
Abstract
Background
There are controversies on the causal role of H. pylori in duodenal ulceration. Helicobacter pylori are curved gram-negative microaerophilic bacteria found at the layer of gastric mucous or adherent to the epithelial lining of the stomach. It’s a public health significance bacteria starting from discovery, and the prevalence and severity of the infection varies considerably among populations. H. pylori are a risk for various diseases, while the extent of host response like gastric inflammation and the amount of acid secretion by parietal cells affects the outcome of infection.
Method
Relevant literature were searched from databases such as Google Scholar, PubMed, Hinari, Web of Science, Scopus, and Science Direct.
Result
The review evidence supports a strong causal relation between H. pylori infection and duodenal ulcer, as patients are more likely to be infected by virulent strains which later cause duodenal ulceration. Thus, eradication of H. pylori infection decreases the incidence of duodenal ulcers, and prevents its recurrence by reducing both basal gastrin release and acid secretion without affecting parietal cell sensitivity. On the other hand, some studies show that H. pylori infection is not associated with the development of duodenal ulcers and such a lack of association revealed that duodenal ulceration has different pathogenesis.
Conclusion
Despite controversies observed in the causal role of H. pylori to duodenal ulceration by various studies, Hill criteria of causation proved the presence of a causal relation between H. pylori infection and duodenal ulcers. Other factors are also responsible for the development of duodenal ulcers and such factors are responsible for the differences in the prevalence of the diseases.
Introduction
Helicobacter pylori (H. pylori) are curved, gram-negative, microaerophilic bacteriaCitation1 found in the gastric mucous layer or adherent to the epithelial lining of the stomach.Citation2 It has been a public health significance bacteria since 1983 as it infects the duodenum where hydrochloric acid and pepsin play a role in the digestion of food, which facilitates damage of the lining by gastric acid.Citation3 H. pylori can elevate acid secretion in people who develop duodenal ulcersCitation4 or hypersecretion of gastric acid can by itself evoke duodenal ulcers.Citation5
The prevalence and the severity of the infection vary considerably among populationsCitation6 due to geographical differences and ways of leading life.Citation4 In the US, 30–40% of people are infected with H. pyloriCitation7 and the prevalence is still high in Eastern Mediterranean countries of the healthy asymptomatic population.Citation8 Most of the infection occurred during childhood with no difference in gender.Citation9
Before the discovery of H. pylori, spicy food, acid, stress, and lifestyle were considered to be the causes of ulcers.Citation2 Age, religion, and water sources are risk factors for H. pylori infection in Indonesia.Citation10 Poor socio-economic status, genetic predisposition, and being resident in a developing country are among known risk factors for H. pylori infection.Citation11 Sharing food or eating utensils, contact with contaminated water and with the stool, saliva, or vomit of an infected person are also potential risk factors.Citation3,Citation11
Dye endoscopy, forceps biopsies for culture, histology, and rapid urease test are used for diagnosis of H. pylori infection, and a patient is considered negative when the serum anti-H. pylori IgG and the three tests on biopsied specimens are all negative.Citation12 H. pylori are associated with an increased risk for the development of duodenal and gastric ulcers, gastric adenocarcinoma, and gastric B-cell lymphoma.Citation6,Citation9 The bacterium attaches to epithelial cells of the stomach and duodenum, then it causes damage to the cells by secreting degradative enzymes (urease, lipases, and proteases) and bacterial virulence factors (cytotoxin-associated gene protein (CagA) and vacuolating cytotoxin (VacA)), and initiating a self-destructive immune response.Citation13 Eradication of infection reduces the risk of duodenal ulcer,Citation14 but the outcome depends on the extent of host response to the infection like gastric inflammation and the amount of acid secretion by parietal cells.Citation4 This review article aims to explore the controversies on the causal role of H pylori in duodenal ulcers.
Methods
Studies were obtained from electronic databases, including Google Scholar, PubMed, Hinari, Web of Science, Scopus, and Science Direct, with hand searches and iterative reviews of reference lists of papers using the keywords “H. Pylori”, “duodenal ulcer”, “causation” and in combination from February 7–13, 2019. A total of 107 papers were obtained from all sources. After the exclusion of redundant and irrelevant literature, a total of 26 separate published empirical articles () in peer-reviewed journals were reviewed. The searching process is displayed in .
Figure 1 Data searching process.
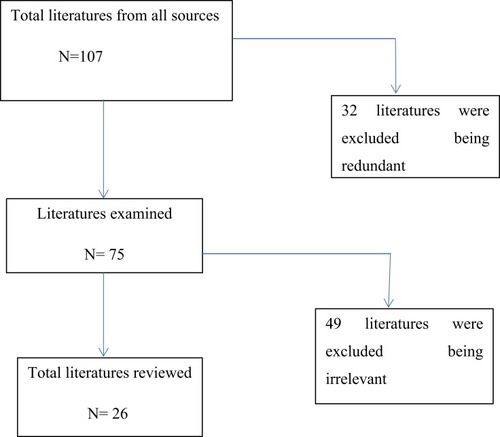
Table 1 Study Characteristics Of Reviewed Articles
The inclusion criteria were: type of study; randomized clinical trial, case-control, cohort, ecological, and cross-sectional, and systematic review, publication; academic journal (peer-reviewed) and non-reviewed reports, population; Global, time-period: 1989 to present, and language; English.
Result And Discussion
Evidence On Causal Relation Between H. pylori Infection And Duodenal Ulcer
H. pylori has a role in the etiology of duodenal ulcer.Citation15–Citation17 Once ingested, the attachment of H. pylori to epithelial cells of the stomach and duodenum occurs through phosphorylation of a 145 kilo Dalton protein and activation of signal transduction pathways.Citation18,Citation19 H. pylori infection blocks normal physiological mechanisms resulting in increased gastrin release and impaired inhibition of gastric acid secretion.Citation18,Citation20 Such endogenous hypersecretion of acid causes gastric metaplasiaCitation4 and synergizes ulceration.Citation21 Thus, the prevalence of H. pylori infection in duodenal ulcer patients is higher than the normal population,Citation22 as patients are more likely to be infected with virulent strains which later cause duodenal ulceration.Citation23 The disease manifestations start when alteration of epithelial cell growth and enhanced apoptosis occur.Citation24 H. pylori containing functional Cag pathogenicity island produce a vigorous inflammatory response,Citation25 and 12% of patients develop late complications with a further 6% mortality rate.Citation26
H. pylori plays a role in the pathogenesis of duodenal ulcer disease in 84.9% of subjects and the single causative factor in 44.1% of patients.Citation27 Duodenal infection with H. pylori is a strong risk factor (RR=51),Citation21 (OR=4)Citation28 for the development of duodenal ulceration. Antral reinfection with H. pylori is also associated with relapseCitation29 (RR=7.6).Citation21 This evidence supports a strong causal relation between H. pylori infection and duodenal ulceration.Citation30
Preexisting history of H. pylori is a risk for the development of duodenal ulcer,Citation28 and it is observed that in young Israelis with an odds ratio of 3.8, the association increased as diagnosis time exceeded 2 years with 56.6% attributable risk.Citation31
Although cigarette smoking, age, sex, and ingestion of non-steroidal anti-inflammatory drugs (NSAID) were not found to be significant risk factors for duodenal ulceration,Citation21,Citation32 H. pylori infection plays a role in the causation of non-NSAID-induced duodenal ulcer perforation.Citation33 Excluding patients taking NSAIDs and/or antibiotics, H. pylori prevalence increased up to 99.1% (98.1±99.6%) among duodenal ulcer patients.Citation34
The current therapy for H. pylori induced ulcer (a proton pump inhibitor and at least two antimicrobials with or without bismuth) is highly effective in eradicating the infection.Citation9 Eradication of H. pylori infection decreases the incidence of duodenal ulcer and prevents its recurrence,Citation22,Citation35–Citation37 and the occurrence of NSAID induced peptic ulcersCitation16 without altering acid output.Citation38 As a result, eradication resulted in falls in both basal gastrin release and acid secretion without affecting parietal cell sensitivity.Citation39 On the other hand, the clinical outcome of eradication therapy over 2 years is significantly poorer in H. pylori-negative patients.Citation7
Evidence Against Causal Relation Between H. pylori Infection And Duodenal Ulcer
A cohort study of 73 participants revealed that prior life acquisition of H. pylori was not associated with duodenal ulcerCitation40 and only a minority of infected persons develop duodenal ulceration.Citation22 This indicates that different pathogenesis had existed for duodenal ulceration.Citation32 Moreover, H. pylori strain with high number of CagA EPIYA-C segments was not associated with duodenal ulcer.Citation41
Duodenal ulcer can relapse after eradication of H. pylori infection, and the ulcer may remain healed after reduction of acid secretion in the presence of infection. Additionally, hypersecretion of gastric acid is strongly associated with the development of duodenal ulcers while it may result in a spontaneous eradication of H. pylori infection.Citation23 The virulent strains cause delayed healing of an ulcer produced by acid hypersecretionCitation42 by interfering with neoangiogenesis of wounded duodenal epithelial cellsCitation23 indicating the bacteria delay the healing of ulcer rather than causing it.
The annual proportion of patients with H. pylori-negative duodenal ulcers increased as the ulcers are more likely to occur in individuals with old age, pre-existing malignancy, recent surgery, underlying sepsis,Citation43 NSAID use,Citation43–Citation45 a concomitant medical problem like Crohn’s disease and hypergastrinaemia,Citation46 specific geographical distribution,Citation47 and recent intake of antibiotics.Citation44 Smoking and the presence of dietary lipids are also risk factors.Citation4,Citation23 Among 71 H. pylori-positive duodenal ulcer patients, 66% had no other detectable causal factors, 30% were regularly taking NSAIDs, and 4% had malignancy.Citation17 Thus, H. pylori is not the primary cause of duodenal ulcer.Citation47
Evaluation Of Causal Relation Between H. pylori Infection And Duodenal Ulcer Through Hill’s Criteria
The review assessed the causal relation between H. pylori infection and duodenal ulcer by using criteria for assessing causation proposed in 1965 by Sir Austin Bradford Hill. Despite controversies observed on the causal role of H. pylori to duodenal ulceration in various literature, Hill criteria of causation proved a causal relation between H. pylori infection and duodenal ulcer ().
Table 2 Hill Criteria For Assessing The Causal Role Of H. Pylori On Duodenal Ulcer
Conclusion
There are controversies among studies on the causal relation between H. pylori infection and duodenal ulcer. Several studies reported H. pylori is a strong risk factor for the development of duodenal ulcers, whereas other studies showed duodenal ulcers can recur after eradication of H. pylori infection, and the ulcer may remain healed after reduction of acid secretion in the presence of active infection, indicating the absence of a causal relation between H. pylori infection and duodenal ulcer. Despite controversies observed in the causal role of H. pylori to duodenal ulcer by various studies, critical examination of empirical evidence through Hill criteria of causation proved the presence of a causal relation between H. pylori infection and duodenal ulcer.
Abbreviations
H. pylori, Helicobacter pylori, NSAID, Non-steroidal anti-inflammatory drug.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgment
We are thankful to Wollo University for providing the necessary facilities for this work.
Disclosure
The authors report no conflicts of interest in this work.
References
- Mohebtash M. Helicobacter pylori and its effects on human health and disease. Arch Iran Med. 2011;14(3):192.21529109
- CDC. Helicobacter Pylori Fact Sheet for Health Care Providers.CDC Stacks. 1998.
- Ra A, Tobe SW. Acute interstitial nephritis due to pantoprazole. Anns Pharmacother. 2004;38(1):41–45. doi:10.1345/aph.1D085
- Calam J, Baron J. ABC of the upper gastrointestinal tract: pathophysiology of duodenal and gastric ulcer and gastric cancer. Br Med J. 2001;323(7319):980. doi:10.1136/bmj.323.7319.98011679389
- Olbe L, Fändriks L, Hamlet A, Svennerholm A-M, Thoreson A-C. Mechanisms involved in Helicobacter pylori induced duodenal ulcer disease: an overview. World J Gastroenterol. 2000;6(5):619. doi:10.3748/wjg.v6.i5.61911819661
- Cover TL, Blaser MJ. Helicobacter pylori in health and disease. Gastroenterology. 2009;136(6):1863–1873. doi:10.1053/j.gastro.2009.01.07319457415
- Bytzer P, Teglbjærg PS, Group DUS, Group US. Helicobacter pylori–negative duodenal ulcers: prevalence, clinical characteristics, and prognosis—results from a randomized trial with 2-year follow-up. Am J Gastroenterol. 2001;96(5):1409–1416. doi:10.1111/j.1572-0241.2001.03774.x11374675
- Eshraghian A. Epidemiology of Helicobacter pylori infection among the healthy population in Iran and countries of the Eastern Mediterranean Region: a systematic review of prevalence and risk factors. World J Gastroenterol. 2014;20(46):17618. doi:10.3748/wjg.v20.i46.1761825516677
- Luman W. Helicobacter pylori: causation and treatment. JR Coll Physicians Edinburgh. 2005;(35):45–49.
- Syam AF, Miftahussurur M, Makmun D, et al. Risk factors and prevalence of Helicobacter pylori in five largest islands of Indonesia: A preliminary study. PLoS One. 2015;10(11):e0140186. doi:10.1371/journal.pone.014018626599790
- Das JC, Paul N. Epidemiology and pathophysiology of Helicobacter pylori infection in children. J Indian Pediatr. 2007;74(3):287–290. doi:10.1007/s12098-007-0046-6
- Tsuji H, Kohli Y, Fukumitsu S, et al. Helicobacter pylori-negative gastric and duodenal ulcers. J Gastroenterol. 1999;34(4):455–460. doi:10.1007/s00535005029610452677
- Costa AC, Figueiredo C, Touati E. Pathogenesis of Helicobacter pylori infection. Helicobacter. 2009;14:15–20. doi:10.1111/j.1523-5378.2009.00702.x19712163
- Malfertheiner P, Megraud F, O’Morain C, et al. Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut. 2007;56(6):772–781. doi:10.1136/gut.2006.10163417170018
- Mégraud F, Lamouliatte H. Helicobacter pylori and duodenal ulcer. Dig Dis Sci. 1992;37(5):769–772. doi:10.1007/bf012964371563322
- Chan FK, Sung JJ, Chung SS, et al. Randomised trial of eradication of Helicobacter pylori before non-steroidal anti-inflammatory drug therapy to prevent peptic ulcers. Lancet. 1997;350(9083):975–979. doi:10.1016/S0140-6736(97)04523-69329511
- Borody TJ, Brandl S, Andrews P, Jankiewicz E, Ostapowicz N. Helicobacter pylori-negative gastric ulcer. Am J Gastroenterol. 1992;87(10).
- Graham DY, Go MF. Helicobacter pylori: current status. Gastroenterology. 1993;105(1):279–282. doi:10.1016/0016-5085(93)90038-e8514046
- Segal E, Cha J, Lo J, Falkow S, Tompkins L. Altered states: involvement of phosphorylated CagA in the induction of host cellular growth changes by Helicobacter pylori. Proc Natl Acad Sci. 1999;96(25):14559–14564. doi:10.1073/pnas.96.25.1455910588744
- Olbe L, Hamlet A, Dalenback J, Fandriks L. A mechanism by which Helicobacter pylori infection of the antrum contributes to the development of duodenal ulcer. Gastroenterology. 1996;110(5):1386–1394. doi:10.1053/gast.1996.v110.pm86130428613042
- Carrick J, Lee A, Hazell S, Ralston M, Daskalopoulos G. Campylobacter pylori, duodenal ulcer, and gastric metaplasia: possible role of functional heterotopic tissue in ulcerogenesis. Gut. 1989;30(6):790–797. doi:10.1136/gut.30.6.7902753403
- Kate V, Ananthakrishnan N, Tovey FI. Is Helicobacter pylori infection the primary cause of duodenal ulceration or a secondary factor? A review of the evidence. Gastroenterol Res Pract. 2013;2013. doi:10.1155/2013/425840
- Hobsley M, Tovey FI, Holton J. Controversies in the Helicobacter pylori/duodenal ulcer story. Trans R Soc Trop Med Hyg. 2008;102(12):1171–1175. doi:10.1016/j.trstmh.2008.04.03518589464
- Tanih N, Ndip L, Clarke A, Ndip R. An overview of pathogenesis and epidemiology of Helicobacter pylori infection. Afr J Microbiol Res. 2010;4(6):426–436.
- Graham DY, Yamaoka Y. H. pylori and cagA: relationships with gastric cancer, duodenal ulcer, and reflux esophagitis and its complications. Helicobacter. 1998;3(3):145–151.9731983
- Escobar MA, Ladd AP, Grosfeld JL, et al. Duodenal atresia and stenosis: long-term follow-up over 30 years. J Pediatr Surg. 2004;39(6):867–871. doi:10.1016/j.jpedsurg.2004.02.02515185215
- Cekin AH, Taskoparan M, Duman A, et al. The role of Helicobacter pylori and NSAIDs in the pathogenesis of uncomplicated duodenal ulcer. Gastroenterol Res Pract. 2012;2012. doi:10.1155/2012/585674
- Nomura A, Stemmermann GN, Chyou P-H, Perez-Perez GI, Blaser MJ. Helicobacter pylori infection and the risk for duodenal and gastric ulceration. Ann Intern Med. 1994;120(12):977–981. doi:10.7326/0003-4819-120-12-199406150-000017741826
- Patchett S, Beattie S, Leen E, Keane C, O’Morain C. Helicobacter pylori and duodenal ulcer recurrence. Am J Gastroenterol. 1992;87(1).
- Van Zanten SV, Sherman PM. Helicobacter pylori infection as a cause of gastritis, duodenal ulcer, gastric cancer and nonulcer dyspepsia: a systematic overview. Can Med Assoc J. 1994;150(2):177.8287340
- Gdalevich M, Cohen D, Ashkenazi I, Mimouni D, Shpilberg O, Kark JD. Helicobacter pylori infection and subsequent peptic duodenal disease among young adults. Int J Epidemiol. 2000;29(3):592–595.10869336
- Reinbach D, Cruickshank G, McColl K. Acute perforated duodenal ulcer is not associated with Helicobacter pylori infection. Gut. 1993;34(10):1344–1347. doi:10.1136/gut.34.10.13448244099
- Ng E, Chung S, Sung J, et al. High prevalence of Helicobacter pylori infection in duodenal ulcer perforations not caused by non-steroidal anti-inflammatory drugs. Br J Surg. 1996;83(12):1779–1781. doi:10.1002/bjs.18008312379038568
- Gisbert J, Blanco M, Mateos J, et al. H. pylori-negative duodenal ulcer prevalence and causes in 774 patients. Dig Dis Sci. 1999;44(11):2295–2302. doi:10.1023/a:102666912359310573377
- Rauws E. Eradication of Helicobacter pylori cures duodenal ulcer disease In: Helicobacter Pylori and Gastroduodenal Pathology. Springer; 1993:347–351.
- Labenz J, Tillenburg B, Peitz U, et al. Helicobacter pylori augments the pH-increasing effect of omeprazole in patients with duodenal ulcer. Gastroenterology. 1996;110(3):725–732. doi:10.1053/gast.1996.v110.pm86088818608881
- Kandulski A, Selgrad M, Malfertheiner P. Helicobacter pylori infection: a clinical overview. Digestive Liver Dis. 2008;40(8):619–626. doi:10.1016/j.dld.2008.02.026
- Rauws E, Tytgat G. Cure of duodenal ulcer associated with eradication of Helicobacter pylori. Lancet. 1990;335(8700):1233–1235. doi:10.1016/0140-6736(90)91301-P1971318
- Moss SF, Calam J. Acid secretion and sensitivity to gastrin in patients with duodenal ulcer: effect of eradication of Helicobacter pylori. Gut. 1993;34(7):888–892. doi:10.1136/gut.34.7.8888344574
- Blaser MJ, Chyou P, Nomura A. Age at establishment of Helicobacter pylori infection and gastric carcinoma, gastric ulcer, and duodenal ulcer risk. Cancer Res. 1995;55(3):562–565.7834625
- Batista SA, Rocha GA, Rocha AM, et al. Higher number of Helicobacter pylori CagA EPIYA C phosphorylation sites increases the risk of gastric cancer, but not duodenal ulcer. BMC Microbiol. 2011;11(1):61. doi:10.1186/1471-2180-11-6121435255
- Hobsley M, Tovey FI, Bardhan KD, Holton J. Does Helicobacter pylori really cause duodenal ulcers? No. Br Med J. 2009;339. doi:10.1136/bmj.b2788
- Chu K-M, Kwok K-F, Law S, Wong K-H. Patients with Helicobacter pylori positive and negative duodenal ulcers have distinct clinical characteristics. World J Gastroenterol. 2005;11(23):3518. doi:10.3748/wjg.v11.i23.351815962366
- Borody TJ, George LL, Brandl S, et al. Helicobacter pylori-negative duodenal ulcer. Am J Gastroenterol. 1991;86(9).
- Kim JG, Graham DY. Helicobacter pylori infection and development of gastric or duodenal ulcer in arthritic patients receiving chronic NSAID therapy. Am J Gastroenterol. 1994;89(2):203–7.8304304
- Hobsley M, Tovey FI, Holton J. Precise role of H pylori in duodenal ulceration. World J Gastroenterol. 2006;12(40):6413. doi:10.3748/wjg.v12.i40.641317072972
- Hobsley M, Tovey F. Helicobacter pylori: the primary cause of duodenal ulceration or a secondary infection? World J Gastroenterol. 2001;7(2):149. doi:10.3748/wjg.v7.i2.14911819753
- Khan MM, Shahzed MN, Jibran M, Rabbani MJ. Frequency of Helicobacter pylori infection in causation of duodenal ulcer perforation. Group. 2009Jan 1;1(19/116):16–37
- Lario S, Ramirez-Lazaro MJ, Aransay AM, Lozano JJ, Montserrat A, Junquera F, Alvarez J, Segura F, Campo R, Calvet X. microRNA profiling in duodenal ulcer disease caused by Helicobacter pylori infection in a western population. Clinical microbiology and infection. 2012 Aug;18(8):E273–82.22524533