
Abstract
A 49-year-old Korean male patient with dementia was diagnosed with probable early-onset Alzheimer’s disease (AD). He presented with memory problems, personality changes, and disorientation. His family history of dementia was probably negative, since no family member with dementia was found or mentioned. Mild cortical atrophy was observed upon magnetic resonance imaging analyses of his brain, and the single-photon emission computed tomography analysis revealed hypoperfusion in the frontal, temporal, and limbic lobes. The patient was tested for mutations in APP, PSEN1, PSEN2, PGRN, MAPT, and PRNP genes. Genetic analysis revealed R62C mutation in PSEN2 gene. PSEN2 R62C mutation was previously reported in European populations, including Dutch and Belgian families with AD. Herein, we present the first case report of PSEN2 R62C mutation in Asia. PolyPhen-2 and SIFT software analyses predicted this mutation as “possibly damaging”, suggesting its potential involvement with AD. In silico protein structural prediction analyses of PSEN2 R62 and C62 revealed two divergent structures, suggesting that large perturbations of R62C mutation might cause dysfunctions of PSEN2, which may alter the normal amyloid production.
Introduction
Alzheimer’s disease (AD) is a complex neurodegenerative disease, which can be divided into two major forms: early-onset AD (EOAD) and late-onset AD (LOAD) with dividing age of 65 years, respectively. Three dominant causative genes for EOAD are amyloid precursor protein (APP), presenilin-1 (PSEN1), and presenlin-2 (PSEN2). Mutations in these genes could increase the production of amyloid beta (Abeta, Aβ) peptide, resulting in their aggregation and deposition, leading to neuronal toxicity and loss. Five to ten percent of all AD cases under 65 years of age can be categorized as EOAD with an autosomal dominant inheritance pattern (familial EOAD). However, family history of the disease could also be absent in several EOAD patients, in which it could be described as occurring due to de novo mutations.Citation1 Even though majority of pathogenic EOAD mutations (almost 200 mutations) were found in PSEN1, only limited numbers of pathogenic mutations were reported in APP (25 cases) and PSEN2 (14 cases; http://www.alzforum.org/mutations).
Mutations in PSEN2 (ch1 227,058,272–227,083,804) are rare, and majority of the reported cases were from patients of European ancestry.Citation2 Only a few PSEN2 mutations were previously reported in Asia, but emerging recent studies found several novel mutations in Korean and Chinese patients.Citation2–Citation5 Phenotypes in AD patients with PSEN2 mutations were milder than those in with PSEN1 mutations. Additional interesting symptoms were also associated with PSEN2-mutation carriers, including atypical dementia, dementia with Lewy bodies, and frontotemporal dementia (http://www.alzforum.org/mutations). Age of disease onset could range between 45 and 88 years.Citation6
Here, we present the detailed case report of a first Korean EOAD patient with a PSEN2 R62C mutation in Asia. In the two main databases, AD and frontotemporal dementia (FTD) mutation database (http://www.molgen.ua.ac.be/ADMutations/) and Alzgene database http://www.alzforum.org/mutations) database, this mutation was previously reported in patients from Europe with LOAD and “pathogenic nature unclear”.Citation7
Materials and methods
Patient information
A 49-year-old, right-handed man visited our memory clinic in April 2013 with memory complaints, which were noticed in 2011 by the patient and his family members. His memory disturbances were gradually increasing, frequently making him lose his belongings without noticing and exhibiting severe memory loss. Other personality changes appeared, such as forgetting important promises to his friends, easily confusing the detailed “must do-lists” or difficulties in the calculations. Prominent naming impairment combined with hesitation to speak became apparent. Sometimes, he asked other people to repeat their conversations due to his failures in comprehending the talks. Geographic disorientations and visuospatial difficulties were also observed during driving with the family members.
The patient was working as a physical education teacher in a middle school, and showed significant impairments and carried out inappropriate decision making and social functions. He could not manage his work as a teacher, for example, creating tests and making decisions at school. Impairments appeared in his daily life activities, such as mistakes in transferring money through telebanking. He presented abnormal behavioral symptoms with an obsessive personality, for example, being stingy with money and also did not allow anyone to spend his money without prior discussions and permission. Patient did not have any medical disease prior to his cognitive decline, and family history was unremarkable since neither his parents nor his siblings showed any cognitive impairment or dementia so far. However, his 14-year-old daughter was mentally handicapped ().
Figure 1 Family tree of the AD patient with R62C mutation.
Abbreviation: AD, Alzheimer’s disease.
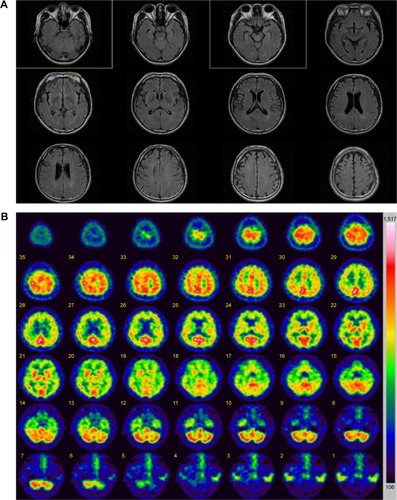
Neurologic examination did not reveal any focal or lateralizing neurologic deficit. Routine laboratory tests, including blood chemistry, electrolyte, and urine analyses, were normal. Serum Venereal Disease Research Laboratory (VDRL) results, including those for Treponema pallidum particle agglutination assay (TPHA), were negative. Thyroid function tests were normal, as with vitamin B12 and folic acid levels. The patient’s apolipoprotein E (APOE) genotype was ε3/ε3. This patient was diagnosed according to the diagnostic criteria for “probable AD” by the National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorder Association, which were ascertained by clinical features, neuropsycho-logical test, and brain magnetic resonance imaging (MRI) imaging with single-photon emission computed tomography (SPECT). Brain MRI revealed mild cortical atrophy without any ischemic change or other lesions (). Brain SPECT showed moderate hypoperfusion in the frontal, limbic, and temporal areas (). The reduced cerebral blood flow from the images of brain SPECT also supported the AD diagnosis.
Figure 2 Imaging data of the patient with PSEN2 R62C.
Abbreviations: MRI, magnetic resonance imaging; SPECT, single-photon emission computed tomography.
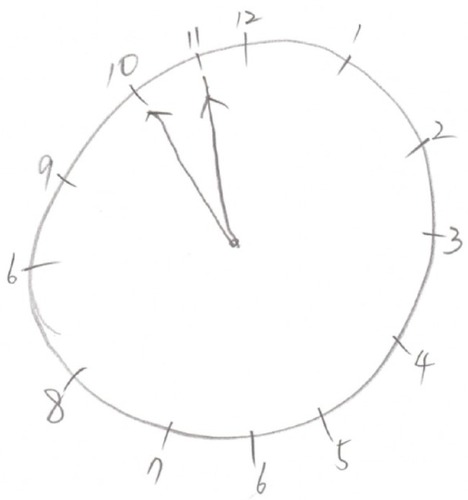
The patient underwent comprehensive neuropsychological tests, and he scored 23 out of 30 (2 percentile) on the mini-mental state examination. The subscores for time orientation and seven-serial calculations were 4 out of 5 and 1 out of 5, respectively. The delayed word recall score was 1 out of 3, and he scored 1 out of 3 in the task of clock drawing (). His score fell in the abnormal range on the attention task of backward digit span (2.5 percentile). Significant impairment appeared in his confrontation naming ability (<0.01 percentile). Performances in copying the intersecting pentagon test and Rey–Osterrieth Complex Figure test were normal, but his performances on clock drawing were severely impaired (5 percentile). On the Seoul verbal learning test, he was able to recall 13 items (0.02 percentile) in three consecutive immediate recall trials, but only 3 items (0.3 percentile) in the 20-minute delayed recall. Poor visual memory score of 10 out of 36 (1 percentile) was obtained in the delayed recall of the Rey–Osterrieth Complex Figure test. He showed abnormal performances in several tasks of frontal and executive functions, especially in the controlled oral word association test, Stroop test, and trail making test.
Figure 3 Clock drawing test.
Patient was diagnosed as probable EOAD, based on clinical assessment, detailed neuropsychological tests, and neuroimaging studies including brain MRI and SPECT.
Genetic screening
Genetic tests were performed in the patient to evaluate possible mutations. We were unable to make segregation analysis, since all family members and relatives refused the genetic test. The patient declined the genetic test for his children too. None of his family members presented any cognitive decline or dementia phenotypes, but they did not agree in releasing other family information. This patient was included in the Clinical Research Center for Dementia of South Korea study, which screened potential causative mutations in 100 patients with EOAD.Citation8 Details of the clinical and scientific analyses of EOAD mutations in the Clinical Research Center for Dementia of South Korea study have not been included previously. A detailed clinical investigation of this patient with detailed personal interview, MRI, SPECT imaging data, and bioinformatic analyses are presented.
Venous blood samples (5 mL) were collected from the patient with an ethylenediaminetetraacetic acid blood drawing tube. Blood sample was centrifuged at 1,500 × g for 5 min, followed by separation of white blood cells (buffy coat) for its storage at −80°C. DNA was purified using GeneAll Blood Protocol kit (GeneAll Biotechnology, Seoul, Korea), and purified DNA was kept at −20°C until the analysis.
A polymerase chain reaction (PCR)-based analysis was performed using primers, as previously described.Citation2 Targeted potential EOAD genes were as following: APP exons 16 and 17, PSEN1, and PSEN2.Citation9–Citation12 Since the diagnosis of EOAD is complicated due to the pathologic overlaps within diverse neurodegenerative disorders, this patient was also screened for progranulin (PGRN), microtubule-associated protein tau (MAPT), and prion (PRNP) genes.Citation13–Citation15
The PCR products were purified using GeneAll Expin PCR kit (GeneAll Biotechnology). Single-strand conformation polymorphism was performed.Citation16 Samples were mixed with formamide and incubated for 10 minutes at 95°C to generate single-stranded DNA bands. For separation, native polyacrylamide electrophoresis (BioRad, Seoul, Korea) was performed for 21 hours. SYBR Gold (Thermo Fisher Scientific, Waltham, MA, USA) staining was used to visualize the DNA bands.
To confirm the mutation, all PCR products were sequenced with the same primer sets in both directions by BioNeer Inc. (Dajeon, Korea). Before sequencing, we purified the PCR products by using GeneAll PCR kit (GeneAll Biotechnology). Big Dye Terminator Cyclic sequencing was performed with the ABI 3730XL DNA Analyzer (http://eng.bioneer.com/home.aspx; BioNeer Inc.). Sequencing data were screened with DNA BASER (http://www.dnabaser.com) software. Sequence variants were identified by NCBI (http://www.ncbi.nlm.nih.gov/gene) and UniProt (http://www.uniprot.org) databases.
Mutations were analyzed by PolyPhen-2 (http://genetics.bwh.harvard.edu/pph2/) online in silico prediction program, which predicted the pathogenic nature of missense mutations. PolyPhen-2 used homology search, multiple sequence alignment, profiling, identity-based scores, and structure-based search parameters (such as accessible surface area and hydrophobicity features). These predictions could define the putative role of missense variants and could predict whether they were probably/possibly damaging or benign. PolyPhen-2 also provided the multiple sequence alignment, which compared the homologous sequences from different organisms. Two types of datasets were used for the prediction: HumDiv and HumVar scores. HumDiv was used for testing the pathogenicty of rare alleles, where mildly damaging variants must be treated as possibly damaging. HumVar was used in case of Mendelian disorders, where more damaging alleles should be distinguished from the less damaging ones.Citation17
We also analyzed the mutation with SIFT algorithm (http://sift.jcvi.org/), which used several databases such as SWISS-PROT, SWISS-PROT/TrEMBL, and NCBI Protein Database. The software analyzed the possibility on the pathogenic properties of mutations by comparing the mutant and normal variants. SIFT scores of point mutation were calculated for weighting the mutations as possibly damaging allele or tolerated (nondamaging), with a dividing score of 0.05, respectively.Citation18
Protein structure prediction analysis of PSEN2 was performed by Raptor X program at the University of Chicago (http://raptorx.uchicago.edu). Normal PSEN2 was composed of 488 amino acids, starting at 61 residues and continuing till residue 448. The prediction was performed at Raptor X web server for both normal PSEN2 and R62C mutation. Based on PSEN2 information from the UniProt database, R62C mutation belonged to the topological domain, positions 1–87, including the mutation site. Superimposed images were visualized by Discovery studio 3.5 software from Accelrys.Citation19
Results
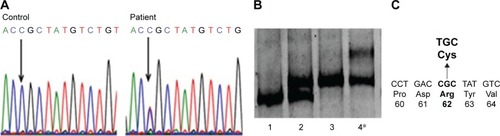
PCR-single-strand conformation polymorphism showed different mobility patterns for this patient’s sample, which suggested the presence of mutation exon 4 of PSEN2 (). Sanger sequencing revealed a heterozygosity of arginine (CGC, Arg, R) to cysteine (TGC, Cys, C) exchange at codon 62, which was previously reported in Europe as possibly a pathogenic variant ().Citation7,Citation20–Citation24 We did not observe any pathogenic mutation in APP, PSEN1, PRNP, PGRN, or MAPT genes.
Figure 4 Genetic analysis of a patient with PSEN2 R62C.
PSEN2 R62C mutation was checked against the Korean Center for Diseases and Controls database (http://www.cdc.go.kr/CDC/contents/), a database of whole genome sequences from 622 healthy control individuals in Korea, but this mutation was not found. Mutation was also checked in the Exome Aggregation Consortium (ExAC) (http://exac.broadinstitute.org/) Browser for reporting all variants from 60,706 unrelated individuals. ExAC was useful for the disease-associated genetic analyses. Frequency of PSEN2 R62C was 0.0001653 (1/10,000–0.001) with heterozygosity only. The previous association studies revealed that this mutation was found in both AD patients and in a few healthy controls.Citation7,Citation21–Citation24
PolyPhen-2 prediction supported the data of Sala Frigerio et al, suggesting PSEN2 R62C as a possibly damaging variant with HumDiv and HumVar scores of 0.877 and 0.513, respectively.Citation22 PolyPhen-2 multiple sequence alignment revealed that R62 might not be conserved among vertebrates. Multiple sequence alignment suggested that PSEN2 sequences of African elephants and giant pandas were similar to human PSEN2, with Arg at the same position. However, in PSEN-like genes of some vertebrate, different amino acids took place of Arg: glycine in Tasmanian devil and short-tailed opossum, threonine in while duckbill platypus, and asparagine in Turkey, respectively. SIFT scores were 0.05, categorizing PSEN2 R62C as a “damaging” variant.
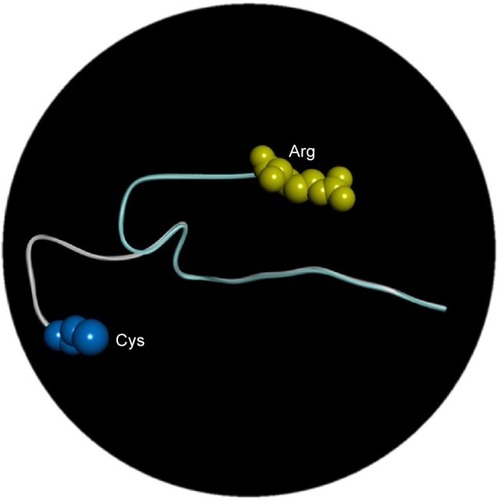
Three-dimensional structure modeling data revealed that PSEN2 1–87 topological domain had an N-terminal loop structure up to residue 71 (), suggesting divergent structures between normal PSEN2 and its mutant R62C. The mutation may not have strong defined structure, but reveals dynamic motion in the loop structure. The highly distinct properties of Arg and Cys could have dramatic impact on the structure and functions of PSEN2. Arg is positively charged with high hydrophilicity and bulk volume, while Cys presents a smaller volume and has a sulfhydryl (-SH) group with negative charge, which can form disulfide bond with other Cys residues inside the PS2 protein or with other proteins. This new SH-bonding potential could result in altered protein functions, which may influence the altered A production.
Figure 5 In silico analysis of PS2 Arg62Cys in three different positions: arginine is labeled with yellow and cysteine with blue.
Discussion
Previously, PSEN2 R62C mutation was reported in LOAD patients and one healthy individual from the Netherlands in Europe.Citation21–Citation24 PSEN2 R62C was also reported in a Caucasian Belgian AD patient with age of onset at 70 years without a detailed clinical report.Citation20,Citation21,Citation23 Sala Frigerio et al detected PSEN2 R62C in one AD patient, whose brother was also diagnosed with AD. Again, no detailed report on the clinical symptoms or disease progression was available, including their age of onset, phenotypes, or genetic testing of their relatives. Hence, the previous reports on PSEN2 R62C did not segregate the relatives of the patients with the disease status.Citation7,Citation21–Citation24
Here, we discovered the same mutation in a Korean male patient with probable EOAD for the first time in Asia. Even though his family did not present with any previous neurologic diseases, this mutation could not be categorized as a probable de novo case, because his family did not agree in revealing any information about their ages nor allowed further genetic testing of siblings and descendants. Hence, we could not completely rule out the possible hereditary traits.
PSEN R62C is located in the N-terminal loop region of PSEN2 protein. Exchange from Arg to Cys could allow PSEN2 to form a disulfide bond with another Cys inside the PSEN2 protein or with other proteins near PSEN2 at cytoplasmic pH (pH 7.2) level. These new SH bonds could have the potential to create novel intermolecular or intramolecular structures that could be involved in pathogenic mechanisms.
At the same locus of PSEN2 R62, another mutation to histidine (His, H) was previously reported with a frequency of 0.009897 (0.001–0.01) in ExAC database. PSEN2 R62H appeared as both homozygous and heterozygous stages, suggesting for the potential of higher number of unaffected individuals and less or no pathogenicity. For H62R, the exchange of Arg to His might not have a dramatic effect on PSEN2, since His and Arg are both positively charged and large amino acids. On the other hand, exchange with Cys could be very different as mentioned in the result. Both PSEN2 R62C and R62H mutations have unclear pathogenicity. Nevertheless, PolyPhen-2 and SIFT analyses suggested that PSEN2 R62C could be more pathogenic than R62H. Both algorithms revealed PSEN2 R62C as possibly damaging, but the R62H was predicted as benign.Citation25 In addition, the ExAC database showed much lower frequency for R62C in unaffected individuals than R62H. Sleegers et al revealed that since both R62C and R62H mutations were rare variants, it would be difficult to perform association study with them; however, they may occur more frequently in patients than in unaffected individuals.Citation21
Guerreiro et al designed an algorithm for classifying PSEN1 and PSEN2 mutations as definitely pathogenic, probably pathogenic, possibly pathogenic, or nonpathogenic groups. If the mutation was found in larger number of patients than controls, it still could be categorized as a “risk factor” or “possibly pathogenic” mutations.Citation26 PSEN2 R62C and R62H are found in higher frequency of patients with dementia than in controls. The measured Aβ levels in the cellular in vitro or in vivo studies of many of the mutations may help in verifying the effect of mutations on increasing Aβ production. PSEN2 R62H mutation did not affect the A production or A 42/40 ratio.Citation27,Citation28 Ertekin-Taner et al examined the correlation of plasma Aβ42 levels between R62C and R62H.Citation7 In this study, a significant association was found between PSEN2 polymorphisms and plasma Aβ42 levels in first-degree relatives with LOAD at a level of 0.03.Citation4 This study was repeated in a large community-based LOAD setting, but no significant association was detected. These findings suggested that even though these PSEN2 mutations might increase the levels of Aβ42 in AD patients, they might not be prominent genetic factors in disease onset. Since the analyses for PSEN2 R62C were not performed thoroughly, the mutational effects on Aβ levels, its metabolism, or altered functions of PSEN2 function cannot be conclusive. In addition, PSEN2 R62C and R62H could be also affected potentially from the gene–environment interactions.Citation7
Besides R62C and R62H, seven missense mutations in the N-terminal region of PSEN2 protein are described in . Majority of them in the N-terminus loop region are categorized as mutations with unclear pathogenicity or nonpathogenic variants. PSEN2 T18M was discovered in a German patient with Parkinson’s disease at 62 years of age, and AD symptoms did not appear until the age of 70 years. No family member was affected with Parkinson’s disease.Citation29 PSEN2 R29H was discovered in one African individual. The functional effect R29H variant remained unknown, but PolyPhen-2 suggested that A29H might have some pathogenic effect.Citation26 PSEN2 G34S was discovered in a Caucasian LOAD patient from the Netherlands, but this mutation did not segregate the family members completely with the disease. PSEN2 G34S did not show clear association with increased Aβ42/Aβ40 ratio.Citation21 PSEN2 P69A was found in a LOAD patient where segregation also could not be assessed, and Dobricic et al suggested that P69A might be a nonpathogenic variant.Citation30 PSEN2 R71W was detected in a LOAD patient without segregation of relatives with the disorder. Previously, PolyPhen-2 predictions suggested that this mutation might be involved in EOAD, but we could not confirm it.Citation21,Citation24,Citation26,Citation31 PSEN2 K82R was found in a Chinese EOAD patient, who presented additional symptoms such as depression and language impairment. She developed memory loss at the age of 53, and family history remained unclear.Citation26 PSEN2 A85V from a Sardinian family was the only pathogenic mutation in the N-terminal region of PSEN2, which was verified from affected family members with AD or dementia with Lewy bodies. The disease usually occurred in 1960s or early 1970s.Citation32
Table 1 Phenotypes of mutations located in the N-terminal region of PSEN2
Conclusion
We discovered a PSEN2 R62C in a male Korean patient with EOAD for the first time in Asia. From the analyses against two major AD databases, AD and FTD mutation databases and the Alzgene databases, PSEN2 R62C was verified as a rare mutation with unclear pathogenic nature, which was similar to the His variant at residue 62, R62H. However, R62C might be involved in pathogenicity, since in silico analyses from PolyPhen-2, SIFT, and three-dimensional modeling suggested pathogenic effects without clear mechanisms. The free SH group in Cys could associate by forming novel disulfide bridge in the loop with nearby proteins or with other sulfurs or metals, leading to altered protein function. Limitation of our study was that we could not make segregation analysis from other family members, since all relatives and family members declined the genetic test, nor revealing other information. Since both PSEN2 R62C and R62H are relatively rare variants in Asia, the association studies may be difficult. Lastly, the functional/cellular studies of these mutations in future could be helpful in verifying their possible roles in AD pathogenicity.
Acknowledgments
Written informed consent for publication of their clinical details and/or clinical images was obtained from the patient.
This work was supported by grants from the Korea Health Technology R&D Project (HI14C3331) through the Korea Health Industry Development Institute (KHIDI), Korea Ministry of Health and Welfare.
Disclosure
The authors report no conflicts of interest in this work.
References
- BagyinszkyEYounYCAnSSKimSThe genetics of Alzheimer’s diseaseClin Interv Aging2014953555124729694
- YounYCBagyinszkyEKimHChoiBOAnSSKimSProbable novel PSEN2 Val214Leu mutation in Alzheimer’s disease supported by structural predictionBMC Neurol20141410524885952
- NiuFYuSZhangZYiXA novel mutation in the PSEN2 gene (N141Y) associated with early-onset autosomal dominant Alzheimer’s disease in a Chinese Han familyNeurobiol Aging201435102420.e1e5
- ShiZWangYLiuSClinical and neuroimaging characterization of Chinese dementia patients with PSEN1 and PSEN2 mutationsDement Geriatr Cogn Disord2015391–2324025323700
- XiaMChenSShiYProbable novel PSEN2 Pro123Leu mutation in a Chinese Han family of Alzheimer’s diseaseNeurobiol Aging201536123334e13e18
- BinettiGSignoriniSSquittiRAtypical dementia associated with a novel presenilin-2 mutationAnn Neurol200354683283614681895
- Ertekin-TanerNYounkinLHYagerDMPlasma amyloid beta protein is elevated in late-onset Alzheimer disease familiesNeurology200870859660617914065
- AnSSParkSABagyinszkyEA genetic screen of the mutations in the Korean patients with early-onset Alzheimer’s diseaseClin Interv Aging2016111817182228008242
- TanziREVaulaGRomanoDMAssessment of amyloid β-protein precursor gene mutations in a large set of familial and sporadic Alzheimer disease casesAm J Hum Genet19925122732821642228
- SchellenbergGDPericak-VanceMAWijsmanEMLinkage analysis of familial Alzheimer disease, using chromosome 21 markersAm J Hum Genet19914835638531998342
- CrutsMvan DuijnCMBackhovensHEstimation of the genetic contribution of presenilin-1 and -2 mutations in a population-based study of presenile Alzheimer diseaseHum Mol Genet19987143519384602
- KamimuraKTanahashiHYamanakaHTakahashiKAsadaTTabiraTFamilial Alzheimer’s disease genes in JapaneseJ Neurol Sci1998160176819804121
- CrutsMGijselinckIvan der ZeeJNull mutations in progranulin cause ubiquitin-positive frontotemporal dementia linked to chromosome 17q21Nature2006442710592092416862115
- RizzuPVan SwietenJCJoosseMHigh prevalence of mutations in the microtubule-associated protein tau in a population study of frontotemporal dementia in the NetherlandsAm J Hum Genet19996424144219973279
- JeongBHJuWKHuhKMolecular analysis of prion protein gene (PRNP) in Korean patients with Creutzfeldt-Jakob diseaseJ Korean Med Sci19981332342409681800
- HayashiKPCR-SSCP: a simple and sensitive method for detection of mutations in the genomic DNAPCR Methods Appl19911134381842918
- AdzhubeiIASchmidtSPeshkinLA method and server for predicting damaging missense mutationsNat Methods20107424824920354512
- NgPCHenikoffSSIFT: predicting amino acid changes that affect protein functionNucleic Acids Res200331133812381412824425
- KällbergMWangHWangSTemplate-based protein structure modeling using the RaptorX web serverNat Protoc2012781511152222814390
- Levy-LahadEWascoWPoorkajPCandidate gene for the chromosome 1 familial Alzheimer’s disease locusScience199526952269739777638622
- SleegersKRoksGTheunsJFamilial clustering and genetic risk for dementia in a genetically isolated Dutch populationBrain2004127Pt 71641164915130954
- Sala FrigerioCLauPTroakesCOn the identification of low allele frequency mosaic mutations in the brains of Alzheimer’s disease patientsAlzheimers Dement201511111265127625937274
- Levy-LahadEWascoWPoorkajPCandidate gene for the chromosome 1 familial Alzheimer’s disease locusScience199526952269739777638622
- BrouwersNSleegersKVan BroeckhovenCMolecular genetics of Alzheimer’s disease: an updateAnn Med200840856258318608129
- CaiYBagyinszkyEAnSSKimSYIn silico modeling of pathogenic or possibly pathogenic point mutations in PSEN2Mol Cell Toxicol2016124453464
- GuerreiroRJBaqueroMBlesaRGenetic screening of Alzheimer’s disease genes in Iberian and African samples yields novel mutations in presenilins and APPNeurobiol Aging201031572573118667258
- WalkerESMartinezMBrunkanALGoateAPresenilin 2 familial Alzheimer’s disease mutations result in partial loss of function and dramatic changes in Abeta 42/40 ratiosJ Neurochem200592229430115663477
- ToMDGokgozNDoyleTGFunctional characterization of novel presenilin-2 variants identified in human breast cancersOncogene200625253557356416474849
- BlauwendraatCWilkeCJansenIEPilot whole-exome sequencing of a German early-onset Alzheimer’s disease cohort reveals a substantial frequency of PSEN2 variantsNeurobiol Aging201637208.e11e17
- DobricicVStefanovaEJankovicMGenetic testing in familial and young-onset Alzheimer’s disease: mutation spectrum in a Serbian cohortNeurobiol Aging20123371481.e7e12
- CruchagaCHallerGChakravertySRare variants in APP, PSEN1 and PSEN2 increase risk for AD in late-onset Alzheimer’s disease familiesPLoS One201272e3103922312439
- PiscopoPMarconGPirasMRA novel PSEN2 mutation associated with a peculiar phenotypeNeurology200870171549155418427071
- ShiZWangYLiuSClinical and neuroimaging characterization of Chinese dementia patients with PSEN1 and PSEN2 mutationsDement Geriatr Cogn Disord2015391–2324025323700