
Abstract
Objectives
Pressure ulcer (PU) treatment poses significant clinical and economic challenges to health-care systems. The aim of this study was to assess the cost-effectiveness and budget impact of enzymatic debridement with clostridial collagenase ointment (CCO) compared with autolytic debridement with medicinal honey (MH) for PU treatment from a US payer/Medicare perspective in the hospital outpatient department setting.
Methods
A cost-effectiveness analysis using a Markov model was developed using a 1-week cycle length across a 1-year time horizon. The three health states were inflammation/senescence, granulation/proliferation (ie, patients achieving 100% granulation), and epithelialization. Data sources included the US Wound Registry, Medicare fee schedules, and other published clinical and cost studies about PU treatment.
Results
In the base case analysis over a 1-year time horizon, CCO was the economically dominant strategy (ie, simultaneously conferring greater benefit at less cost). Patients treated with CCO experienced 22.7 quality-adjusted life weeks (QALWs) at a cost of $6,161 over 1 year, whereas MH patients experienced 21.9 QALWs at a cost of $7,149. Patients treated with CCO achieved 11.5 granulation weeks and 6.0 epithelization weeks compared with 10.6 and 4.4 weeks for MH, respectively. The number of clinic visits was 40.1 for CCO vs 43.4 for MH, and the number of debridements was 12.3 for CCO compared with 17.6 for MH. Probabilistic sensitivity analyses determined CCO dominant in 72% of 10,000 iterations and cost-effective in 91%, assuming a benchmark willingness-to-pay threshold of $50,000/quality-adjusted life year ($962/QALW). The budget impact analysis showed that for every 1% of patients shifted from MH to CCO, a cost savings of $9,883 over 1 year for a cohort of 1,000 patients was observed by the payer.
Conclusion
The results of these economic analyses suggest that CCO is a cost-effective, economically dominant alternative to MH in the treatment of patients with PUs in the hospital outpatient department setting.
Introduction
Pressure ulcers (PUs) contribute to significant morbidity and health-care costs among institutionalized patients. The overall prevalence of PUs in US care settings is an estimated 9.3% and is as high as 28.8% among patients in long-term acute care facilities.Citation1 Patients who experience PUs report greater levels of pain,Citation2 lower levels of health-related quality of life,Citation3 and require longer lengths of stay.Citation4 The annual health-care costs attributed to PUs in the US are an estimated $9.1–$11.8 billion.Citation5 The Centers for Medicare and Medicaid Services (CMS) no longer reimburse hospitals for the treatment of hospital-acquired stage III and IV PU.Citation6 Therefore, the added costs of PU treatment (an average of $8,250–$20,311) can create a substantial financial burden for hospitals.Citation7
The National Pressure Ulcer Advisory Panel defines four stages of PUs based on the degree of tissue loss; exposure of subcutaneous fat, bone, tendon, and muscle; and the amount of slough or eschar present.Citation8 The management of PUs requires proper wound bed preparation,Citation9 the selection of appropriate wound dressings to maintain a moist environment, and attention to proper nutrition.Citation10 Wound bed preparation includes debridement, the removal of nonviable and necrotic tissue that impairs the reepithelialization processes necessary for healing.Citation11 Debridement also reduces the bacterial burden of the wound and exposes newer wound margin cells with greater proliferative potentials.Citation11 Debridement may be conducted through sharp, enzymatic, biological, mechanical, or autolytic methods.Citation10 The selection of an appropriate method is guided by wound and patient characteristics as well as clinician and timing considerations.Citation9 Compared with surgical and mechanical debridement, enzymatic and autolytic methods have high degrees of selectivity, are easy to use, and are less painful to patients.Citation9
Clostridial collagenase ointment (CCO) is an enzymatic debridement agent that selectively breaks downs the collagen in the extracellular matrix of necrotic tissue that anchors the tissue to the wound.Citation9 Furthermore, collagenase enhances keratinocyte proliferation and migration, promoting epithelialization and a faster reduction in wound size.Citation9 Economic analyses report that CCO is a cost-effective treatment for PU debridement relative to treatment with autolytic hydrocolloidCitation12 and hydrogelCitation13 dressings.
Medicinal honey (MH) has been used since ancient times for its antibacterial effect, acceleration of tissue growth and wound healing, and reduction of inflammation.Citation14–Citation18 It is thought to act as an autolytic debriding agent,Citation14 though evidence of its effectiveness in this capacity is conflicting.Citation15,Citation16 Cost-effectiveness studies comparing honey to usual care for the treatment of diabetic foot ulcersCitation17 and venous foot ulcersCitation18 yielded inconsistent results. To the authors’ knowledge, no economic analyses have examined the cost-effectiveness of MH relative to CCO for the treatment of PUs.
This study aims to assess the cost-effectiveness and budget impact of enzymatic debridement using CCO compared with autolytic debridement with MH for PU treatment in the hospital outpatient department (HOPD) setting.
Methods
Model design
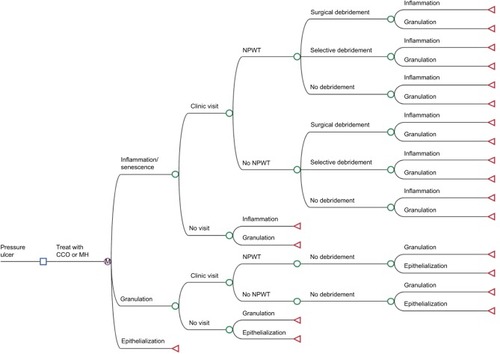
A Markov model was constructed to assess the incremental cost-effectiveness of CCO compared to MH for the treatment of PU. The base case analyses assumed a cohort of adult patients (≥18 years) with PUs treated in a HOPD. The three health states in the model included inflammation/senescence, granulation/proliferation (patients achieving 100% granulation), and epithelialization (). All patients entered the model in the inflammation/senescence health state and then either could fail to progress clinically (stay in that health state), achieve 100% granulation (transition to the second health state), or achieve epithelialization (absorbing health state) during any of the 1-week cycles (). Patients transitioned to health states in the model in 1-week cycle lengths based on transition probabilities derived from the US Wound Registry (USWR).Citation19 One-week cycle lengths were chosen because treatment for wound care is centered around weekly clinic visits, and physician evaluation and treatment actions emanate from these visits. The model terminated after a time horizon of 1 year or epithelialization (whichever came first). The model was constructed from a US payer perspective and assessed all costs in 2016 US dollars. Outcomes evaluated included total 1-year costs, number of granulation and epithelialization weeks, number of clinic visits and debridements, quality-adjusted life weeks (QALWs), and incremental cost-effectiveness ratios (ICERs). The model, sensitivity analyses, and outcomes were constructed and analyzed in TreeAge Pro 2016 (TreeAge Software, Inc., Williamstown, MA, USA).
Figure 1 Three-state Markov diagram of wound healing.

Figure 2 Schematic representation of the Markov model.
Abbreviations: CCO, clostridial collagenase ointment; MH, medicinal honey; NPWT, negative pressure wound therapy.
Furthermore, the study developed a simple budget impact model to estimate the financial impact of using CCO compared with MH for the treatment of PU over a time horizon of 1 year. The budget impact model can provide clinicians and decision-makers with guidance when selecting the CCO or MH therapeutic approach. A sample population of 1,000 patients was considered.
Health state transition probabilities
Health state transition probabilities were based on the observed rates from an analysis of patients from the USWR.Citation19 The USWR is a nonprofit organization that provides data on outcomes and resource utilization among patients with chronic, hard-to-heal wounds. Data are collected from over 100 hospital-based outpatient clinics in the US and Puerto Rico as part of the CMS Physician Quality Reporting System.Citation20 The USWR analysis used for the transition probabilities in this analysis included 446 CCO-treated patients with at least one encounter record with a PU diagnosis (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] diagnosis codes 707.00–707.07, 707.09, and 707.20–707.25) between January 2007 and December 2012. Patients were matched to the corresponding honey-treated PUs (341 patients). In total, there were 517 PUs in each group, with the majority of PUs being stage III or IV (17% were unstageable or stage II). Patients had at least one encounter with a PU diagnosis after the index PU event and were followed from the index date until either 100% granulation or epithelialization or the end of the study period. CCO users had significantly fewer total clinic visits (9.1 vs 12.6; p<0.001), fewer total selective sharp debridements (2.7 vs 4.4; p<0.001), and fewer PUs receiving negative-pressure wound therapy (NPWT) (29% vs 38%; p=0.002) compared with MH. These results were used to calculate the weekly health state transition probabilities in the model ().
Table 1 Health state transition probabilities
Health state utility values
QALWs were calculated by multiplying the time spent in a given health state (life weeks) by a utility value (a health status score ranging from 0 [death] to 1 [perfect health]). In this model, utility values were obtained from the medical literature.Citation21 Patients with PU entered the model with a baseline utility of 0.36 for the “inflammation/senescence” health state; “granulation/proliferation” health state utility value was 0.68, and for “epithelialization”, it was 0.8. Utilities associated with all health states were applied for the full 1-week the patient remained in the particular health state.
Costs
Our analysis was conducted from the perspective of a US payer/Medicare, and costs were expressed in 2016 US dollars. When the physician only performed evaluation and management (E&M) services, a level 3 established visit was assumed. When the HOPD only performed a clinic visit, the charge for a level 3 established clinic visit was assumed. When the physician performed surgical or selective debridement, an E&M charge was not assumed; the HOPD only billed the same surgical or selective debridement even if they followed that debridement with nonselective (enzymatic) debridement. When the physician performed an E&M service and ordered the HOPD staff to perform either nonselective debridement or NPWT, the level 3 established clinic visit was assumed for the physician and either nonselective debridement or NPWT was assumed for the HOPD. If the physician performed surgical debridement and orderd the HOPD staff to follow with NPWT, surgical debridement was assumed for the physician while both surgical debridement and NPWT were assumed for the HOPD ().
Table 2 Procedure and visit costs, 2016 US dollars
The costs of CCO and MH were only included in the sensitivity analyses because Medicare does not separately reimburse for CCO in the HOPD setting (drugs, dressings, and medical supplies are bundled into the debridement procedure code). CCO costs were calculated using the average wound size (7.8 cm2) from the USWR analysisCitation19 and multiplied by the wholesale acquisition cost ($6.83/g)Citation22 to obtain an estimated weekly cost of $63.75. In a secondary sensitivity analysis, the CCO usage was scaled down weekly to coincide with reduction in the average wound size. This was calculated based on the weighted average of the weekly wound size change for granulated patients and the average weekly change for patients who did not granulate.Citation19,Citation23 The cost for MH was estimated using the density of MH (1.5 g/cm3), wholesale acquisition cost ($0.33/mL),Citation22 and the average wound size, assuming a 0.2-cm-thick application was used to calculate the required amount, in grams, per application. Once-daily application was assumed, the quantity was converted to mL/week required (10.92), and a weekly cost was calculated of $3.60 per week for MH.
Sensitivity analysis
One-way sensitivity analysis was conducted to assess the relative impact of each input parameter on the results of the model. Model parameters and assumptions were varied independently across predetermined ranges. Where available, 95% confidence intervals were used for the ranges.Citation19 Monte Carlo simulation (MCS) of 10,000 iterations was performed to determine the joint uncertainty of model parameters. For each variable in MCS, a triangle distribution was assumed (defined by a likeliest, low, and high value) because the true nature of variance for these variables is not well understood and the triangle distribution (when used appropriately) does not violate the requirements of any variable (ie, costs cannot be less than $0, and probabilities and utilities must lie between 0 and 1). The results of the MCS were plotted on a cost-effectiveness acceptability curve and incremental cost-effectiveness scatterplots.
Results
Base case analysis
Under the base case model assumptions, patients treated with CCO achieved an average of 22.7 QALWs and incurred costs of $6,161 over 1 year. Patients treated with MH achieved an average of 21.9 QALWs, with an average cost of $7,149 (). This suggests CCO is the dominant economic treatment strategy.
Table 3 Base case analysis results
Sensitivity analyses
When a constant cost of therapy based on the initial wound size was incorporated in the model (CCO, $63.75/week; MH $3.60/week), patients treated with CCO incurred costs of $8,177 compared to an average cost of $7,269 for patients treated with MH. When the cost of therapy incorporated a decreasing cost over time based on a weighted average of wound size change over time, CCO again was the dominant economic strategy compared to MH, incurring average total costs of $7,029 compared to average costs of $7,200.
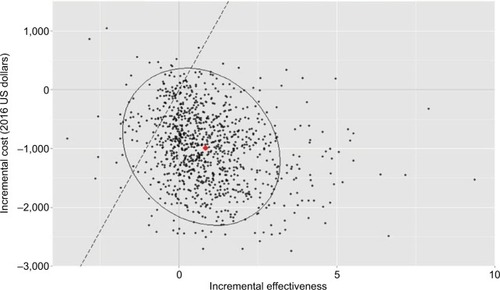
The results of the one-way sensitivity analyses depicted in show that the base case model results were most sensitive to the rate of debridement, the rate of clinic visits, and the probability of granulation, when these inputs were varied independently across a low-to-high range of costs. CCO lost economic dominance (ICER> $0) when MH granulation and clinic visit rates were varied to their lowest values, and when the CCO granulation rates were varied to their highest values. Results of the MCS suggested that CCO would be the dominant strategy compared to MH in 91% of the 10,000 iterations at a willingness-to-pay threshold of $50,000/quality-adjusted life year (corresponding to $962/QALW) and that it fully dominates MH in 71% of iterations ( and ). Probabilistic sensitivity analysis of the second sensitivity scenario, where CCO/MH costs were incorporated with a decay in usage over time, suggests that CCO would be dominant in 48% of iterations and cost-effective in 74%.
Figure 3 Results of the one-way sensitivity analysis.
Abbreviations: E&M, Evaluation and management; CCO, clostridial collagenase ointment; NPWT, negative-pressure wound therapy; ICE, incremental cost-effectiveness; WTP, willingness-to-pay threshold; MH, medicinal honey; QALWs, quality-adjusted life weeks.
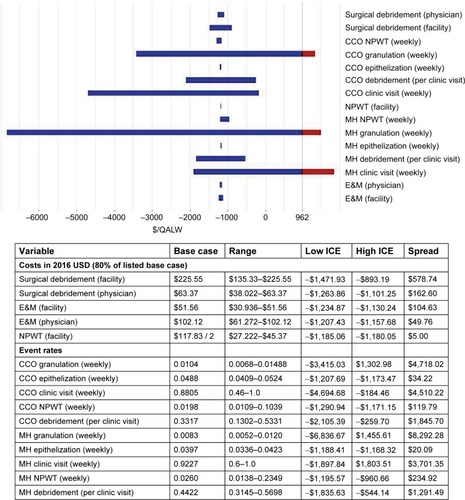
Figure 4 Cost-effectiveness acceptability curve.
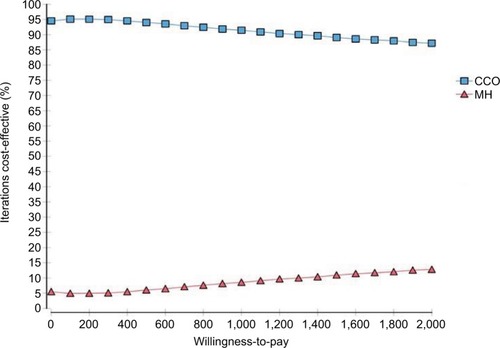
Figure 5 Cost-effectiveness scatterplot.
Abbreviations: WTP, willingness-to-pay; CCO, clostridial collagenase ointment; MCS, Monte Carlo simulation.
Budget impact
A simple budget impact analysis was performed assuming a patient population of 1,000 patients and the same base case scenario as the cost-effectiveness model (where costs of CCO and MH were not included separately because drugs, dressings, and medical supplies are bundled into the debridement procedure code). For every 1% of patients shifted from MH to CCO, there would be a cost savings to the payer of $9,883 over a 1-year horizon. For instance, an initial 20% CCO/80% MH share of patients being shifted to 50%/50% would result in a cost savings of $296,484 over a 1-year period of time.
Discussion
PUs can be difficult-to-treat and slow-to-heal wounds, particularly stages III and IV. These wounds are often treated in a HOPD, where the wound can be evaluated and treated by a group of wound care specialists to stimulate granulation and subsequent epithelialization. In HOPDs, evaluation and management of PUs include wound location, size, tissue type, periwound characteristics, and wound exudate, as well as development of a treatment plan that treats any comorbidities that may affect the patient’s ability to epithelialize. This information alongside periodic assessments allows the HOPD staff to track the progress of the wound throughout therapy and make changes to the treatment plan based on these outcomes. Treatment of PU remains a clinical challenge and, for wounds that do not granulate or epithelialize, can lead to infection and hospitalization. Enzymatic debridement with CCO compared to autolytic debridement with MH has been shown to promote a faster rate of granulation and epi-thelialization,Citation19 although its impact on the risk of infection and hospitalization among patients with slow-to-heal PUs remains to be confirmed.
The evidence available to guide clinicians in regard to debridement approaches for PU is limited and nearly absent for slow-to-heal PUs. Randomized controlled trialsCitation24,Citation25 have shown significant differences between groups treated with CCO vs hydrogel dressings in terms of time required to completely remove necrotic tissue as well as time to epithelialization, both in favor of CCO. One trialCitation26 showed a quantitative difference favoring debridement with CCO compared to another proteolytic enzyme, fibrinolysin/deoxyribonuclease, but the results did not reach statistical significance. Wilcox et alCitation27 demonstrated in a large retrospective analysis of more than 300,000 wounds that faster epithelialization of PUs was generally correlated with more frequent debridement. However, despite the high incidence of PUs, higher level evidence for proper debridement methods is scarce.
In this study, this model assessed the cost-effectiveness of enzymatic debridement with CCO vs autolytic debridement with MH as treatment for PU among patients in the HOPD setting from a US payer’s perspective. At the time of initiating treatment at the HOPD, the average age of these PUs was approximately 6 months, demonstrating the slow-to-heal nature of the wounds being assessed. Overall, the results of the Markov analysis found that CCO was associated with greater quality-adjusted life outcomes (0.84 QALW) at lower total health-care costs than MH (−$988). This economic dominance was robust under a series of sensitivity analyses where input cost and utility estimates were varied. This would result in potential cost savings of $9,883 per percentage point shift from MH to CCO per 1,000 patients.
Results from the sensitivity analysis showed that the weekly rate of debridement and clinic visits were some of the most sensitive model inputs. The adjunctive benefits of debridement and NPWT for treatment of PU are well supported in the literature.Citation28,Citation29 McCallon and FrilotCitation30 found that patients with stage III and IV PU who received both NPWT and CCO reported improved wound outcomes in several Bates-Jensen Wound Assessment Tool categories, particularly in changes in the overall score and the necrotic tissue domain. Additional findings reported that patients with late-stage PU who received NPWT, sharp debridement, and CCO reported an increased rate of granulation and epithelialization compared to NPWT and sharp debridement alone.
Our Markov model is the first to assess the cost-effectiveness of enzymatic debridement with CCO to autolytic debridement with MH. A number of studies have compared enzymatic debridement with CCO to other debridement methods, primarily other autolytic modalities, in terms of both treatment efficacy and cost, and found similar results. Carter et alCitation31 compared the cost of CCO and selective sharp debridement to selective sharp debridement alone for the management of PU using data from the USWR, and found that adding CCO to selective debridement resulted in an ICER of −$375 per ulcer-free week with 17.2 additional ulcer-free weeks and a cost savings of $6,445 per patient over a 2-year period. Waycaster and MilneCitation13 found similar results using data based on a randomized controlled trial in a long-term care setting, where enzymatic debridement with CCO was economically dominant over autolytic debridement with a hydrogel, providing an additional 99 epithelialized wound days and a cost savings of $3,477 over a 1-year period. Using data from a randomized controlled trial in an outpatient setting, Motley et alCitation32 found that CCO and selective sharp debridement compared to selective sharp debridement alone over 1 year yielded eight additional ulcer-free weeks with a cost savings of approximately $300 per patient for the management of diabetic foot ulcers.
The results of our model are promising; however, certain limitations should be considered when interpreting these results. 1) Results cannot be generalized to wounds of other etiologies (ie, diabetic foot ulcers, venous leg ulcers, or other chronic wounds) or other countries because our study uses real-world data from the US. 2) Comparison of other studies may be challenging because the study population is outpatient based rather than inpatient or long-term care. Our study uses real-world data from the USWR, which may be more generalizable to what is happening in the HOPD clinics. In addition, data inputs to the model were derived from relatively small samples. Furthermore, epithelialization rates had to be simplified owing to the high variance in both groups resulting from loss to follow-up in the USWR. 3) Ulcer recurrence rate is not likely to impact any findings,Citation31 and therefore, the model did not incorporate any ulcer recurrence or complications such as infection or hospitalization. 4) Although other adjunctive therapies such as cellular/tissue-derived products and hyperbaric oxygen therapy were similar between groups,Citation19 it is possible that the incidence of other therapies or dressings not captured may have been different. 5) A limitation of the Markov model is that the probability of moving out of a particular health state is not dependent on the states a patient may have experienced prior to entering that specific health state.Citation33 However, with the use of time-dependent transition probabilities, this limitation is minimized. Furthermore, parameter uncertainty was reduced by conducting probabilistic sensitivity analyses. Despite these limitations, the findings for this study provide critical information on the cost-effectiveness of enzymatic debridement with CCO and autolytic debridement with MH in the management of PUs.
Conclusion
Treatment with CCO increases PU patient quality of life and is associated with fewer health-care expenditures over 1 year compared to MH, making CCO the dominant economic strategy. Results of our model suggest, based on input data from the USWR, that a larger proportion of patients treated with CCO achieved epithelialization, had fewer clinic visits and number of debridements, and spent more weeks in granulation. Given the cost savings and added benefit of ulcer-free weeks, health-care providers should consider using CCO over MH for the treatment and management of PUs within the HOPD setting. Future research is warranted to support and expand upon the results found from this model analysis.
Acknowledgments
The authors thank Rich Bizier for assisting with the programming and additional data analyses, and Caroline Fife for providing clinical expertise.
Disclosure
Gilligan, Liang, Limone, Mearns, and Miller, employees of Truven Health Analytics, an IBM Company, received a research contract from Smith & Nephew to conduct this study. Schaum and Waycaster are employees of Smith & Nephew, Inc. The authors report no other conflicts of interest in this work.
References
- VanGliderCLachenbruchCAlgrim-BoyleCMeyerSThe International Pressure Ulcer Prevalence Survey: 2006–2015. A 10-Year Pressure Injury Prevalence and Demographic Trend Analysis by Care SettingJ Wound Ostomy Continence Nurs20174412028
- AhnHStechmillerJFillingimRLyonDGarvanCBodily pain intensity in nursing home residents with pressure ulcers: analysis of national minimum data set 3.0Res Nurs Heal2015383207212
- GoreckiCBrownJMNelsonEAImpact of pressure ulcers on quality of life in older patients: a systematic reviewJ Am Geriatr Soc20095771175118319486198
- WangHNiewcyzkPDiVitaMImpact of pressure ulcers on outcomes in inpatient rehabilitation facilitiesAm J Phys Med Rehabil201493320721624088778
- Agency for Healthcare Research and QualityPreventing Pressure Ulcers in Hospitals Available from: http://www.ahrq.gov/professionals/systems/hospital/pressureulcertoolkit/putool1.htmlAccessed October 20, 2016
- SpectorWDLimcangcoROwensPLSteinerCAMarginal hospital cost of surgery-related hospital-acquired pressure ulcersMed Care201654984585127219637
- KandilovAMCoomerNMDaltonKThe impact of hospital-acquired conditions on medicare program paymentsMedicare Medicaid Res Rev201444E1E23
- BlackJBaharestaniMCuddiganJENational Pressure Ulcer Advisory Panel’s updated pressure ulcer staging systemDermatol Nurs200719434334917874603
- McCallonSKWeirDLantisJCOptimizing wound bed preparation with collagenase enzymatic debridementJ Am Coll Clin Wound Spec201561–2142326442207
- WhitneyJPhillipsLAslamRGuidelines for the treatment of pressure ulcersWound Repair Regen20061466367917199832
- KirshenCPresidentVWooKDebridement: a vital component of wound bed preparationAdv Skin Wound Care200619950651717132956
- MüllerEvan LeenMWBergemannREconomic evaluation of collagenase-containing ointment and hydrocolloid dressing in the treatment of pressure ulcersPharmacoeconomics200119121209121611772156
- WaycasterCMilneCTClinical and economic benefit of enzymatic debridement of pressure ulcers compared to autolytic debridement with a hydrogel dressingJ Med Econ201316797698623701261
- MolanPCPotential of honey in the treatment of wounds and burnsAm J Clin Dermatol200121131911702616
- VandammeLHeynemanAHoeksemaHVerbelenJMonstreySHoney in modern wound care: a systematic reviewBurns2013123981514152523896128
- SimonATraynorKSantosKBlaserGBodeUMolanPMedical honey for wound care – still the “latest resort?”Evid Based Complement Alternat Med20096216517318955301
- MoghazyAMShamsMEAdlyOAThe clinical and cost effectiveness of bee honey dressing in the treatment of diabetic foot ulcersDiabetes Res Clin Pract201089327628120646771
- JullAWalkerNParagVMolanPRodgersARandomized clinical trial of honey-impregnated dressings for venous leg ulcersBr J Surg200895217518218161896
- GilliganAMWaycasterCRBizierRChuBCCarterMJFifeCEComparative effectiveness of clostridial collagenase ointment to medical honey for treatment of pressure ulcers in the hospital outpatient department settingAdv Wound Care201764125134
- Centers for Medicare and Medicaid Services2015Physician Quality Reporting System, 2015 Available from: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Downloads/2015QCDRPosting.pdfAccessed April 1, 2017
- KaitaniTNakagamiGIizakaSCost-utility analysis of an advanced pressure ulcer management protocol followed by trained wound, ostomy, and continence nursesWound Repair Regen201523691592126284460
- Redbook Drug Pricing Database72016Micromedex
- Santyl Dosing Calculator Available from: http://www.santyl.com/hcp/dosing-calculatorAccessed October 8, 2016
- MilneCTCiccareliAOLassyMA comparison of collagenase to hydrogel dressings in wound debridementWounds20102227027425901516
- MilneCTCiccareliAOLassyMA comparison of collagenase to hydrogel dressings in maintenance debridement and wound closureWounds20122431732225876167
- PullenRPoppRVolkersPProspective randomized doubleblind study of the wound-debriding effects of collagenase and fibrinolysin/deoxyribonuclease in pressure ulcersAge Ageing20023112613011937475
- WilcoxJRCarterMJCovingtonSFrequency of debridements and time to heal: a retrospective cohort study of 312 744 woundsJAMA Dermatol20131491050105823884238
- GuptaSBaharestaniMBaranoskiSGuidelines for managing pressure ulcers with negative pressure wound therapyAdv Skin Wound Care2004172 Suppl11615716646
- BaharestaniMde LeonJMendez-EastmanSConsensus statement: a practical guide for managing pressure ulcers with negative pressure wound therapy utilizing vacuum-assisted closure–understanding the treatment algorithmAdv Skin Wound Care200821Suppl 1120
- McCallonSKFrilotCA retrospective study of the effects of clostridial collagenase ointment and negative pressure wound therapy for the treatment of chronic pressure ulcersWounds201527445325786076
- CarterMJGilliganAMWaycasterCRSchaumKFifeCECost effectiveness of adding clostridial collagenase ointment to selective debridement in individuals with stage IV pressure ulcersJ Med Econ201720325326527774840
- MotleyTAGilliganAMLangeDLWaycasterCDickersonJEJrCost effectiveness of clostridial collagenase ointment on wound closure in patients with diabetic foot ulcer: economic analysis of results from a multicenter, randomized, open-label trialJ Foot Ankle Res20158711225653717 ErratumJ Foot Ankle Res201692827493688
- BriggsASculpherMAn introduction to Markov modeling for economic evaluationPharmacoeconomics19981339740910178664