
Abstract
Background
This study examines real-world drug utilization patterns, health care resource use, and costs among patients receiving adjuvant treatment with IFN versus patients receiving no treatment (“observation”) for malignant melanoma following surgery.
Methods
A retrospective cohort study was conducted using administrative claims from Truven Health Analytics (MarketScan®) to identify all adjuvant melanoma patients (aged ≥18 years) diagnosed between June 2007 and June 2011 who had a lymph node dissection (ie, index surgery) and were treated with IFN or subsequently observed. Health care resource use and costs of services were converted to 2012 US dollars and were evaluated and compared using multivariable regression.
Results
Of 1,999 eligible subjects with melanoma surgery claims, 179 (9.0%) were treated with IFN and 1,820 (91.0%) were observed. The median duration (days) and number of doses of IFN therapy were 73 and 36, respectively. Among IFN-treated patients, only 10.6% completed ≥80% of maintenance therapy. The total average cost for patients treated with IFN was US$60,755±$3,972 (n=179); significantly higher than for patients undergoing observation ($31,641±$2,471; P<0.0001). Similar trends were observed when evaluating total cost components, including melanoma-related and non-melanoma–related medical costs. Among the melanoma-related medical costs, outpatient services, including office visits and laboratory testing, represented between 33% and 53% of total costs and demonstrated the largest difference between IFN-treated and observation patients. Outpatient service costs for IFN-treated patients were $32,414±$2,498, over three times greater than those for observation patients ($10,556±$1,128; P<0.0001).
Conclusion
The majority of adjuvant melanoma patients in this study was treated with observation versus IFN treatment. Among those who attempted IFN treatment, most could not complete the recommended course of therapy. Health care costs were significantly greater for patients treated with IFN, with the greatest differences being for melanoma-related medical cost components. These findings illustrate the significant economic burden borne by adjuvant melanoma patients and their health insurers.
Introduction
Over the last decade, the incidence of melanoma has increased faster than that of any other solid tumor.Citation1 Currently, the lifetime risk of developing melanoma is one in 50, and in 2013 nearly 80,000 new cases of melanoma were diagnosed in the USA alone.Citation2 Although early recognition and surgical excision clearly represent the best opportunity for cure, there are also patients who present at more advanced stages.
Patients with thick or ulcerated primary lesions (American Joint Committee on Cancer stage IIB or IIC) and patients with pathological or clinical evidence of regional nodal metastasis (American Joint Committee on Cancer stage III) represent a significant treatment challenge, with a reported 5-year survival rate ranging from 30% to 70%.Citation3 According to US national guidelines, adjuvant therapy is offered to patients with stage IIB, IIC, or III disease who have undergone surgery, consisting exclusively of treatment with IFN-α under different formulations, such as high-dose IFN (HDI) and pegylated IFN. However, according to the National Comprehensive Cancer Network, the impact of adjuvant IFN on overall survival (OS) remains unclear.Citation4 Enrollment in clinical trials and observation are also valid treatment options for patients with stage IIB, IIC, or III melanoma.Citation4 For both physicians and patients, the factors that drive decision making in these cases are complex.
The basis for adjuvant treatment of stage IIB, IIC, or III disease with IFN-α rests on a randomized, multicenter, national trial, E1684, that was conducted by the Eastern Cooperative Oncology Group in 1995 (n=287).Citation5 Data from this trial demonstrated significantly improved relapse-free survival (RFS) and OS with the use of adjuvant HDI in patients with non-metastatic but locally advanced melanoma. Based on these data, the US Food and Drug Administration approved HDI for post-surgical adjuvant treatment of high-risk melanoma patients; however, data in subsequent trials concerning the adjuvant use of IFN-α have been less conclusive. For example, in trial E1690 (n=642), conducted by the same investigators when commercial IFN became available as a post-study drug, HDI did not exhibit a significant OS benefit when compared with observation alone (hazard ratio [HR] =1.0; P=0.995).Citation6 A similar finding was reported when comparing low-dose IFN-α versus observation. Another trial designed to evaluate HDI versus observation for 1 month (E1697; n=1,150) was discontinued at interim analysis due to lack of IFN treatment benefit.Citation7 Conversely, a formal meta-analysis of 18 randomized controlled trials enrolling over 10,000 participants (published between 1995 and 2011) demonstrated that adjuvant IFN was associated with significantly improved disease-free survival (HR =0.83; 95% confidence interval [CI] 0.78–0.87; P<0.00001) and OS (HR =0.91; 95% CI 0.85–0.97; P=0.003).Citation8 As a result, an inconsistent standard of care has emerged, with North American guidelines promoting the use of HDI for stage IIB, IIC, or III disease, while European oncologists and other health care decision-makers have concluded that routine use of IFN cannot be recommended.Citation9,Citation10
In addition to the clinical debate around the use of HDI for stage IIB, IIC, or III melanoma, controversies exist from an economic standpoint. Whereas some investigators have found that adjuvant use of HDI for non-metastatic melanoma is cost-effective, with cost-utility ratios comparable to those for other cancer interventions,Citation11 others have suggested that it may be cost-effective in only the most advanced adjuvant sub-stages.Citation12
Despite these contradictory findings and the substantive debate in the melanoma literature, IFN-α remains an important treatment option for many patients with non-metastatic but locally advanced melanoma in the USA. There are other factors to consider in addition to clinical efficacy, including tolerability and cost. The most prominent acute toxicities of IFN comprise an influenza-like syndrome and include fatigue, depression, and myalgia, among others.Citation13,Citation14
Real-world experience with IFN therapy and its associated costs are increasingly of interest, not only to payers but also to physicians and patients.Citation15 Real-world data can supplement results from randomized clinical trials with additional information on comparative effectiveness, safety, and cost, helping to optimize the management of patients with cancer.Citation16 However, real-world research with IFN therapy in melanoma patients is limited.Citation15 Our study, which builds upon a similar, retrospective, real-world study in this setting,Citation15 used a US-based administrative claims dataset to examine the real-world treatment patterns associated with IFN therapy and to examine health care resource use (HCRU) and direct medical costs among patients receiving adjuvant IFN treatment versus patients receiving no treatment (observation) for non-metastatic but locally advanced malignant melanoma.
Materials and methods
Design and setting
This was a retrospective cohort analysis using the Truven Health MarketScan Claims Data for the period June 1, 2007 to June 30, 2011. The MarketScan database captures person-specific clinical utilization, expenditures, and enrollment across inpatient, outpatient, prescription drug, and carve-out services from a selection of large employers, health plans, and government and public organizations. It links paid claims with encounter data and includes private sector health data from approximately 100 payers. These data represent the medical experience of insured employees and their dependents for active employees, early retirees, Consolidated Omnibus Budget Reconciliation Act continuers, and Medicare-eligible retirees with employer-provided Medicare supplemental plans for approximately 43 million individuals. It also includes inpatient and outpatient diagnoses and procedures as well as retail and mail order prescription records. Available data on prescription records include the National Drug Code and the quantity of the medication dispensed. Charged, allowed, and paid amounts are available for all services rendered, as are dates of service for all claims. Additional data elements include demographic variables (age, sex, and geographic region), product type (eg, health maintenance organization, preferred provider organization), payer type (eg, commercial, self-pay), provider specialty, and eligibility dates related to plan enrollment and participation.
Subjects and treatments
The study identified non-metastatic melanoma patients following local-regional lymph node dissection (ie, non-metastatic, post-surgical lymph node dissection). Since staging information was not available in the database, an operational definition for non-metastatic, post-surgical melanoma was used, with specific inclusion criteria as follows: a) procedure code for melanoma-related surgical intervention (ie, lymph node dissection; ) any time during the identification period between June 1, 2007 and June 30, 2011 (index surgery); b) primary diagnosis based on International Statistical Classification of Diseases, Ninth Revision (ICD-9) diagnosis codes (172.0–172.9 or V10.82) any time during 90 days prior to or after the index surgery; c) age ≥18 years at the time of the index surgery; and d) continuous enrollment for 6 months prior to and 3 months after the index surgery. Patients were excluded if they received systemic chemotherapy during the 180 days prior to or 60 days after the index surgery (ie, lymph node dissection; ), or if they had an ICD-9 diagnosis code for any other primary cancer (140.x-171.x, 174.x-195.x, 199.x, 209.x) on ≥1 inpatient claims ≥2 outpatient visit claims, during the 180 days prior to and including or 60 days after the index date. Patients were also excluded if they had an ICD-9 diagnosis code for any secondary cancer on ≥1 inpatient claims, or ≥2 outpatient visit claims, during the 180-day period prior to and including the index date. This last criterion was not applied if the ICD-9 diagnosis code was for a metastasis involving a site common to melanoma (196.0, 196.3, 196.5) or was unlikely to be associated with another primary cancer ().
Eligible patients with receipt of melanoma-related systemic chemotherapy, defined as a claim for dacarbazine and/or temozolomide and/or paclitaxel and/or carmustine and/or cisplatin and/or carboplatin and/or vinblastine and/or ipilimumab and/or vemurafenib (), beyond 60 days from the index surgery were right censored. Patients were followed until the end of continuous enrollment or the end of the patient data.
The non-metastatic, post-surgical melanoma cohort included all patients identified per the inclusion/exclusion criteria above and constituted the overall study population of non-metastatic, post-surgical melanoma patients. This cohort was sub-classified into two cohorts: a) the IFN cohort: patients with evidence of treatment with IFN within 120 days of the index surgery and b) the non-IFN (observation) cohort: patients without evidence of treatment with IFN within 120 days of the index surgery.
Data analyses
The available IFN claims data were used to assess compliance with established recommendations for IFN treatment. Adjuvant IFN therapy for non-metastatic melanoma is 12 months in duration and consists of induction and maintenance phases. The induction phase requires intravenous administration of IFN five times per week for 4 weeks (20 doses), followed by a maintenance phase consisting of self-administered subcutaneous injections three times per week for 48 weeks (144 doses).Citation13 We implemented a 2-week window to allow for real-world variation in dosing during induction. Consequently, the induction phase was regarded as the first 42 days following initiation of IFN therapy, while days 43–365 were taken to comprise the maintenance phase. Patients were censored before day 365 if they received chemotherapy, lacked continuous enrollment, or were lost to observation.
Treatment patterns with IFN therapy
For patients in the IFN cohort, the duration and frequency of dosing were observed. Based on the frequency of dosing, completion of IFN therapy was defined as receipt of 20 doses intravenously during the induction phase and 144 doses of self-administered subcutaneous injections during the maintenance phase.Citation15 The percentages of patients receiving ≥80% (treatment compliance), ≥50%, and <50% (treatment discontinuation) of the expected 164 doses during the induction and maintenance phases were reported.
Resource utilization and cost
Economic measures of interest included costs associated with the index surgery, follow-up surgeries, IFN therapy, melanoma-related outpatient care, ancillary services, and hospital admissions. Imaging costs were not considered. Additionally, non-melanoma–related costs, such as costs of medications other than IFN and outpatient and inpatient costs without a listed melanoma diagnosis, were considered. Costs were assessed using the amount paid to providers for a claim or health service, including copayment(s) and/or coinsurance, and were reported on a per-patient per-year basis. All costs were expressed in 2012 US dollars and were adjusted using the medical care component of the US Consumer Price Index.Citation17
Melanoma-related (index) surgery resource use and costs included all index surgery, anesthesia, pathology, and hospital care-related claims and associated costs. Follow-up (post-index) surgery resource use costs included all post-index surgery, anesthesia, pathology, and hospital care-related claims and associated costs. IFN therapy resource use and costs included drug costs along with the services required to monitor IFN therapy (complete blood count panels, thyroid-releasing hormone stimulation tests, infusion administrations, and associated office visits). Finally, melanoma-related medical service resource use and costs included outpatient care as well as ancillary/laboratory and radiation therapy services associated with a melanoma ICD-9 diagnosis. A claim was considered to be melanoma-related as long as it was associated with a diagnosis of melanoma regardless of its position (ie, primary diagnosis or not).
Comparison of post-index costs
Aggregate melanoma-related direct medical costs were examined separately for IFN- and non IFN-treated patients. In addition to unadjusted comparisons, generalized linear modeling was employed to assess differences in resource use and costs while controlling for potential confounding factors. Observed data patterns provided guidance as to the selection of model specifications (eg, negative binomial for resource use and gamma for costs). In addition, univariate results provided guidance as to which resource-use and cost measures were modeled. Explanatory variables in the base model included: a) age (18–34, 35–44, 45–54, 55–64, or 65+ years); b) sex; c) plan type (health maintenance organization, preferred provider organization, point of sale, indemnity, or unknown); d) geographic region; e) payer type (commercial, Medicaid, Medicare, self-insured, or other); f) physician specialty; and g) Charlson comorbidity index score.Citation18 Candidate variables were retained in the model if significant (P<0.05) or if there was a strong clinical rationale for their inclusion. The coefficient of determination and scaled deviance were used to assess model goodness of fit. Since patients had variable follow-up, costs were annualized. The annualized cost was calculated as the total cost divided by duration of follow-up with the resulting quotient being extrapolated to a 12-month time horizon.
Results
Patient population
An index surgery event was identified for 76,137 patients (), of whom 5,685 had a confirmed claim for a melanoma diagnosis within 90 days of the index surgery. Additional selection criteria reduced the final cohort for analysis to 1,999 non-metastatic, post-surgical patients. Additional attrition criteria included: 1) age <18 years (n=28); 2) melanoma-related surgical interventions (n=13); 3) evidence of systemic chemotherapy in the pre-index or post-index periods (n=907); 4) evidence of other primary (n=1,068) or secondary (n=285) cancer in the pre-index or post-index periods; 5) patients with IFN treatment 120 days beyond the index surgery (n=46); and 6) patients with capitated data (n=22) (). Of the 1,999 patients who comprised our final cohort, 179 (9.0%) received IFN treatment and 1,820 (91.0%) did not receive adjuvant IFN therapy and were classified as observed. Clinical and demographic characteristics for the IFN and non-IFN cohorts are presented in . The two groups differed significantly with regard to age at first melanoma-related surgery, geographic region, and the presence of cerebrovascular disease prior to index surgery, but not sex, physician specialty at index, other pre-index comorbidities, or comorbidity index score. The number (percent) of patients who received chemotherapy agents during their follow-up period was 18 (10.1%) and 127 (7.0%) in the IFN and non-IFN cohorts, respectively. Mean (standard deviation) follow-up was 738 days (404.8) and 704 days (421.6) in the IFN and non-IFN cohorts, respectively, while median (range) follow-up was 680 days (109–1,780) and 619 days (62–1,825), respectively.
Figure 1 Attrition of sample size, by reason.
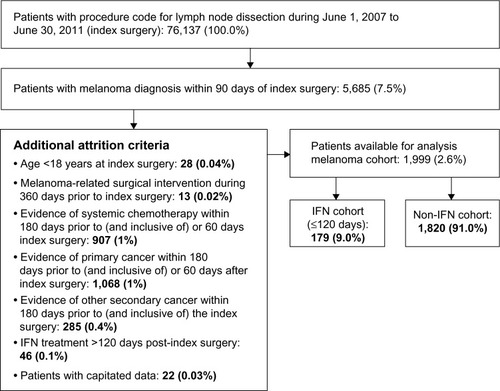
Table 1 Demographic and clinical characteristics
Adjuvant IFN therapy treatment patterns
Of the 179 patients who received adjuvant IFN treatment, only 100 (55.9%) successfully completed the 20-dose induction phase (). Among the 79 patients who did not complete the induction phase, the average (median) duration of follow-up was 591 (537) days. One hundred and ten (61.5%) of the original 179 patients in this IFN cohort went on to receive maintenance dosing. During the maintenance phase, only 19 patients (10.6%) completed at least 80% of the required 144 doses. Among the patients who initiated maintenance treatment, the average (median) duration of follow-up was 718 (627) days. Fifty-one patients (28.5%) discontinued IFN maintenance therapy as indicated by receipt of <50% of the required maintenance dose administrations. Among patients in the IFN cohort, 27.9% were on therapy for 2–29 days, 21.2% for 30–90 days, and 9.5% for 91–180 days. Less than one-third of patients (n=57) continued therapy for between 181 and 365 days. A small minority of IFN-treated patients (5%) had evidence of maintenance therapy lasting beyond 365 days for reasons that could not be explained by the data. The average duration of IFN therapy was 143±136 days, and the average number of completed doses was 57±50 ().
Table 2 Treatment patterns of IFN therapy
Adjuvant IFN therapy HCRU and costs
HCRU and adjusted average treatment costs per melanoma patient per year are reported in for both IFN-treated and observation patients, and include those associated with the index surgery, any follow-up surgeries, and melanoma-related medical care. Total costs are also shown. The total average cost per IFN-treated patient was $60,755±$3,972 (n=179); significantly higher than the total average cost of patients undergoing observation ($31,641±$2,471; P<0.0001). The adjusted ratio of total IFN-related treatment costs to observation-related treatment costs was 1.92. HCRU and medical costs for melanoma-related medical services and non-melanoma medical services were also significantly higher for IFN-treated patients compared to observation patients. Melanoma-related medical costs were $38,730±$4,254 for IFN-treated patients versus $13,995±$2,676 for observation patients (P<0.001), and non-melanoma–related medical costs were $22,415±$12,668 for IFN-treated patients versus $18,442±$13,438 for observation patients (P<0.0001). Costs for outpatient services, including office visits and laboratory testing, comprised 33%–53% of all melanoma-related medical costs and, among all costs, exhibited the greatest difference between IFN-treated and observation patients. Outpatient service costs for IFN-treated patients were $32,414±$2,498 and were over three times greater than those for observation patients ($10,556±$1,128; P<0.0001).
Table 3 Per-patient per-year health care utilization and costsTable Footnotea
Discussion
The objective of our study was to use a US-based administrative claims dataset (Truven Health MarketScan Claims Data; June 1, 2007 to June 30, 2011) to examine real-world treatment patterns associated with IFN therapy as well as to examine HCRU and medical costs among patients receiving adjuvant treatment with IFN versus patients receiving no treatment (observation). Our analysis found that the majority of patients (91.0%) did not receive adjuvant IFN therapy and were instead observed. The rate of IFN use was lower than would be expected for patients with stage II or III disease, and may limit the generality of our findings. Additionally, among patients who did receive IFN treatment, the vast majority were unable to successfully complete either the induction phase (44.1%) or maintenance phase (89.4%) of therapy. Treatment costs were considerably higher for IFN-treated patients, with a total average cost per IFN-treated patient nearly twice the total average cost per observation patient. Melanoma-related medical costs, including office visits and laboratory testing, comprised a significant proportion of total treatment costs for both IFN-treated patients and observation patients. However, these costs were more than three times higher for IFN-treated patients than patients who were not treated with IFN.
Despite conflicting evidence in the clinicalCitation5–Citation8 and economic literature,Citation11,Citation12 there have been relatively few published studies of the real-world patterns of use and costs associated with adjuvant IFN in non-metastatic melanoma patients.Citation15,Citation19,Citation20 A real-world, retrospective, US study by Hackshaw et al using administrative claims described treatment patterns, health care resource utilization, and costs for patients with malignant melanoma diagnosed between 2004 and 2008 who received IFN therapy following surgery.Citation15 In that study, approximately half of patients with malignant melanoma on IFN therapy following surgery did not complete the recommended 1-year treatment course, potentially compromising the full therapeutic benefits of IFN and underscoring an unmet treatment need. For patients to achieve the full clinical and economic benefits of IFN treatment, it is important that they adhere to the recommended therapy regimen. This is especially true for the induction phase; induction is considered an essential element in the treatment schedule because the separation of Kaplan–Meier curves for RFS occurs very early in treatment.Citation21 In our study, fewer than 60% of patients completed the induction phase of treatment according to the predefined criteria. The authors of another study evaluating a 4-week course of IFN therapy, equivalent to the induction phase alone, reported no improvement in RFS (6.8 years vs 7.3 years for observation).Citation7,Citation22 These findings suggest that a longer duration of treatment may be important. In our analysis, approximately 10% of patients completed the maintenance phase of IFN therapy, with an average duration of treatment of 143 days and an average of <60 doses completed. The main reasons for IFN discontinuation, although unknowable in this claim-based analysis, are likely to be related to disease progression and toxicity.Citation5 Possible additional factors contributing to discontinuation may include the inconvenience of infusion administration and frequency of therapy during the induction phase.Citation23 Reasons for discontinuation could not be determined in our study due to the data source used.
Limitations
The results of this research should be interpreted in light of the study design. There are important limitations to be considered when evaluating the results of a retrospective administrative claims database study. Notably, disease stage could not be confirmed due to the absence of staging information in the database. We assumed that receipt of IFN therapy (or observation) and the absence of systemic chemotherapy following lymph node surgery among melanoma patients was representative of regional disease. We were also unable to fully discriminate between sentinel lymph node biopsy and lymph node dissection in this analysis. This last limitation may have led to an oversampling of patients with less advanced disease, limiting the generalizability of the results. That said, a similar approach for identifying adjuvant IFN eligible patients was adopted and published by Hackshaw et al and was shown to be an acceptable method for identifying adjuvant IFN eligible patients given the limitations of claims-based data.Citation15 Furthermore, the rate of IFN use in our study was lower than would be expected, though it was consistent with the findings of Hackshaw et al who reported a prevalence of IFN treatment of 8.4% among 18,075 patients with a confirmed claim of surgery related to melanoma.Citation15 The low apparent rate of IFN treatment can be attributed to the inability to stage patients accurately using claims data. Most surgically resected patients are not candidates for IFN treatment due to being classified with an earlier stage of disease. It is conceivable that the IFN cohort in our study included such patients. Additionally, significant differences in the pre-index characteristics of the IFN and observation cohorts were observed, and these could have contributed in part to the research findings. There was also a lack of congruence between the recommended length of IFN treatment and required duration of follow-up. However, we believe the eligibility criteria that were applied were conservative and that a sensitivity analysis of the inclusion of patients with a minimum of 12 months of follow-up would not be useful due to the expected bias and observed duration of follow-up among most patients.
Choices made in the design of this study affected our ability to assess completion of the induction and maintenance phases of IFN treatment, in a similar manner to the retrospective study by Hackshaw et al.Citation15 Completion of the induction phase was measured as the receipt of ≥20 doses within 42 days after the start of IFN treatment, whereas completion of the maintenance phase was measured as the receipt of ≥144 doses between days 43 and 365 after the start of IFN treatment. Phase completion was assessed among those patients with continuous enrollment. Given that patients were included if IFN treatment was initiated within 120 days of the index surgery, an assessment of the completion of the induction phase required a minimum of 42 and maximum of 162 days of follow-up, while an assessment of the completion of the maintenance phase required a minimum of 365 and maximum of 485 days of follow-up. In spite of the variability in required follow-up, most patients included in the IFN cohort were followed for a sufficient period of time to assess completion of the induction and maintenance phases. Among the 179 patients included in the IFN cohort, 79 did not complete the induction phase, and among these the average (median) duration of follow-up was 591 (537) days. Similarly, 110 of the 179 patients included in the IFN cohort started the maintenance phase, and among these the average (median) duration of follow-up was 718 (627) days.
Assumptions were also made in our study about medication compliance and completion rates, particularly during the self-administered maintenance phase of IFN therapy. Because the induction phase required an intravenous infusion, it was safe to assume that medication claims represented actual administration during induction; however for the self-administered maintenance phase, it was necessary to assume that a medication claim for IFN represented a self-administration of the drug. Although this assumption could not be verified, medication claims are commonly used to assess medication compliance in the published literature.Citation24 While the number of IFN doses received was quantified and related to treatment discontinuation, analyses of IFN dose (ie, units received) were not performed. Finally, costs were measured in our study using amounts paid to providers. Actual costs may have been lower than the reimbursement rates used in our research. It is not known whether any of the patients who contributed data to our study were participating in a clinical trial. If so, then it is possible that participation in a sponsored clinical trial impacted the patient’s claims history, resulting in fewer claims and/or lower costs.
Conclusion
This retrospective cohort study shows that the majority of adjuvant melanoma patients were treated with observation (vs IFN treatment). Among those patients who attempted IFN treatment, most were unable to complete the induction or maintenance phases, which may have limited the clinical effectiveness of their therapy.Citation15 Additionally, total health care costs were significantly greater for patients treated with IFN than for those who were not treated with IFN. These results, which may have implications for payers/decision-makers, suggest a need to consider the implications of adjuvant treatment selection following index surgery and provide information about the costs associated with IFN therapy. Future studies are needed that combine claims and electronic databases, thereby allowing more accurate staging and elimination of contamination of the IFN cohort with patients with less severe disease.
Acknowledgments
The authors wish to acknowledge Dr Cyril Konto, Global Clinical Research, Bristol-Myers Squibb, and Dr David Battleman, TrueNorth Lifesciences, for their significant contributions to the development and execution of the research and review of the corresponding manuscript. Professional editorial support was provided by Lisa Sullivan and Matthew Dougherty at StemScientific.
Supplementary materials
Table S1 Identification codes for data analysis
Table S2 Improbable sites of lymph node metastasis from selected primary cancers
Disclosure
The study was funded by Bristol-Myers Squibb. YZ, TKL, JWS, and SK are employees and stockholders of Bristol-Myers Squibb. The authors have no other conflicts of interest in this work.
References
- RigelDSEpidemiology of melanomaSemin Cutan Med Surg201029420420921277533
- SiegelRNaishadhamDJemalACancer statistics, 2013CA Cancer J Clin2013631113023335087
- FrankSJMeyerMInterferon as adjuvant therapy for high-risk melanomaMelanoma Lett19951314
- National Comprehensive Cancer NetworkNCCN Clinical Practice Guidelines in Oncology: MelanomaNational Comprehensive Cancer Network, Version 42011 Available from: http://www.nccn.org/professionals/physician_gls/pdf/melanoma.pdfAccessed October 30, 2014
- KirkwoodJMStrawdermanMHErnstoffMSSmithTJBordenECBlumRHInterferon alfa-2b adjuvant therapy of high-risk resected cutaneous melanoma: the Eastern Cooperative Oncology Group Trial EST 1684J Clin Oncol19961417178558223
- KirkwoodJMIbrahimJGSondakVKHigh- and low-dose interferon alfa-2b in high-risk melanoma: first analysis of intergroup trial E1690/S9111/C9190J Clin Oncol200018122444245810856105
- AgarwalaSSLeeSJFlahertyLERandomized phase III trial of high-dose interferon alfa-2b (HDI) for 4 weeks induction only in patients with intermediate- and high-risk melanoma (Intergroup trial E 1697)J Clin Oncol201129527s
- MocellinSLensMBPasqualiSPilatiPChiarion SileniVInterferon alpha for the adjuvant treatment of cutaneous melanomaCochrane Database Syst Rev20136CD00895523775773
- PuntCJEggermontAMAdjuvant interferon-α for melanoma revisited: news from old and new studiesAnn Oncol200112121663166611843241
- DummerRHauschildAGuggenheimMKeilholzUPentheroudakisGESMO Guidelines Working GroupCutaneous melanoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-upAnn Oncol201223Suppl 7vii86vii9122997461
- HillnerBEKirkwoodJMAtkinsMBJohnsonERSmithTJEconomic analysis of adjuvant interferon alfa-2b in high-risk melanoma based on projections from Eastern Cooperative Oncology Group 1684J Clin Oncol1997156235123589196150
- CormierJNXingYDingMCost effectiveness of adjuvant interferon in node-positive melanomaJ Clin Oncol200725172442244817557957
- Intron® [product information]Kenilworth, NJSchering-Plough Corporation2009
- KilbridgeKLColeBFKirkwoodJMQuality-of-life-adjusted survival analysis of high-dose adjuvant interferon alpha-2b for high-risk melanoma patients using intergroup clinical trial dataJ Clin Oncol20022051311131811870174
- HackshawMDKrishnaAMauroDJRetrospective US database analysis of drug utilization patterns, health care resource use, and costs associated with adjuvant interferon alfa-2b therapy for treatment of malignant melanoma following surgeryClinicoecon Outcomes Res2012416917622754281
- LymanGHThe evolution of clinical trials in oncology: randomised controlled trials to real world studiesAnn Oncol201425Supplement 4iv41iv42
- US Bureau of Labor Statistics [homepage on the Internet]Consumer price index2001 Available from: http://www.bls.gov/cpi/Accessed February, 2012
- DeyoRACherkinDCCiolMAAdapting a clinical comorbidity index for use with ICD-9-CM administrative databasesJ Clin Epidemiol19924566136191607900
- DavisKLMitraDKotapatiSIbrahimRWolchokJDDirect economic burden of high-risk and metastatic melanoma in the elderly: evidence from the SEER-Medicare linked databaseAppl Health Econ Health Policy200971314119558193
- KotapatiSDavisKLMitraDIloejeUTreatment patterns in high risk and metastatic melanoma: Evidence from linked electronic medical records and administrative claims dataJ Clin Oncol200826Suppl Abstr 17540
- KeffordRFAdjuvant therapy of cutaneous melanoma: the interferon debateAnn Oncol200314335836512598338
- PayneMJArgyropoulouKLoriganPPhase II pilot study of intravenous high-dose interferon with or without maintenance treatment in melanoma at high risk of recurrenceJ Clin Oncol201432318519024344211
- KirkwoodJMBenderCAgarwalaSMechanisms and management of toxicities associated with high-dose interferon alfa-2b therapyJ Clin Oncol200220173703371812202672
- LehmannAAslaniPAhmedRAssessing medication adherence: options to considerInt J Clin Pharm2014361556924166659