
Abstract
Background
This ex vivo study aimed to compare transportation of the mesiobuccal root canal of mandibular first molars instrumented with ProTaper, Race and Sendoline rotary systems using cone beam computed tomography (CBCT).
Materials and methods
Forty-five mesiobuccal canals of mandibular first molars were randomly divided into three groups of 15. Root canals in each group were instrumented with the ProTaper, Race or Sendoline rotary system according to the manufacturers’ instructions. Root canal preparations were performed by one operator, while root canal wall measurements were made by another operator blinded to the group allocation of teeth. The pre- and post-chemomechanical preparation CBCT scans were obtained and evaluated at 3, 6 and 9 mm levels from the apex. The amount of root canal transportation at these levels was calculated. Data were analyzed using SPSS version 17 via Mann–Whitney and Kruskal–Wallis tests. P<0.05 was considered significant.
Results
No significant difference was noted in canal transportation among the groups (P>0.05), but ProTaper showed the least and Sendoline caused the most canal transportation in the coronal third.
Conclusion
ProTaper, Race and Sendoline rotary systems are not significantly different in terms of canal transportation. Although all rotary files cause root canal transportation, ProTaper and Race showed the least amount of canal transportation in the coronal and apical thirds, respectively.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Endodontic treatment is performed to clean and shape the root canal system and efficiently fill the root canal in a three-dimensional (3D) fashion. According to Schilder, root canal preparation should flare the root canal from apical to coronal third and maintain the apical foramen without changing the original curvature of the root canal path.Citation1 A successful endodontic treatment is hard to perform in some teeth due to complexities of the root canal anatomy and degree or radius of the root canal curvature.Citation2,Citation3 Canal transportation occurs as the result of tendency of the files to straighten up and return to their original straight shape. Canal transportation is defined as the removal of dentin from the external wall of the curvature in the apical half and internal wall of the curvature in the coronal half of the root canal, which negatively affects long-term prognosis of root canal treatment.Citation3
The introduction of nickel titanium (NiTi) files with high flexibility has resulted in safer preparation of curved canals and has decreased the incidence of iatrogenic procedural errors such as canal transportation.
ProTaper system is extensively used for root canal preparation. Due to their unique design, ProTaper files are suitable for the preparation of curved and calcified canals.Citation4 The amount of root canal transportation by this system is less than that observed using M-Two, and thus, ProTaper can be easily and safely used in the clinical setting.Citation5 Canal straightening using ProTaper was compared with Reciproc, and it was found that single-file systems can well shape the curved canals, are cost effective and decrease procedural errors and complications such as instrument fracture.Citation6 One-Shape and WaveOne have shown less canal transportation and higher canal-centering ability than ProTaper.Citation7 The canal-centering ability of the Revo-S system is higher than that of ProTaper, and the amount of canal transportation caused by ProTaper is higher than that by Revo-S. However, in general, differences among Revo-S, One-Shape and ProTaper are not significant for the instrumentation of curved canals.Citation8 The canal-centering ability of ProTaper and Profile Vortex systems is not significantly different either, and both systems cause transportation of the apical foramen.Citation9 Another study found no significant difference in the transportation of curved canals following instrumentation with Hero Shaper, ProTaper, Twisted File and Liberator.Citation10
The Race rotary system has been previously studied, and its optimal efficacy for cleaning and shaping of root canals with a high centering ability has been confirmed.Citation11 Final apical preparation by BioRace is more efficacious and practical as it has a fewer number of files compared to Race.Citation12 Files in this system have a triangular cross section and alternating cutting edges.Citation13
Sendoline S5 (Sendoline, Taby, Sweden) is a new NiTi rotary system made of the conventional NiTi alloy. It has a unique S-shaped cross section and progressive flutes along its length. This design enhances the extrusion of debris and decreases the risk of fracture. Sendoline S5 instruments include five files of S1 (0.08/30), S2 (0.06/30), S3 (0.04/30), S4 (0.04/25) and S5 (0.04/20).Citation14
It has been shown that ProTaper Universal and WaveOne NiTi files with a high taper cause greater canal transportation than Sendoline S5 and GTX files with a lower taper.Citation15
Noninvasive techniques such as cone beam computed tomography (CBCT), which shows 3D cross-sectional views of the root, are advantageous for the assessment of root canal anatomy and comparison of the canal shape before and after preparation.Citation16,Citation17 For this purpose, CBCT is more valuable than conventional techniques as it does not damage the samples and also allows for the measurement of the amount of root dentin removed by endodontic instrumentation.Citation18 Currently, CBCT images are commonly used for diagnostic purposes.Citation19,Citation20 Therefore, this ex vivo study aimed to compare the transportation of the mesiobuccal canal of mandibular first molars prepared with three NiTi rotary systems, namely, ProTaper, Race and Sendoline S5, using CBCT.
Materials and methods
A total of 45 mandibular first molars with closed apices and a mean root curvature of 20–40° at a 5–9 mm distance from the apex measured by the Schneider’s methodCitation21 were chosen. The teeth had a mean length of 19–22 mm. The teeth had been extracted for periodontal or orthodontic reasons at the Oral and Maxillofacial Department of Zahedan University of Medical Sciences, School of Dentistry. Written informed consent was obtained from all patients. The study protocol was approved by the ethics committee of this university (IR. ZAUMS.REC.1395.9).
Tissue residues and calcified debris were eliminated by scaling, and the teeth were immersed in a 0.1% thymol solution at 9°C for 24 hours. The teeth were then rinsed under running water to eliminate thymol residues and stored in saline at 4°C until the experiment. Primary radiographs were obtained to assess the apex of the mesial root and determine the degree of root curvature. Teeth with mesial canals with an independent apical foramen and no sign of calcification or internal resorption were chosen. Teeth with S- or C-shaped canals were excluded. All roots were inspected under a stereomicroscope at ×12 magnification to ensure absence of craze lines, cracks or fractures. Teeth with such defects were excluded and replaced with sound teeth.
The access cavity was prepared using a diamond bur with a high-speed hand piece under water and air spray to reveal the mesiobuccal canal orifice. A #10 K file (MANI Inc., Utsunomiya, Japan) was used for the working length determination. The file was introduced into the canal until its tip was visible at the apex. Working length was determined 1 mm short of this length. The root was covered with a silicon impression material (Oranwash; Zhermack SpA, Badia Polesine (RO), Italy) to simulate the periodontal ligament. The apical foramen was sealed with red dental wax to prevent the entry of the silicon impression material into the apical foramen. The teeth were then mounted in blocks made of polyvinyl siloxane putty wash (Speedex; Coltène/Whaledent AG, Altstätten, Switzerland) measuring 5×5 cm2 to the level of their cementoenamel junction in a parallel fashion to standardize before and after instrumentation radiographs. A small piece of an orthodontic wire was placed at the corner of silicon blocks to determine the direction of scanning. The teeth were randomly divided into three groups (n=15), and ProTaper, Race and Sendoline rotary systems were used for root canal preparation in Groups 1–3, respectively.
Root canal preparation
All root canals were prepared using the crown-down technique by a hand piece (X-Smart; Dentsply Maillefer, Ballaigues, Switzerland) with controlled speed and torque recommended by the manufacturer for each system along with rinsing with 2.5% sodium hypochlorite with a 30-gauge needle between instruments. Also, 17% EDTA and 5.25% sodium hypochlorite were used for the final rinse to eliminate the smear layer.
The ProTaper universal rotary system
In the ProTaper group (Dentsply Maillefer), first the SX file and then S1 and S2 files were used with 300 rpm and 3 N·cm torque for flaring of the orifice, and coronal and middle thirds of the mesiobuccal canal to obtain a straight-line access. Then, for the preparation of glide path, #15 K file was used to the working length. Root canal preparation was continued by F1, F2 and F3 files to the working length. Each file was discarded after use in three canals.
The Race rotary system
The preparation of mesiobuccal root canals was started with 0.01/40 NiTi files of Race at 600 rpm with 2 N·cm torque according to the manufacturer’s instructions and followed by the use of 0.08/35, 0.06/25, 0.04/25 files if required. Canals were finally prepared with 0.04/25, 0.06/25, 0.06/30 files to the working length.
The Sendoline rotary system
The mesiobuccal canal in this group was prepared with Sendoline S5 rotary files at 300 rpm and 2 N·cm torque according to the manufacturer’s instructions as follows: first, the 0.08/30 files was used to flare the coronal and middle thirds to obtain a straight-line access, and then 0.06/30 files was used to access two-thirds of the root canal and continued by the 0.04/30 files to reach the apical third; the 0.04/25 files was used to the working length, and the apical region was instrumented with 0.04/20, 0.04/25 and 0.04/20 files; and the 0.06/30 files was eventually used for apical widening.
CBCT
The CBCT scans were obtained of the root canals before and after preparation using dental X-ray unit (Vatech Co., Hwaseong, South Korea) with exposure settings of 5.4 mA, 89 kVp and 17 s. The thickness of instrumented and non-instrumented canal walls was measured at 3, 6 and 9 mm from the apex. Canal transportation, denoted as CT, was calculated using the following formula: CT=(A1−A2)−(B1−B2),Citation22 where A1 is the shortest distance from the mesial root surface to the mesial margin of the nonprepared canal; A2 is the shortest distance from the mesial root surface to the mesial margin of the prepared canal; B1 is the shortest distance from the distal root surface to the distal margin of the nonprepared canal; and B2 is the shortest distance from the distal root surface to the distal margin of the prepared canal.
A value of 0 indicates no transportation, while negative values indicate transportation toward the distal side (furcation side) and positive values indicate transportation toward the mesial side.
It should be noted that preparation of all canals was performed by the same operator, while measurements were made by another operator blinded to the group allocation of teeth.
Data were statistically analyzed using SPSS version 17 (SPSS Inc., Chicago, IL, USA) via the Mann–Whitney and Kruskal–Wallis tests. P≤0.05 was considered statistically significant.
Results
and show the mean and standard deviations of root canal transportation in millimeters at different levels from the apex in the three groups. Although no significant difference was noted among the three groups at different levels in terms of canal transportation (P>0.05), ProTaper caused slightly higher transportation in the apical third and Protaper showed the least and Sendoline caused the most canal transportation in the coronal third.
Figure 1 Mean and standard deviations of canal transportation (in millimeters) in the three groups at different levels from the apex.
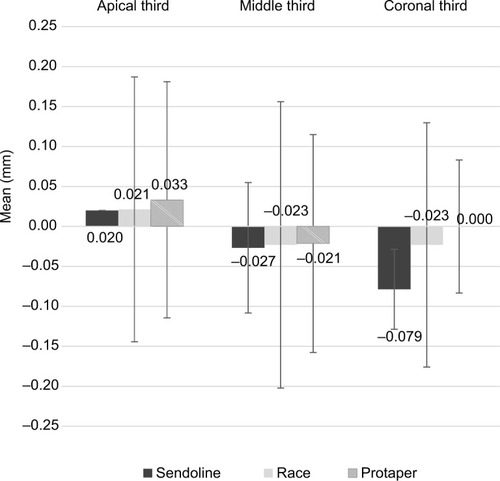
Table 1 Mean and standard deviations of canal transportation (in millimeters) in the three groups at different levels from the apex (n=15)
Discussion
Root canal transportation in some areas such as the apical third compromises root canal obturation. Also, the excess elimination of dentin from the internal wall of the curve in the coronal third weakens the root canal wall and may result in strip perforation and micro-cracks, which must be prevented.Citation23,Citation24
Canal transportation is a procedural error, which decreases the efficacy of the preparation technique and results in incomplete cleaning of the root canal. It also compromises the apical seal.Citation2,Citation23 Wu et al reported that apical transportation of >0.3 mm negatively affects the sealing ability of filling materials.Citation23
Our results showed no significant difference among the groups in terms of canal transportation (P>0.05). But ProTa-per caused slightly higher transportation in the apical third. This finding is probably attributed to the use of the F3 file (0.09/30) in the apical third because we flared the apical region to size 30 in all groups. Stavileci et al also prepared the apical third to F3 using the ProTaper rotary system.Citation25 Increased tapering of the file even with the same size can increase canal transportation. This was clearly noted in Race and Sendoline S5 systems as file #30 with 6% taper was used and caused the same amount of canal transportation, which was less than that of ProTaper. This finding was in agreement with the results of previous studies, which showed no significant difference among rotary systems in canal transportation.Citation26–Citation29 However, our findings in this respect were different from those of Jain et al.Citation30 They showed that ProTaper caused significantly higher canal transportation in the apical and middle thirds, while in the coronal third, this system was not significantly different from other rotary systems. This finding may be due to the progressive tapering of this file along its cutting blade, decreased flexibility and tendency to straighten the curved canals.Citation31 Similar results were obtained by Versiani et al, and they confirmed that optimal centering ability and minimal transportation are achieved by apical preparation up to size 30.Citation31 These results were in accord with ours. However, Pagliosa et al demonstrated that apical preparation with the F2 file of the ProTaper system causes canal transportation toward the internal wall of the curve,Citation10 whereas in our study, the same amount of transportation occurred in the outer wall of the curve, which is probably due to the use of the F3 file to the working length. This finding is in line with the definition of the American Association of Endodontists regarding root canal transportation. They defined root canal transportation as the removal of the root canal structure from the external wall of the curve in the apical half, which results in the accumulation of debris in this area. In general, our results revealed that the ProTaper system caused root canal transportation in the apical region, which was in accordance with the results of Kunert et alCitation32 in 2010 and Javaheri and JavaheriCitation4 in 2007.
Our results showed that ProTaper, Sendoline S5 and Race at 6 mm from the apex removed more dentin from the internal wall of the canal and caused canal transportation toward the internal wall of the curve. It appears that full rotation along with the in and out movement of rotary files without any other intervention (anti-curvature movement) eliminates dentin from the internal wall of the curve due to high tapering of these instruments and makes this wall susceptible to strip perforation and micro-cracks. Therefore, anticurvature movement of the rotary files in curved canals is suggested.
Our results indicated that at 9 mm from the apex, ProTaper removed dentin in equal amounts from the two canal walls but Sendoline S5 removed more dentin from the internal wall of the curve and caused canal transportation toward the furcation area, although this difference was not significant (P>0.05). This finding may be due to the difference in the cross section of this file and that of ProTaper, which results in the removal of higher mounts of dentin from the internal wall of the root canal. It has been reported that Sendoline S5 and Reciproc cause less transportation at the canal orifice than Twisted File, which has been attributed to the S-shaped cross section of Sendoline S5 files.Citation14 Our results revealed that Race at this level removed more dentin from the internal wall of the curve and caused canal transportation toward the furcation. This result was in agreement with that of Ozgur et al.Citation33 They reported that Race showed the highest amount of transportation in the coronal third, which was significantly higher than that caused by ProTaper and Hero Shaper.Citation33 Also, Al-Sudani and Al-Shahrani indicated that Race caused significantly higher transportation than Profile and K3; Profile was superior to other systems in terms of all measured variables.Citation34
Despite all the attempts to simplify biomechanical root canal preparation techniques, the effect of rotary instruments on root canal shape must be taken into account. A complete root canal preparation with minimal canal transportation can be expected with the use of high-taper files in the cervical and middle thirds and low-taper files in the apical third of root canals.
Conclusion
All rotary files cause a small amount of canal transportation. Sendoline S5 caused the highest amount of transportation in the coronal third, while ProTaper caused the least amount of transportation in the coronal and middle thirds and the highest amount of transportation in the apical third.
Acknowledgments
The authors would like to thank the Research Deputy of Zahedan University of Medical Sciences for financially supporting this study and also the Zahedan Medical Imaging Center for providing the CBCT scans. This manuscript was derived from a thesis for a DDS, MS degree.
Disclosure
The authors report no conflicts of interest in this work.
References
- SchilderHCleaning and shaping the root canalDent Clin North Am1974182692964522570
- PetersOACurrent challenges and concepts in the preparation of root canal systems: a reviewJ Endod200430855956715273636
- MooreJFitz-WalterPParashosPA micro-computed tomographic evaluation of apical root canal preparation using three instrumentation techniquesInt Endod J200942121057106419912375
- JavaheriHHJavaheriGHA comparison of three Ni-Ti rotary instruments in apical transportationJ Endod200733328428617320715
- YangGYuanGYunXZhouXLiuBWuHEffects of two nickel-titanium instrument systems, Mtwo versus ProTaper universal, on root canal geometry assessed by micro-computed tomographyJ Endod201137101412141621924193
- Barbosa-RibeiroMAlbergariaSJMalvarMdFGCrusoé-RebelloIMGomesBPFdACarvalhoFBdCanal transportation and centering ability of curved root canals prepared using rotary and reciprocating systemsBraz J Oral Sci2015143214218
- BürkleinSHinschitzaKDammaschkeTSchäferEShaping ability and cleaning effectiveness of two single-file systems in severely curved root canals of extracted teeth: Reciproc and WaveOne versus Mtwo and ProTaperInt Endod J201245544946122188401
- DekaABhuyanABhuyanDA comparative evaluation of root canal area increase using three different nickel-titanium rotary systems: an ex vivo cone-beam computed tomographic analysisContemp Clin Dent2015617925684917
- González SánchezJDuran-SindreuFde NoéSMercadéMRoigMCentring ability and apical transportation after overinstrumentation with ProTaper Universal and ProFile Vortex instrumentsInt Endod J201245654255122264187
- PagliosaASousa-NetoMDVersianiMARaucci-NetoWSilva-SousaYTAlfredoEComputed tomography evaluation of rotary systems on the root canal transportation and centering abilityBraz Oral Res201529117
- Pasternak-JúniorBSousa-NetoMSilvaRCanal transportation and centring ability of RaCe rotary instrumentsInt Endod J200942649950619298575
- ElemamRFCapelasJAVazMViriatoNPereiraMdLFLAzevedoÁIn vitro evaluation of root canal transportation after use of BT-Race filesSPEMD20165728793
- RangelSCremoneseRBryantSDummerPShaping ability of RaCe rotary nickel-titanium instruments in simulated root canalsJ Endod200531646046315917688
- AltunbasDKutukBKustarciAShaping ability of reciprocating single-file and full-sequence rotary instrumentation systems in simulated curved canalsEur J Dent20159334626430361
- CeyhanliKKamaciATanerMErdilekNCelikDShaping ability of two M-wire and two traditional nickel-titanium instrumentation systems in S-shaped resin canalsNiger J Clin Pract201518671371726289506
- PalekerFvan der VyverPJComparison of canal transportation and centering ability of K-files, ProGlider File, and G-Files: a micro-computed tomography study of curved root canalsJ Endod20164271105110927178250
- SaberiEAFarhad-MollashahiNNiknamiMMousaviERasuliHEx vivo evaluation of the root form and root canal morphology of the mandibular first molar using CBCT technologyZahedan J Res Med Sci201416716
- ElsheriefSMZayetMKHamoudaIMCone-beam computed tomography analysis of curved root canals after mechanical preparation with three nickel-titanium rotary instrumentsJ Biomed Res201327432633523885273
- PratiwiDSoegihartoBMKrisnawatiBKOrthodontists reproducibility and accuracy in linear and angular measurement on 2d digital and 3d cbct radiographic examinationJDR Clin Trans Res20171039971004
- TumenDSTumenECGunayALacinNCetinSGThe typical appearance and CBCT images of the patient with Papillon–Lefevre syndrome: a case reportJIDMR201583128132
- SchneiderSWA comparison of canal preparations in straight and curved root canalsOral Surg Oral Med Oral Pathol19713222712755284110
- ShortJAMorganLABaumgartnerJCA comparison of canal centering ability of four instrumentation techniquesJ Endod19972385035079587320
- WuMKFanBWesselinkPRLeakage along apical root fillings in curved root canals: Part I. Effects of apical transportation on seal of root fillingsJ Endod200026421020611199720
- HülsmannMPetersOADummerPMMechanical preparation of root canals: shaping goals, techniques and meansEndod Topics20051013076
- StavileciMHoxhaVGörduysusMOLaperreKTatarIHoxhaREffect of endodontic instrumentation technique on root canal geometryInt Endod J2017103952957
- ÖzerSYComparison of root canal transportation induced by three rotary systems with noncutting tips using computed tomographyOral Surg Oral Med Oral Pathol Oral Radiol Endod2011111224425021167759
- VallaeysKChevalierVArbab-ChiraniRComparative analysis of canal transportation and centring ability of three Ni–Ti rotary endodontic systems: Protaper®, MTwo® and Revo-S™, assessed by micro-computed tomographyOdontology20161041838825248755
- Santa-RosaJde Sousa-NetoMDVersianiMAShaping ability of single-file systems with different movements: a micro-computed tomographic studyJ Endod2016113228
- NavósBVHoppeCBMestieriLBBöttcherDESóMVRGreccaFSCentering and transportation: in vitro evaluation of continuous and reciprocating systems in curved root canalsJ Conserv Dent201619547827656071
- JainAAsraniHSinghalACBhatiaTKSharmaVJaiswalPComparative evaluation of canal transportation, centering ability, and remaining dentin thickness between WaveOne and ProTaper rotary by using cone beam computed tomography: an in vitro studyJ Conserv Dent201619544027656063
- VersianiMAPasconEÁde SousaCJABorgesMAGSousa-NetoMDInfluence of shaft design on the shaping ability of 3 nickel-titanium rotary systems by means of spiral computerized tomographyOral Surg Oral Med Oral Pathol Oral Radiol Endod2008105680781318424117
- KunertGGFontanellaVRCde MouraAAMBarlettaFBAnalysis of apical root transportation associated with ProTaper Universal F3 and F4 instruments by using digital subtraction radiographyJ Endod20103661052105520478464
- OzgurUMCehreliZCOzgenMBTasmanDFComparative evaluation of three nickel-titanium instrumentation systems in human teeth using computed tomographyJ Endod200632766867116793477
- Al-SudaniDAl-ShahraniSA comparison of the canal centering ability of ProFile, K3, and RaCe nickel titanium rotary systemsJ Endod200632121198120117174683