
Abstract
Introduction
Airway management in patients with panfacial fracture remains a challenge to anesthesiologists and surgeons. Submental intubation is an effective and less invasive alternative to tracheostomy during intraoperative airway management where orotracheal and nasotracheal intubation are not appropriate options. In addition, submental intubation allows proper access to oronasal airways and occlusion during intraoperative management.
Methods
The descriptive retrospective study was carried out and evaluated the outcomes of submental intubation in the management of panfacial fracture, complex maxillary or mandible fracture associated with nasal bone fracture and naso-orbito-ethmoid (NOE) fracture. The medical records of 23 patients who received submental endotracheal intubation were reviewed at UCMS College of Dental Surgery, Bhairahawa, Rupandehi, Nepal from March 2014 to December 2018. The following parameters were evaluated: mode of trauma, time required for intubation, accidental extubation, accidental perforation of the pilot balloon during its insertion, period of hospital stay, post-operative complications, such as the healing of submental scars both intraorally and extraorally.
Results
The submental intubation was successfully done in all patients with minimal obvious post-operative complications. The mode of trauma for majority of cases of panfacial fracture who underwent submental intubation was road traffic accident (69.56%). The mean time required for intubation was 8.43 (±0.84) minutes. No accidental extubations occurred. Accidental perforation of the pilot balloon was seen in one patient (4.35%) during tube manipulation which was managed successfully by changing the tube. The healing of submental scars was uneventful intraorally and extraorally in almost every case. The mean period of hospital stay in patients with submental intubation was 7.95 (±1.49) days.
Discussion
Submental intubation is an effective and safe method as it is not associated with complications of tracheostomy during management of panfacial fracture, NOE fracture and craniofacial fracture. In addition, it does not interfere with IMF during intraoperative period.
Introduction
Panfacial fractures are simply defined as those involving the upper, middle, and lower thirds of face simultaneously. These complex injuries are fractures that involve the frontal bones, zygomaticomaxillary complex, NOE region, maxilla and mandible. Panfacial trauma management is always a challenge for maxillofacial surgeons as well as anesthetists, not only to achieve the facial aesthetic/contour but also to get the satisfactory functional end results with selection of proper intubation techniques. Airway management in panfacial trauma during the intraoperative period is often a crucial and difficult task.Citation1
Isolated mandible and/or midface fracture can be managed by either orotracheal or nasotracheal intubation technique. However, nasotracheal intubation technique precludes the treatment of nasal fracture and orotracheal intubation interferes with IMF, comprising the proper reduction and stabilization of mandible and maxillary fractures. The choice of anesthetic techniques has always been a great challenge for midface and/or mandible fractures associated with isolated nasal bone fractures or NOE fractures.Citation2,Citation3
Other procedures such as tracheostomy or cricothyroidotomy can be alternative procedures for effective intraoperative airway management while dealing with such complex fractures. However, this might be associated with a significant number of complications. The most documented complications are hemorrhages due to injury to the thyroid gland and its adjacent vessels, surgical emphysema, pneumothorax, recurrent laryngeal nerves damage, cardiac arrest caused by vagal nerve stimulation, wound infections, post-hypercapnic shock, tracheomalacia, acute pulmonary edema, air embolism, tracheal stenosis, tracheoesophageal fistula and hypertrophic scars.Citation4–Citation8 However, tracheostomy is one of the most accepted methods of airway management in patients requiring mechanical ventilation to avoid injuries to the vocal cords and in those with acute airway obstruction.Citation9 But patient morbidity and complications associated with these procedures made surgeons and anesthetists to opt for more effective methods.
To overcome these difficulties with minimal complications, Hernandez Altemir (1986) proposed a novel submental intubation technique which involved passing the endotracheal tube through an extraoral incision in the submental region in the floor of the mouth intraorally. The literature recommended that this intubation technique would help in securing airways with unhindered intraoral surgical fields, and in addition allowed for IMF, at the same time evading the aforesaid drawbacks and complications.Citation10 In addition, it ensures the surgical field is free of endotracheal tube during surgery in a coronal approach. Out of all the difficulties, submental intubation is a minimally traumatic procedure which overcomes most of the difficulties in panfacial trauma. Thus, the present study aimed to prove that submental intubation is most effective alternative for airway management in patients with panfacial trauma during general anesthesia.
Materials and Methods
The design of the study was a descriptive retrospective study which was approved by the Institutional Review Committee (IRC) of the Universal College of Medical Sciences, Bhairahawa, Nepal (IRC number 044/19). Written informed consent from patients was obtained for the publication of their data and images.
Among 498 cases of maxillofacial trauma registered between March 2014 to December 2018 at UCMS College of Dental Surgery, Bhairahawa, Rupandehi, Nepal; 23 submental intubations were performed for panfacial trauma. Patients with midface fractures (Le Fort I, Le Fort II, Le Fort III), along with frontal or NOE and mandibular fractures planned for open reduction internal fixation, and in whom submental intubation was done were selected for the study. Parameters recorded were personal details of patient, mode of trauma, type of maxillofacial trauma, intubation time, accidental extubation, accidental perforation of the pilot balloon during its insertion, period of hospital stay and any post-operative complications including the healing of submental scars. Polytrauma patients with concomitant severe head injury; serious thoracic injury; patients for whom more than two major operations were expected; patients who require mechanical ventilation for more than 8 days after surgical management, as tracheostomy is the choice as per protocol were excluded from the study.Citation3,Citation11 Patients with incomplete medical records were not included in the study.
The technique used for submental intubation was followed as per the technique published by Hernandez Altemir (1986).Citation10
Surgical Technique
After the patient was intubated successfully with orotracheal intubation, standard skin preparation with 10% povidone-iodine solution was carried out, followed by temporary draping of the mouth and submental area. An incision of approximately 1.5–2 cm was made along the paramedian submental region, next to the medial aspect of the inferior border of the mandible as shown in . Skin, subcutaneous tissue, platysma and mylohyoid muscles were passed through using a curved hemostat which was in close approximation with the lingual cortex of the mandible. Tenting of the mucosal layer is appreciated in the floor of the mouth and an incision was made in the most prominent part of hemostat. After the incision, artery forceps were opened creating a surgical tunnel through which the endotracheal tube can be passed easily. The tube cuff was first deflated and the artery forceps was inserted intraorally and the pilot balloon of the tube was grasped and pulled gently outside and secured. Precaution should be taken to look for perforation which can be checked by inflating the balloon. The artery forceps was reintroduced into the tunnel and the proximal end of the endotracheal tube was pulled out as shown in . The tube was then attached to the connector and the circuit was re-established as shown in . In between the procedures, the oxygen saturation of the patient should be monitored. Auscultation was carried out by the anesthetist to confirm the accurate position of tube. A throat pack in the form of ribbon gauze was then inserted to protect the pharynx from blood and debris intraoperatively. 3–0 silk sutures were placed around the tube to secure it, thus minimizing intraoperative tube movement and preventing accidental extubation. After the procedure is completed, the sutures around the tube were removed and the pilot balloon was deflated and submental intubation was transformed into orotracheal intubation in reverse. The skin wound was closed with simple interrupted sutures using 5–0 prolene® extraorally while intraoral wound with 4–0 vicryl®.
Figure 1 Incision made at submental region after orotracheal intubation.

Figure 2 Endotracheal tube has been passed from oral to submental through surgically created tunnel.

Figure 3 Endotracheal tube is connected to circuit after successful switch of tube from oral to submental.

Data were entered in Microsoft Excel 2007 and analyzed by means of Statistical Package for Social Sciences (SPSS 18.0 for Windows, SPSS Inc.). For descriptive statistics; percentage, mean, range and standard deviation were calculated.
Results
A total of 23 subjects with panfacial fractures with complete medical records who were surgically treated and managed successfully with submental intubation within the study period were included in the study. Patients' demographic data, type of fracture, time duration for submental intubations and period of hospital stays are illustrated in .
Table 1 Descriptive Data of Patients
The selected group included 18 male (78%) and 5 female (22%) subjects as shown in . The mean age was 30.3 ± 10.74 years (age range, 17–42 years) as shown in . The mode of trauma were from road traffic accidents (69.56%), followed by fall from height (17.39%), and physical assault (13.04%) as shown in . Individual site fracture distribution is shown in . The mean duration of submental intubation was 8.43 ± 0.84 mins (range, 7–10 mins) as shown in . During intra-operative tube manipulation, pilot balloon perforation was observed in one case (4.35%) which was managed by replacing the tube with other one as shown in . No accidental extubation of tube was present. The mean post-operative hospital stay after surgery was 7.95 ±1.49 days (range, 6–12 days) in which the maximum hospital stays were patients associated with craniofacial fracture as shown in . All 23 patients were successfully extubated in the operation theater itself. Patients were evaluated post-operatively at 1 week, 1 month and 4 months. No post-operative complications such as motor or sensory salivation deficit, bleeding or infections were noted. Intraoral wound healing was satisfactory. The scar had been well accepted by the patients without any hypertrophic scarring or keloid formation, except in one subject where there was a hypertrophic scar and this was managed with intralesional steroid therapy as shown in .
Table 2 Mean Intubation Time, Age and Hospital Stays of Patients
Figure 4 Gender distribution of panfacial fracture.
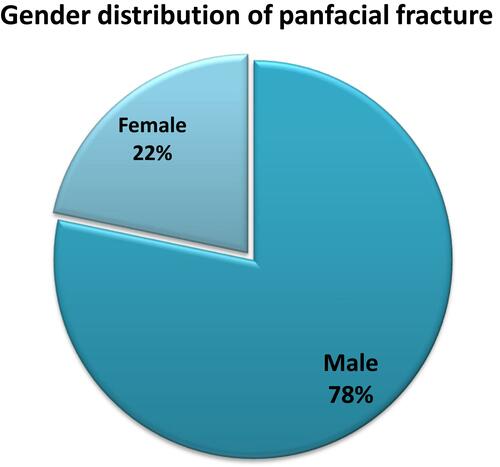
Figure 5 Mode of trauma in panfacial fracture.
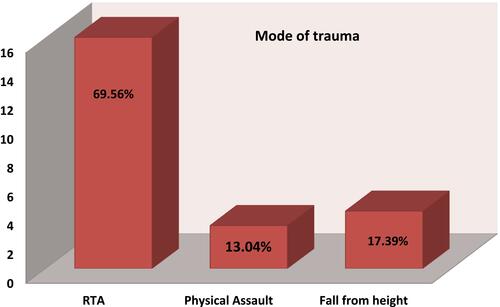
Figure 6 Individual site fracture distribution of patients who have undergone submental intubation.
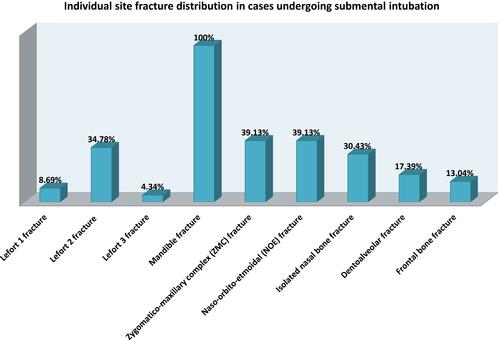
Figure 7 Intraoperative pilot balloon perforation of endotracheal tube.
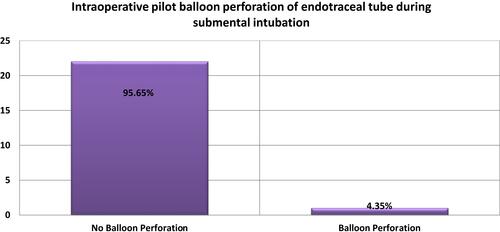
Figure 8 Post-operative complications in patients who have undergone submental intubation.
Discussion
Intraoperative airway management is a very challenging task in panfacial reconstruction surgery and has gone through major breakthroughs since the application of submental intubation. The major indication for submental intubation is when there is a need for fixation of the mid face and mandible, combined with isolated nasal or NOE bone fracture to ensure an intact occlusion.Citation9,Citation10
Oral intubation is a common procedure in securing the airway but it interferes with the clear surgical field intraorally and poses difficulties in assessing occlusion during the intraoperative period. So nasotracheal intubation is an the alternative approach to orotracheal intubation and most frequently used in managing oral and maxillofacial trauma. However, nasotracheal intubation is contraindicated in basilar skull fractures due to the incidence of accidental intracranial placement,Citation10 possible cerebrospinal fluid leak, and/or cerebro-meningeal infections,Citation2 epistaxis, pharyngeal injury, external nares pressure necrosis, recurrent middle ear infections, sinusitis, sepsis and difficulty in passing a nasal tube.Citation12–Citation14
Tracheostomy is the preferred option in patients with panfacial trauma where there is need for prolonged intubation. Numerous complications have been documented in various literatures, ranging from simple to life threatening.Citation4–Citation8 There have been several options for short-term airway management which include retromolar intubation and nasal tube switch technique. The literature reveals that retromolar intubation has various disadvantages such as being more traumatic, obtrusive, expensive and time consuming.Citation15 Another alternative nasal tube switch technique had complications, such as the need for intraoperative re-intubation, aspiration due to posterior nasal bleed, difficulty in maintaining airway with the need for tracheostomy and possible loosening of plates and screws due to excessive load on fixations.Citation16
Submental intubation was first described by Hernandez AltemirCitation10 in 1986. After its development, it has been used as a first choice technique for intra-operative airway management in complex maxillofacial injuries. Panfacial trauma is one of the most common indicators for submental endotracheal intubation.Citation17
Various modifications of Altemir’s technique have been reported in the literature with their own advantages and disadvantages. Anatomic modification includes Stoll et al,Citation18 MacInnis and Baig,Citation19 Taglialatela et alCitation20 and Mahmood et al.Citation21 Anesthetic modification includes Green and Moore,Citation22 Altemir and Montero,Citation23 Drolet et al,Citation24 Amin et alCitation25 and Lim et al.Citation26 In our study, we performed Altemir’s original technique for submental intubation for management of panfacial fractures as per departmental protocol. Contraindications for this technique are infection at the site of incision, bleeding diathesis, disrupted laryngotracheal anatomy and a restricted retromolar space to allow suctioning.Citation25
There are various reported complications associated with submental endotracheal intubation. The major complication is accidental extubationCitation25 which can be further prevented via placing a stay suture around tube. Other complications are wound infections, endotracheal tube damage, tube dislodgement or obstruction, transient lingual nerve paresthesia, bleeding and submental hypertrophic scar.Citation17
In this study, submental endotracheal intubations were successfully carried out in all panfacial trauma patients with no major intra-operative or post-operative complications, allowing the operating surgeon to manipulate fractured bone freely as well as help to establish maxillomandibular fixation without any restrictions. Moreover, patients extubation after the surgical procedure was uneventful, without any long-term post-operative patient morbidity. Other associated possible post-operative complications such as oro-cutaneous fistula, traumatic injuries to the submandibular and sublingual glands or ducts, accidental extubations, lingual nerve damage were not observed. A hypertrophic scar was observed in one patient which was treated with intralesional steroid 6 months after the procedure. During tube manipulation from intraoral to extraoral submental plane, pilot balloon perforation was seen in one patient which was successfully managed by replacing the tube with another.
Submental intubation could be an effective technique with minimal patient morbidity, precautions must be considered by both surgeons and anesthesiologists. Initial airway management is challenging with complex maxillofacial trauma patients. After the airway has been secured by orotracheal intubation, submental intubation is always a second step during panfacial trauma management. The endotracheal tube must be firmly held intraorally to prevent accidental extubation during tube manipulation. Blunt dissection with the artery forceps must be carried out in close approximation to the medial border of the mandible to avoid injuries to the salivary glands and ducts.
Conclusion
Submental intubation is one of the definitive alternatives to tracheostomy in panfacial trauma patients, along with nasal or NOE fractures, who do not require prolonged ventilatory support. The major advantage is assessment and manipulation of occlusion during surgery without any hindrances and facilitate during surgery for associated nasal and skull base trauma. It has been proven a safe and effective technique with less morbidity, minimal complications and avoids tracheostomy related complications.
Abbreviations
NOE, Naso-orbito-ethmoid; IMF, Intermaxillary fixation; ZMC, Zygomaticomaxillary complex.
Disclosure
The authors report no conflicts of interest in this work.
References
- Mohan R, Iyer R, Thaller S. Airway management in patients with facial trauma. J Craniofac Surg. 2009;20:21–23. doi:10.1097/SCS.0b013e318190327a
- Biglioli F, Mortini P, Goisis M, Bardazzi A, Boari N. Submental orotracheal intubation: an alternative to tracheotomy in transfacial cranial base surgery. Skull Base. 2003;13:189–195. doi:10.1055/s-2004-817694
- Shetty PM, Yadav SK, Upadya M. Submental intubation in patients with panfacial fractures: a prospective study. Indian J Anaesth. 2011;55:299–304. doi:10.4103/0019-5049.82685
- Bernard AC, Kenady DE. Conventional surgical tracheostomy as the preferred method of airway management. J Oral Maxillofac Surg. 1999;57:310–315. doi:10.1016/S0278-2391(99)90679-1
- Wood DE, Mathisen DJ. Late complication of tracheotomy. Clin Chest Med. 1991;12:597–609.
- Goldenberg D, Golz A, Netzer A, Joachims HZ. Tracheotomy changing indications and a review of 1130 cases. J Otolaryngol. 2002;31:211–215. doi:10.2310/7070.2002.21091
- Viau F, Lededente A, Le Tinier JY. Complications des trach´ eotomies. Rev Pneumol Clin. 1988;44:24–32.
- Nwoku AL, Al-Balawi SA, Al-Zahrani SA. A modified method of submental oroendotracheal intubation. Saudi Med J. 2002;23:73–76.
- Rodrigues WC, de Melo WM, de Almeida RS, Pardo-Kaba SC, Sonoda CK, Shinohara EH. Submental intubation in cases of panfacial fractures: a retrospective study. Anesth Prog. 2017;64:3, 153–61. doi:10.2344/anpr-64-04-07
- Hernández Altemir F. The submental route for endotracheal intubation: a new technique. J Maxillofac Surg. 1986;14:64–65. doi:10.1016/S0301-0503(86)80261-2
- Heffner JE. The technique of tracheotomy and cricothyroidotomy. When to operate and how to manage complications. J Crit Illn. 1995;10:561–568.
- Schultz RC. Nasotracheal intubation in the presence of facial fractures. Plast Reconstr Surg. 1990;86:104–106. doi:10.1097/00006534-199011000-00053
- Fonseca R, Walker R. Oral and Maxillofacial Trauma. 2nd ed. Philadelphia: WB Saunders; 1997:105–135.
- Hall DB. Nasotracheal intubation with facial fractures. JAMA. 1989;261:1198.
- Martinez- Lage JL, Eslava JM, Cebrecos AI, Marcos O. Retromolar intubation. J Oral Maxillofac Surg. 1998;56:302–306. doi:10.1016/S0278-2391(98)90103-3
- Werter JR, Richardson G, Mcilwain MR. Nasal tube switch: converting from nasal to an oral endotracheal tube without extubation. J Oral Maxillofac Surg. 1994;52:994–996. doi:10.1016/S0278-2391(10)80090-4
- Jundt JS, Cattano D, Hagberg CA, Wilson JW. Submental intubation: a literature review. Int J Oral Maxillofac Surg. 2012;41:46–54. doi:10.1016/j.ijom.2011.08.002
- Stoll P, Galli C, Wachter R, Bahr W. Submandibular endotracheal intubation in panfacial fractures. J Clin Anesth. 1994;6:83–86. doi:10.1016/0952-8180(94)90127-9
- MacInnis E, Baig M. A modified submental approach for oral endotracheal intubation. Int J Oral Maxillofac Surg. 1999;28:344–346. doi:10.1034/j.1399-0020.1999.285280506.x
- Taglialatela S, Maio G, Aliberti F. Submento-submandibular intubation: is the subperiosteal passage essential? Experience in 107 consecutive cases. Br J Maxillofac Surg. 2006;44:12–14. doi:10.1016/j.bjoms.2005.07.011
- Mahmood S, Lello G. Oro endotracheal intubation: mediansubmental (retrogenial) approach. J Oral Maxillofac Surg. 2002;60:473–474. doi:10.1053/joms.2002.31244
- Green JD, Moore UJ. A modification of sub-mental intubation. Br J Anaesth. 1996;77:789–791. doi:10.1093/bja/77.6.789
- Altemir FH, Montero SH. The submental route revisited using the laryngeal mask airway: a technical note. J Craniomaxillofac Surg. 2000;28:343–344. doi:10.1054/jcms.2000.0175
- Drolet P, Girard M, Poirier J, Grenier Y. Facilitating submental endotracheal intubation with an endotracheal tube exchanger. Anesth Analg. 2000;90:222–223. doi:10.1097/00000539-200001000-00044
- Amin M, Dill-Russell P, Manisali M, Lee R, Sinton I. Facial fractures and submental tracheal intubation. Anaesthesia. 2002;57:1195–1199. doi:10.1046/j.1365-2044.2002.02624_1.x
- Lim HK, Kim IK, Han JU. Modified submental orotracheal intubation using the blue cap on the end of the thoracic catheter. Yonsei Med J. 2003;44:919–922. doi:10.3349/ymj.2003.44.5.919