

Abstract
Purpose
Adult growth hormone deficiency (AGHD) is often underdiagnosed and undertreated, leading to costly comorbidities. Previously, we developed an algorithm to identify individuals in a commercially insured US population with high, moderate, or low likelihood of having AGHD. Here, we estimate and compare direct medical costs by likelihood level.
Patients and Methods
Retrospective, observational analysis using the Truven Health MarketScan database to analyze direct medical costs relating to inpatient and outpatient claims, outpatient prescription claims, medication usage, clinical utilization records, and healthcare expenditures. Patients were categorized into groups based on algorithmically determined likelihoods of AGHD. Likelihood groups were further stratified by age and sex. Trajectories of annual costs (USD) by likelihood level were also investigated.
Results
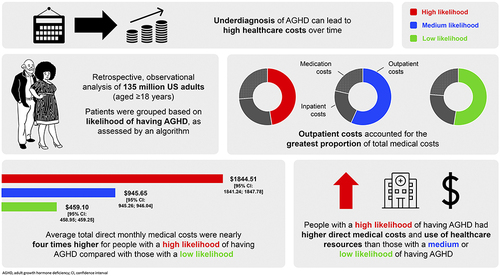
The study cohort comprised 135 million US adults (aged ≥18 years). Individuals ranked as high-likelihood AGHD had a greater burden of comorbid illness, including cardiovascular disease and diabetes, than those ranked moderate- or low-likelihood. Those in the high-likelihood group had greater mean total direct medical monthly costs ($1844.51 [95% confidence interval (CI): 1841.24;1847.78]) than those in the moderate- ($945.65 [95% CI: 945.26;946.04]) and low-likelihood groups ($459.10 [95% CI: 458.95;459.25]). Outpatient visits accounted for the majority of costs overall, although cost per visit was substantially lower than for inpatient services. Costs tended to increase with age and peaked around the time that individuals were assigned a level of AGHD likelihood. Total direct medical costs in individuals with a high likelihood of AGHD exceeded those for individuals with moderate or low likelihood.
Conclusion
Understanding the trajectory of healthcare costs in AGHD may help rationalize allocation of healthcare resources.
Plain Language Summary
Growth hormone is an important substance found in the body. Adult growth hormone deficiency (AGHD) is the reduced production of growth hormone unrelated to the normal reduction seen with aging. Untreated AGHD can result in the development of other conditions, known as comorbidities, which can be expensive to manage.
Previously, 135 million privately insured people in the US, aged 18–64 years, were categorized into groups by their likelihood (high, medium, or low) of having AGHD. This study compared the estimated direct medical costs (eg hospital care and medication) across the different likelihood levels. People with a high likelihood of AGHD had more comorbidities than people with a medium/low likelihood, and an average total direct medical monthly cost of $1844.51, nearly twice as much as those with a medium likelihood ($945.65), and four times as much as those with a low likelihood ($459.10). These costs tended to increase with age, with the highest costs associated with people aged 50–59 years and 60–64 years. Outpatient costs (for treatments not requiring an overnight hospital stay) accounted for the greatest proportion of total medical costs, ahead of inpatient costs (for treatments requiring an overnight hospital stay) and medication costs.
These findings suggest that diagnosing and treating AGHD earlier may help to reduce medical costs over time. Increased testing and treatment will cause an initial increase in the use of healthcare resources, but could improve overall cost effectiveness by reducing the long-term impact of the disease and avoiding unnecessary healthcare use.
Graphical Abstract
Abbreviations
AGHD, Adult Growth Hormone Deficiency; CCI, Charlson Comorbidity Index; CHA2DS2VASc, Score for atrial fibrillation stroke risk; CI, Confidence Interval; DCSI, Diabetes Complications Severity Index; CS, Cushing’s Syndrome; GH, Growth Hormone; SD, Standard Deviation; SMD, Standardized Mean Difference.
Data Sharing Statement
Data are subject to third-party restrictions. The data that support the findings of this study are available from a third party (International Business Machines Corporation). Restrictions apply to the availability of these data, which were used under license for this study. Data can be acquired through licenses from the vendor.
Compliance with Ethics Guidelines
This was a retrospective database study without prospectively enrolled participants. All database records are de-identified and fully compliant with US patient confidentiality requirements, including the Health Insurance Portability and Accountability Act of 1996. The data used for this study did not involve the interaction or interview with any subjects and the data does not include any individually identifiable data and, as such, is not research involving human subjects. Accordingly, ethical approval was not required for this study.
Acknowledgments
Data from the Truven database were supplied by International Business Machines Corporation. Any analysis, interpretation, or conclusion based on these data is solely that of the authors and not of International Business Machines Corporation. The authors thank Teddy Sun and Kai Wai Lee, formerly of Novo Nordisk, for their contributions to early drafts of this manuscript and Navid Nedjatian of Novo Nordisk for his review of and input to the manuscript.
Medical writing and editorial support for the development of this manuscript, under the direction of the authors, were provided by Sonia Vyskocilova, PhD, and Helen Marshall, BA, of Ashfield MedComms, and David Floyd, PhD, on behalf of Ashfield MedComms, funded by Novo Nordisk.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
KCJY has received research grants to the Barrow Neurological Institute from Ascendis, Crinetics, Corcept, Sparrow Pharmaceuticals, and Amryt; served as occasional advisory board member for Novo Nordisk, Ascendis, Ipsen, Amryt, Recordati, Xeris and Crinetics; served as occasional speaker for Novo Nordisk and Recordati. LSB and JMK have nothing to disclose. DRC has acted as a consultant for Novo Nordisk. MFa and JMT are employees and stockholders of Novo Nordisk. ARH has acted as consultant for Ascendis and Novo Nordisk. NK is an employee of Novo Nordisk; and holds stocks in Novo Nordisk and Pfizer. MFl has received research support for her institution from Ascendis; received occasional consulting honoraria from Ascendis, Novo Nordisk, and Pfizer, and is part of the Pituitary Society Board of Directors.