doi:10.3389/fpsyt.2019.00864
- Rosenbaum DL, Gillen MM, Bloomer SA. The effects of sleep on body image: examining the roles of depression, perceived stress, and anxiety. J Am College Health. 2023;1–9. doi:10.1080/07448481.2023.2186153
- Gao S, Assink M, Cipriani A, Lin K. Associations between rejection sensitivity and mental health outcomes: a meta-analytic review. Clin Psychol Rev. 2017;57:59–74. doi:10.1016/j.cpr.2017.08.007
- Henrich J, Heine SJ, Norenzayan A. The weirdest people in the world? Behav Brain Sci. 2010;33(2–3):61–83. doi:10.1017/S0140525X0999152X