
Abstract
Objective
The objective of this study was to compare the cephalometric skeletal and dental characteristics of unilateral complete cleft lip and palate (UCCLP) subjects with and without missing teeth.
Design
A retrospective records review was conducted for patients who are being treated at the cleft lip and palate (CLP) clinics in the College of Dentistry.
Methods
Ninety-six consecutive records of non-syndromic UCCLP subjects were recruited (33 subjects without missing teeth, 50 subjects with only one missing tooth, and 13 subjects with two or more missing teeth). Skeletal and dental characteristics were assessed using lateral cephalometric radiographs in UCCLP subjects with missing teeth and compared to the group with no missing teeth. A total of 25 linear and angular measurements were analyzed and compared between the sample groups.
Results
Of the dental variables tested, overjet was significantly different between the three groups. The UCCLP subjects with multiple missing teeth had the smallest overjet (–3.89±2.75 mm; P=0.015) among the three groups. None of the skeletal characteristics reached statistical significance.
Conclusion
Missing teeth influence the dental but not skeletal characteristics of UCCLP. Overjet is significantly reduced in UCCLP subjects with multiple missing teeth. Future studies with larger sample sizes are warranted.
Introduction
Cleft lip (CL), cleft lip and palate (CLP), and isolated cleft palate (CP) are all referred to as orofacial clefts; they are arguably the most common human craniofacial anomaly.Citation1 Evidence-based research and anecdotal clinical observations have revealed adverse effects on craniofacial growth resulting from orofacial anomalies.Citation2,Citation3 These are caused by the intrinsic effects of the cleft anomaly and possibly as a result of treatment, such as scarring following the surgical closure of the cleft defects.
Orofacial clefts are associated with soft tissue and skeletal and/or dental defects. Such defects may manifest in the form of discontinuity of the lip/alveolar process, missing or malformed teeth, and skeletal deformity in three planes (anteroposterior, vertical, and transverse).Citation4 These defects may consequently decrease the overall oral health–related quality of life in adults and children.Citation5–Citation7 Lisson et alCitation3 argued that surgical interventions influence the dental arch forms and alveolar development which restrict craniofacial growth, and this can be evident in the anteroposterior skeletal dimension.
Although congenitally and/or developmentally missing teeth are seen in individuals with CLP,Citation8–Citation12 this type of dental anomaly varies according to ethnicity, cleft type, and gender.Citation13–Citation17 Cleft width, arch form, and shape of nasal septum can give information about lateral incisor agenesis.Citation18 Furthermore, lateral incisor agenesis had been linked to deficient maxillary growthCitation19,Citation20 and dental arch discrepancy.Citation21
In non-cleft patients, severe hypodontia, with more than six missing teeth has been linked to various craniofacial consequences, including a class III pattern, maxillary and mandibular angular prognathism, and maxillary restriction.Citation22 A previous study have investigated tooth agenesis in cleft patientsCitation23 and assessed anthropometric lip measurements. They found that lip measurements were predictive of the occurrence of dental anomalies (lateral agenesis).Citation24
In a recent study, Wu et alCitation25 evaluated a number of cephalometric characteristics present in Taiwanese individuals with unilateral CLP and found a general reduction in their skeletal vertical dimensions and a reduction in the overjet. Further studies are needed to explore the skeletal and dental characteristics of individuals with unilateral complete cleft lip and palate (UCCLP) in other ethnic groups, particularly Middle Eastern. Therefore, the aim of this study was to compare the cephalometric dentoskeletal characteristics of UCCLP individuals with and without missing teeth.
Materials and methods
Study design
This retrospective study was based on the records of patients with orofacial clefts seen in the clinics of the CLP team. Ethical approval was obtained from the institutional Research Center, King Saud University, Riyadh, Saudi Arabia (PR 0026). Since this was a retrospective study in a teaching hospital where patients consented for their records to be used for research purposes, no further consent was obtained. All records were treated with confidentiality, and patients’ name and personal data were kept anonymous. Skeletal and dental characteristics were assessed in UCCLP individuals with missing teeth and were compared to age- and gender-matched groups of individuals with UCCLP and no missing teeth. Linear and angular measurements obtained from lateral cephalometric radiographs were evaluated and compared between the sample groups.
Sample characteristics
Inclusion criteria were:
Individuals with UCCLP aged 7–14 years
Presence of complete records, including dental/medical files, panoramic radiographs, occlusal radiographs, and lateral cephalograms
Exclusion criteria were:
Patients who had undergone comprehensive orthodontic or orthopedic treatment
Those who had undergone any extraction treatment
Patients with poor-quality records
Patients who had undergone alveolar bone graft (ABG)
Patients who did not adhere to surgical treatment protocol
All patients with UCCLP were treated according to the standard protocol at the CLP team, College of Dentistry. Lip repair is undertaken between 3 and 6 months of age followed by palatal repair at around 9–12 months. An ABG is performed around 9–11 years of age following the diagnosis of bone defect in the cleft site. The graft bone is harvested from the iliac crest. Presurgical orthodontic preparation is usually performed to facilitate the surgical access and primary closure during the alveolar bone grafting. Presurgical orthopedic treatment is not usually provided.
Records of patients who have been treated in the College of Dentistry (King Saud University, Riyadh, Saudi Arabia) from January 1991 to December 2014 were retrieved from the database of the CLP team and the orthodontic clinics. All records that met the inclusion criteria were investigated. Medical records were examined to obtain more data regarding the nature and extension of the cleft. The sample was divided into two main groups depending on the presence or absence of missing permanent teeth; individuals in the control sample (Group 1) had a full set of teeth (excluding third molars), whereas those in Group 2 were missing at least one tooth of any type (excluding third molars). Group 2 was further subdivided into two groups according to the number of teeth each individual was missing: Group 2A was composed of those who had only one missing tooth, and Group 2B included those who were missing two or more teeth.
Diagnosis of missing permanent teeth was made based on an interpretation of panoramic and occlusal radiographs taken between the ages of 7 and 14 years. The lateral cephalometric radiographs were taken prior to the ABG surgery and were traced and analyzed.
All selected cephalometric radiographs were taken with the patient’s head in a natural position and with the teeth in centric occlusion. The radiographs were taken with a Planmeca Proline XC PAN/CEPH X-ray Unit (Planmeca Oy, Helsinki, Finland), set at 66–72 kV and 12 mA, using 0.3–1 seconds of exposure time, following the manufacturer’s instructions. The magnification ratio at the midsagittal plane was 10.74% in the cephalometric film. The lateral cephalograms were scanned using the EPSON Perfection V700 Photo, a dual lens system (Epson Electronics Company, Suwa, Japan). The digitized radiographs were then traced and analyzed using Dolphin Imaging Software® (Version 11.7.05.66; Dolphin Imaging & Management Solutions, Chatsworth, CA, USA).
One calibrated orthodontist traced and analyzed all radiographs after magnification adjustment.
Cephalometric landmarks and measurements
The selected landmarks are shown in . A total of 25 linear and angular measurements were conducted. Seven angular, five linear, and one ratio were measured for skeletal features (). Six angular and five linear dental tissue measurements were measured as well ().
Figure 1 The skeletal, dental, and soft tissue landmarks used in the study.
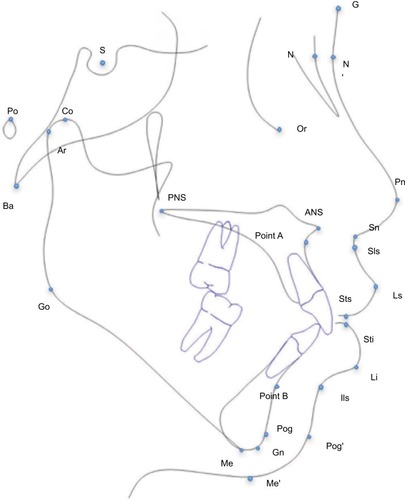
Table 1 Skeletal measurements used in this study
Table 2 Dental measurements used in this study
Statistical analyses
Data were analyzed using SPSS software (SPSS Version 22.0 for Windows; IBM Corporation, Armonk, NY, USA). The normality of the variables was assessed visually and through normality tests (Shapiro–Wilk test). Appropriate statistical tests were used depending on the normality of variables. Comparison of the three groups was performed using the parametric one-way ANOVA, followed by multiple comparison tests using the Bonferroni method when a significant value was found. Since Group 1 was tested against Group 2A and 2B only, the P-value was adjusted to 0.025. The Kruskal–Wallis test followed by the multiple comparison test was used for nonparametric variables.
Intra-examiner reliability
To evaluate intra-examiner reliability, 10 randomly selected lateral cephalometric radiographs were retraced and remeasured on two occasions with a 2-week interval, the two measurements for each radiograph were compared and Cohen Kappa was calculated. Dahlberg’s formula was used to estimate the allocation error of the cephalometric points.
The intra-examiner reliability test (Cohen Kappa) indicated that all variables were highly reliable (r from 0.795 to 0.993), the P-value for the difference between the two sets of cephalometric measurements was not significant. Moreover, calculating the margin of errors using the Dahlberg’s formula showed that the quantity of errors was between 0.2 and 1.2. This reflects highly reliable measures.
Results
The retrieved database included 499 individuals with orofacial cleft, of which 204 had a UCCLP. A total of 96 patients’ records met the preset inclusion criteria, among those 44 were male (45.9%) and 52 were female (54.1%), more details of age and gender distribution are found in .
Table 3 Descriptive data of the sample
The recorded age range of the recruited sample was 9–13 years with a mean of 10.94 years. All cephalometric radiographs were taken at an age of 9 years prior to orthodontic expansion and ABG.
The main reported missing teeth in this study were the lateral incisors on the cleft side, followed by premolars and central incisors. The number of missing teeth ranged from zero to three teeth, with a mean of 1.25 per subject. A detailed distribution of the missing teeth is illustrated in .
Table 4 Distribution of missing teeth in the sample
No differences were found between the three groups in reference to the skeletal cephalometric characteristics (). In terms of dental features, overjet was significantly different among the three groups (P=0.015). The rest of the dental measurements were not statistically significant ().
Table 5 Comparison of skeletal measurements between Groups 1, 2A and 2B using one-way ANOVA and Kruskal–Wallis testTable Footnote*
Table 6 Comparison of dental measurements between Groups 1, 2A, and 2B using one-way ANOVA and Kruskal-Wallis test
Discussion
This study included subjects with UCCLP who had not yet undergone ABG. Grafting serves as a bony support for teeth close to the cleft site, stabilizes the cleft maxillary segments, eliminates the notch in the alveolar ridge, supports the alar base, enables expansion of the maxillary suture, and improves facial symmetry.Citation26 These effects can substantially influence the skeletal and dental cephalometric measurements. The same applies to extraction and orthodontic treatment. Our sample therefore excluded UCCLP subjects who had received ABG or orthodontic treatment with or without extraction.
When measurements in the anteroposterior dimension were assessed, there were no statistically significant differences in the ANB angle and facial convexity among the three groups. In fact, these groups exhibited a Class I skeletal pattern with an ANB angle ranging from 1.59° to 2.33°. These findings were in agreement with Wu et al,Citation25 who showed that these differences were not statistically significant despite the presence, or absence, of certain teeth. However, contrary to Wu et al,Citation25 who found a significant reduction in the lower anterior face height with increasing missing teeth, this study did not find significant differences in lower face height between the groups.
Of the evaluated dental measurements, the overjet was statistically significantly different in the three groups (P=0.015). This coincides with a previous study that found a significant difference in overjet among Taiwanese individuals with UCCLP and missing teeth in comparison with their counterparts without dental anomalies.Citation25 The difference in overjet in our sample can be attributed to teeth tipping toward the anterior spaces, which occur as a result of missing teeth. The lower incisors in our sample were more protruded, relative to the chin (APog line) (P=0.027), further contributing to the reduction in overjet as the number of missing teeth increased.
The reduced overjet in correlation to multiple missing teeth introduces a new challenge to orthodontists who are treating UCCLP, as cleft patients already present with Class III skeletal pattern.Citation4 More reduction in overjet would require more complex treatment to normalize it. In some cases, UCCLP present with Class I skeletal pattern; in such cases, anchorage planning is very critical, especially in the anterior region, where it is required to keep the upper incisors proclined to facilitate overjet correction.
None of the skeletal findings in this study were statistically significant. These results disagree with the findings on non-cleft subjects suffering from a variety of missing teeth. Acharya et alCitation22 reported that missing teeth in the anterior region had a significant effect in terms of the skeletal relationship, as the SNA decreased by 0.3°, SNB decreased by 0.1°, and ANB decreased by 0.2° for every additional missing tooth. Although our findings were not significant, a pattern of ANB reduction can be noticed in the three groups, ANB of 2.33, 2.16, and 1.59 had been recorded for Groups 1, 2A, and 2B, respectively, yet this pattern could not be confirmed or proved.
Ideally, a priori sample size calculation should have been carried out. However, the nature of the studied sample (UCLP) and the extreme difficulty of allocating a good number of patients with good records limited the sample included in our study, especially in Group 2B. Moreover, only 96 (47%) patients of the allocated 204 were recruited, which is due to the restricted inclusion criteria. The recruited sample who received surgical treatment with the same protocol from two surgical teams, although it would be more ideal to recruit the sample from one team work, which will reduce our sample further. Therefore, the results of this study must be considered with caution.
Missing teeth may influence cephalometric features for cleft patients, yet the cause and effect relationship cannot be explained by this cross-sectional study. Future studies should consider conducting longitudinal and multicenter investigations of craniofacial characteristics, along with the inclusion of a larger sample and a wider spectrum of cleft subjects. Also, the effects of cleft shape and size on growth were not verified or recorded in details within the medical notes. Thus, they were not assessed in this study. Nonetheless, all recruited patients were treated by the same team and following a standard protocol. Using 3D reconstruction software from CT scans as opposed to 2D films had been suggested to enable more accurate measurements to be taken specially with superimposed structures.Citation27 However, this cannot be justified due to the excessive radiation.
Oral clefts exhibit a variety of clinical presentations; however, our investigation included only UCCLP anomalies. Nationally, researchers in the CLP field should undertake comprehensive projects to assess all types of orofacial clefts. These longitudinal and comprehensive research studies will enable health care providers to implement valid treatment protocols that are appropriate for the unique nature and complexity of the orofacial cleft population.
Conclusion
Missing teeth influence the dental characteristics of UCCLP. Overjet is significantly reduced in the group with multiple missing teeth. No statistically significant skeletal differences were found across the three groups.
Disclosure
The authors report no conflicts of interest in this work.
References
- CouplandMACouplandAISeasonality, incidence, and sex distribution of cleft lip and palate births in Trent Region, 1973-1982Cleft Palate J198825133373422598
- LissonJAHankeITränkmannJChanges of vertical skeletal morphology in patients with complete unilateral and bilateral cleft lip and palateCleft Palate Craniofac J200542549049416149829
- LissonJASchilkeRTränkmannJTransverse changes after surgical closure of complete cleft lip, alveolus and palateClin Oral Investig1999311824
- ShetyePRUpdate on treatment of patients with cleft—Timing of orthodontics and surgerySemin Orthod20162214551
- WardJAVigKWFirestoneARMercadoAda FonsecaMJohnstonWOral health-related quality of life in children with orofacial cleftsCleft Palate Craniofac J201350217418122236323
- Queiroz HerkrathAPHerkrathFJRebeloMAVettoreMVMeasurement of health-related and oral health-related quality of life among individuals with nonsyndromic orofacial clefts: a systematic review and meta-analysisCleft Palate Craniofac J201552215717224805870
- AntonarakisGSPatelRNTompsonBOral health-related quality of life in non-syndromic cleft lip and/or palate patients: a systematic reviewCommunity Dent Health201330318919524151795
- SuzukiATakahamaYMaxillary lateral incisor of subjects with cleft lip and/or palate: Part 1Cleft Palate Craniofac J19922943763791643070
- JiroutováOMüllerováZThe occurrence of hypodontia in patients with cleft lip and/or palateActa Chir Plast199436253567618404
- TsaiTPHuangCSHuangCCSeeLCDistribution patterns of primary and permanent dentition in children with unilateral complete cleft lip and palateCleft Palate Craniofac J19983521541609527312
- ShapiraYLubitEKuftinecMMHypodontia in children with various types of cleftsAngle Orthod2000701162110730671
- Al-KharboushGHAl-BalkhiKMAl-MoammarKThe prevalence of specific dental anomalies in a group of Saudi cleft lip and palate patientsSaudi Dent J2015272758026082573
- AizenbudDCamasuviSPeledMBrinICongenitally missing teeth in the Israeli cleft populationCleft Palate Craniofac J200542331431715865468
- PegelowMAlqadiNKarstenALThe prevalence of various dental characteristics in the primary and mixed dentition in patients born with non-syndromic unilateral cleft lip with or without cleft palateEur J Orthod201234556157021750243
- ParanaibaLMColettaRDSwertsMSQuintinoRPde BarrosLMMartelli-JúniorHPrevalence of Dental Anomalies in Patients With Nonsyndromic Cleft Lip and/or Palate in a Brazilian PopulationCleft Palate Craniofac J201350440040521973329
- MikulewiczMOgińskiTGedrangeTBerniczei-RoykoAPrussakEPrevalence of second premolar hypodontia in the Polish cleft lip and palate populationMed Sci Monit20142035536024584216
- Al JamalGAHazza’aAMRawashdehMAPrevalence of dental anomalies in a population of cleft lip and palate patientsCleft Palate Craniofac J201047441342020590463
- DoucetJCDelestanCMontoyaPNew neonatal classification of unilateral cleft lip and palate part 2: to predict permanent lateral incisor agenesis and maxillary growthCleft Palate Craniofac J201451553353923621660
- AntonarakisGSFisherDMPermanent Tooth Agenesis and Maxillary Hypoplasia in Patients with Unilateral Cleft Lip and PalatePlast Reconstr Surg20151365648e656e
- LaiLHHuiBKNguyenPDLateral incisor agenesis predicts maxillary hypoplasia and Le Fort I advancement surgery in cleft patientsPlast Reconstr Surg20151351142e148e
- HardwickeJChhabraPRichardBAbsent maxillary lateral incisor as evidence of poor midfacial growth in unilateral cleft lip and palateOral Surg Oral Med Oral Pathol Oral Radiol2015119439239525660277
- AcharyaPNJonesSPMolesDGillDHuntNPA cephalometric study to investigate the skeletal relationships in patients with increasing severity of hypodontiaAngle Orthod201080451151820482356
- LaiMCKingNMWongHMAbnormalities of maxillary anterior teeth in Chinese children with cleft lip and palateCleft Palate Craniofac J2009461586419115788
- AntonarakisGSFisherDMPresurgical Unilateral Cleft Lip Anthropo-metrics and the Presence of Dental AnomaliesCleft Palate Craniofac J201552439540424437562
- WuTTKoEWChenPKHuangCSCraniofacial characteristics in unilateral complete cleft lip and palate patients with congenitally missing teethAm J Orthod Dentofacial Orthop2013144338139023992810
- Kuijpers-JagtmanAMLongREThe influence of surgery and orthopedic treatment on maxillofacial growth and maxillary arch development in patients treated for orofacial cleftsThe Cleft Palate-Craniofacial Journal200037611210670881
- TulunogluOEsenlikEGulsenATulunogluIA comparison of three-dimensional and two-dimensional cephalometric evaluations of children with cleft lip and palateEur J Dent20115445145821912501