
Abstract
Background
The aim of this study was to analyze the clinical characteristics of patients with adverse cutaneous drug reactions, which occur when a medicinal product results in cutaneous morbidity.
Methods
The study included 308 patients who were diagnosed as having an adverse cutaneous drug reaction during the study period (2007–2009). In 84 cases, histopathologic examination of skin biopsies were also performed.
Results
Patients with drug reactions were found to be more commonly female (63%) than male (37%). Beta-lactam antibiotics were found to be the most frequent cause of adverse cutaneous drug reactions (42.7%), followed by non-steroidal anti-inflammatory drugs (16.5%). Acute urticaria was the most common clinical presentation (59.2%) followed by fixed drug eruptions (18.5%), and maculopapular eruptions (14.9%).
Conclusion
Adverse cutaneous drug reactions in our study population were mainly induced by beta-lactam antibiotics and non-steroidal anti-inflammatory drugs. The most common forms of cutaneous adverse drug reactions were found to be acute urticaria, fixed drug eruptions, and maculopapular rashes.
Introduction
Adverse drug reactions (ADRs) are undesirable and typically unanticipated reactions independent of the intended therapeutic purpose of a medication,Citation1 that may result in significant morbidity and even mortality. Cutaneous reactions are the most common form of ADRs,Citation2 occurring in 2%–3% of inpatient and in approximately 2% of outpatient patients referred for dermatologic evaluation; approximately 2% of ADRs are considered severe or fatal.Citation3,Citation4 Drug reactions are more common in women, and increase with age and the number of medications used.Citation5
ADRs may be either immunologic (ie, drug allergy) or non-immunologic (ie, drug intolerance), with drug allergies estimated to account for 6%–10% of all ADRs, and drug intolerance accounting for the remaining 90%–94%.Citation6 Cutaneous ADRs produce a wide range of clinical manifestations such as pruritus, maculopapular eruptions, urticaria, angioedema, phototoxic and photo allergic reactions, fixed drug reactions, erythema multiforme, vesiculobullous reactions (eg, Stevens–Johnson syndrome and toxic epidermal necrolysis), exfoliative dermatitis, acute generalized exanthematous pustulosis, and serum sickness.Citation7,Citation8 Whereas maculopapular rashes and urticaria are among the most common cutaneous drug reactions,Citation9 anaphylaxis, Stevens–Johnson syndrome, and toxic epidermal necrolysis may result in mortality.Citation10
The purpose of this study was to examine the clinical characteristics and purported etiologic agents for ADRs in our patient population.
Materials and methods
A descriptive, prospective case-series study was performed during 2007–2009. Three hundred and eight consecutive inpatient and outpatient subjects with a diagnosis of ADR referred to the dermatology service of Sina hospital in Hamadan, Iran were enrolled in the study. All patients suspected of having an ADR were clinically evaluated by an attending dermatologist. In 84 cases, histopathological examination of skin biopsies were obtained, in many cases to distinguish between specific types of drug reaction, eg, DRESS syndrome versus exanthematous eruptions. The presence of eosinophils in dermal inflammatory infiltrates was considered to support a hypersensitivity reaction.
Each patient was informed of the nature of the study and signed a consent form approved by the Research Council and Ethics Committee of Hamedan University of Medical Sciences, Hamedan, Iran. Written informed consent was obtained from patients for publication of this study and for any accompanying images. The study was performed in accordance with the ethical guidelines of the 1975 Declaration of Helsinki.
Exclusion criteria in this study included: 1) a history of taking more than one drug class likely to cause the adverse reaction; 2) clinical manifestations that were not compatible with drug reactions; 3) patient inability to produce the medication consumed the last 3 weeks that purportedly caused the reaction (to prevent recall bias); 4) cases involving overlapping diagnoses with other conditions; and 5) cases in which the clinical diagnosis did not match the findings cited in the pathology report.
Results
During the study period, 308 patients, including 114 men (37%) and 194 women (63%), were enrolled. Of the 308 patients, the diagnosis of ADR was made based on purely clinical manifestations in 224 cases; histological confirmation was obtained in 84 cases. The mean age of patients was 35.2±16.8 years (range 2–77 years). In the present study, ADRs were more frequently seen in the third and fourth decades of life, with 40% of reactions seen in this age group. The clinical manifestations of cutaneous ADRs are summarized in and examples are provided in and . Only 20 of the 308 patients (6.5%) in our study reported a history of a previous drug reactions.
Figure 1 A 25-year-old woman with the diagnosis of acute generalized exanthematous pustulosis following the use of cephalexin.

Figure 2 A 37-year-old woman with clinical manifestation of DRESS syndrome due to phenytoin.

Table 1 Clinical manifestations of cutaneous adverse drug reactions
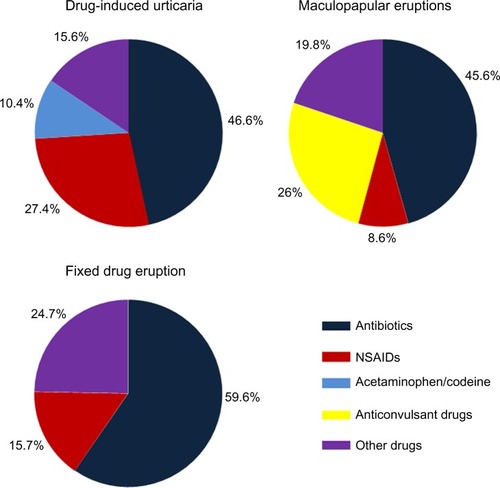
In patients with urticarial drug eruptions, 76 (46.6%) were attributed to antibiotics, 45 (27.4%) to non-steroidal anti-inflammatory drugs (NSAIDs), and 17 (10.4%) to codeine with acetaminophen. In patients with maculopapular eruptions, 21 (45.6%) were attributed to antibiotic use, 12 (26%) to anticonvulsant drugs, and four (8.6%) to NSAIDs. In the beta-lactam and NSAID subgroups, amoxicillin and ibuprofen were the most common offending agents, respectively. In patients with fixed drug eruptions, 34 (59.6%) were attributed to taking trimethoprim-sulfamethoxazole and nine (15.7%) to taking NSAIDs ().
Figure 3 Causative agents for the three most common types of cutaneous drug reactions: urticaria, fixed drug eruptions, and maculopapular eruptions.
In patients with a diagnosis of fixed drug eruption induced by trimethoprim-sulfamethoxazole (34 patients), most lesions were present in the genital area (18 patients). Five patients had lesions in both the genital area and the lip, and only one patient suffered from a lesion present only on the lip. The remaining patients had lesions in other areas, including the hands and feet. In the group taking NSAIDs (nine patients), one patient had a fixed drug eruption on the lip, one patient had it on the genital area, and two patients had lesions on both the lip and genital area. The remaining five patients had lesions on other body areas, including the hands, feet, and trunk.
Among the seven patients with erythema multiforme, two had history of taking trimethoprim-sulfamethoxazole. In this study, only one patient had a diagnosis of DRESS syndrome, which was attributed to phenytoin.
In this study, the most common cutaneous clinical manifestations of ADRs in the order of frequency were urticaria, maculopapular eruptions, and fixed drug reactions (). Antibiotics (42.7%) and NSAIDs (16.5%) were the most common causes of drug reactions in our study population.
Discussion
Consistent with the results of previous studies, we found that adverse cutaneous drug reactions are more common in women than in men.Citation11 In the present study, 40% of drug reactions were seen in third and fourth decades of life, which is consistent with the findings of Sushma et al in their 2005 study.Citation8
In the study performed by Souissi et al in 2007, the most common cutaneous clinical manifestations were maculopapular eruptions followed by fixed drug eruptions, and antibiotics and NSAIDs were the most commonly purported agents.Citation12 Fiszenson-Albala et al, in a study of drug reactions in the French population, reported maculopapular eruptions followed by urticaria and erythroderma to be the most frequent ADRs in their population.Citation13 Kacalak-Rzepka et al reported maculopapular eruptions and urticaria as the most common forms of ADR.Citation11 The high prevalence of urticaria in our study may be due to the excessive use of beta-lactam antibiotics for the treatment of upper respiratory viral infections, often without proper medical indication.
In patients with a diagnosis of fixed drug eruption induced by trimethoprim-sulfamethoxazole, most lesions were seen in the genital area, whereas in the group taking NSAIDs, most lesions were seen on the hands and feet. In comparison, Justiniano et al reported that fixed drug eruptions induced by trimethoprim-sulfamethoxazole were most commonly present on the genital area, while those induced by NSAIDs were most commonly seen on the lip.Citation14
It should be noted that our study does not address the mechanism of ADRs, and many drug reactions may not result from allergic or non-allergic drug hypersensitivity. In addition, a drug reaction cannot be confirmed without further testing, such as rechallenge, which was not performed in our study. Moreover, histologic examination may not reveal changes specific to a drug eruption, although biopsies may be helpful in distinguishing particular subtypes of reactions. Furthermore, a more helpful study may compare the adverse event rate to exposure rate by gathering local data on dispensing of various etiologic agents to estimate the cutaneous adverse event rate.
Conclusion
According to our results, adverse cutaneous drug reactions were mainly induced by beta-lactam antibiotics and NSAIDs. The most common forms of cutaneous ADRs in order of frequency were acute urticaria, fixed drug eruptions, and maculopapular rashes. In our study, the most common form of cutaneous ADR was found to be urticaria, while some studies conducted in other parts of the world have found maculopapular eruptions to be more common. The high consumption of beta-lactam antibiotics in the treatment of common viral upper respiratory infections in our area may contribute to our findings.
Disclosure
The authors have no conflicts of interest to declare.
References
- HunzickerTKaziaPBraunschweigSComprehensive hospital drug monitoring (CHDM): Adverse skin reaction a 20 year surveyAllergy19975243883939188919
- Jean RevuZAllanoreLVDrug ReactionBologniaJean LJorizzoJoseph LJulieDermatology3rd edElsevier2012335
- Charli-JosephYCruz-FuentesCOrozco-TopeteRIncidence of adverse cutaneous drug reaction in Mexican sample: an exploratory study on their association to tumour necrosis factor alpha TNF2 alleleJ Eur Acad Dermatol Venereol200923778879219309429
- WolfROrionEMarcosBMatzHLife-threatening acute adverse cutaneous drug reactionsClin Dermatol200523217118115802211
- PichlerWJYawalkarNBritschgiMCellular and molecular pathophysiology of cutaneous drug reactionAm J Clin Dermatol200234299238
- HamiltonRGAdkinsonNFJrClinical laboratory assessment of IgE-dependent hypersensitivityJ Allergy Clin Immunol20031112 SupplS687S70112592314
- Kimyai-AsadiAHarrisJCNousariHCCritical overview: adverse cutaneous reactions to psychotropic medicationsJ Clin Psychiatry1999601071472510549695
- SushmaMNoelMVRitikaMCJamesJGuidoSCutaneous adverse cutaneous drug: a 9 year study from a South Indian HospitalPharmacoepidemiology Drug Saf2005148567570
- RevuzJValeyrie-AllanoreLDrug reactionsBologniaJLLorizzoJLRapiniRPDermatology2nd edSpainMosby-Elsevier2008301320
- RoujeanJCEpidemiology of drug reaction, service de dermatologie, Universite Paris200413322328
- Kacalak-RzepkaAKlimowiczABielecka-GrzelaSZaługaEMaleszkaRFabiańczykHRetrospective analysis of adverse cutaneous drug reactions in patientsAnn Acad Med Stetin2008542525819374232
- SouissiAFennicheSBenmouslyRBenJSMarrakHMokhtarIStudy of the cutaneous drugs reactions in a teaching hospital in TunisTunis Med200785121011101519170378
- Fiszenson-AlbalaFAuzerieVMaheEA 6 month prospective survey of cutaneous drug reactionBr J Dermatol200314951018102214632808
- JustinianoHBerlingeri-RamosACSanchezJLPattern analysis of drug-induced skin diseaseAm J Dermatopathol200830435236918645307