
Abstract
Objectives
Acute kidney injury (AKI) is a common complication in elderly patients and is associated with poor outcomes. However, the effect of transient and persistent geriatric AKI on short-term mortality is unclear. We aimed to study the incidence, clinical characteristics, and prognostic impact of transient and persistent AKI in such patients.
Methods
We retrospectively enrolled very elderly patients (≥75 years) from the geriatric department of the Chinese PLA General Hospital between 2007 and 2015. AKI was defined according to the 2012 Kidney Disease: Improving Global Outcomes criteria. AKI patients were divided into transient or persistent AKI groups based on their renal function at 3 days post-AKI. Renal function recovery was defined as a return to the baseline serum creatinine (SCr) levels.
Results
In total, 668 geriatric patients (39.0%) experienced AKI, and 652 satisfied the inclusion criteria. Of these 652 patients, 270 (41.4%) had transient AKI, and 382 (58.6%) had persistent AKI. The 90-day mortality was 5.9% in patients with transient AKI and 53.1% in patients with persistent AKI. Multivariate analysis revealed that low hemoglobin levels (odds ratio [OR] =0.989; 95% CI: 0.980–0.999; P=0.025), low mean aortic pressure (OR =0.985; 95% CI: 0.971–1.000; P=0.043), peak SCr (OR =1.020; 95% CI: 1.015–1.026; P<0.001) levels, high uric acid (OR =1.002; 95% CI: 1.000–1.003; P=0.040) levels, high blood urea nitrogen (OR =1.028; 95% CI: 1.000–1.056; P=0.047) levels, and mechanical ventilation requirements (OR =1.610; 95% CI: 1.012–2.562; P=0.044) were associated with persistent AKI. Persistent AKI (hazard ratio [HR] =5.741; 95% CI: 3.356–9.822; P<0.001) and more severe AKI stages (stage 2: HR =3.363; 95% CI: 1.973–5.732; P<0.001 and stage 3: HR =4.741; 95% CI: 2.807–8.008; P<0.001) were associated with 90-day mortality.
Conclusion
AKI is common in very elderly patients, with transient renal injury representing close to 42% of all cases of geriatric AKI. More frequent SCr measurements may be helpful for the early diagnosis of transient geriatric AKI. Persistent geriatric AKI is independently associated with a significantly higher risk of 90-day mortality.
Introduction
Acute kidney injury (AKI), which occurs in 23%–40% of elderly patients,Citation1–Citation5 is associated with an increased risk of both chronic kidney disease (CKD) and death.Citation6–Citation9 The key to improving the prognosis of AKI is early diagnosis and early intervention. Nonetheless, AKI diagnosis currently still relies on an increase in serum creatinine (SCr) or a decrease in urine output, which are late markers of impaired renal function.Citation10,Citation11 Delayed AKI diagnosis is probably one of the main reasons for its high morbidity and mortality.Citation12
It should be noted, however, that only a small percentage of AKI patients undergo severe AKI or need dialysis, whereas the majority of AKI patients suffer from milder degrees of renal injury.Citation13,Citation14 The early recognition of AKI is important for preventing or minimizing the associated adverse outcomes.Citation11 However, unfortunately, most general units routinely measure SCr only once or twice a week. This practice may also be a factor in the delay of AKI diagnosis, especially in situations where small changes in SCr occur in elderly people who lack baseline SCr measurements. It is also possible that such impaired renal injury occasionally may be very transient. Therefore, the SCr-based diagnosis of very transient AKI would be missed, underestimating the real incidence of AKI in the very elderly population.Citation15,Citation16
The clinical implications of transient and persistent AKI in very elderly patients are unknown. Therefore, the goals of the present study were to 1) compare the rates of transient and persistent AKI from different AKI stages; 2) address the key clinical differences between transient and persistent AKI; and 3) examine the effect of transient and persistent AKI on short-term mortality.
Materials and methods
This study was conducted at the Geriatric Department of the Chinese PLA General Hospital. The study design was approved by the Clinical Ethics Committee of the Chinese PLA General Hospital, and each patient provided informed written consent. We included all hospitalizations of very elderly patients (≥75 years of age) who were admitted between January 2007 and December 2015. All admissions were screened and evaluated for AKI, categorizing them according to the Kidney Disease Improving Global Outcomes (KDIGO) criteria.Citation10 Exclusion criteria included patients who had been previously diagnosed with CKD,Citation17 stayed in the hospital for <2 days, lacked at least 2 SCr measurements during hospitalization, and had a missing or incomplete medical history.
Definitions
We used the current 2012 KDIGO definition of AKI as the major screening criteria,Citation10 but urine output criteria were not applied. Baseline estimated glomerular filtration rates (eGFRs) were calculated according to the Chronic Kidney Disease Epidemiology Collaboration.Citation18 For baseline SCr, we used the most recent stable measurement during the previous 3 months.Citation4 Peak SCr was the highest SCr reached during the episode. “Transient AKI” was defined as a return to baseline SCr within 3 days post-AKI and “Persistent AKI” was defined as renal dysfunction without recovery within 3 days.Citation19,Citation20
Statistical analysis
Continuous variables are presented as the mean ± SD, or medians (with 25th and 75th percentiles), depending on the variable distribution. Categorical variables are presented as numbers or percentages. Between-group comparisons were made using Student’s t-test or Mann–Whitney U-test for continuous variables and with Pearson’s chi-squared or Fisher’s exact tests for categorical variables. Logistic regression analyses were performed to identify the covariates associated with persistent AKI. Survival curves were estimated by the Kaplan–Meier product-limit method and compared by the Mantel (log-rank) test. Prognostic survival factors were identified using the Cox proportional hazards regression model. A P-value <0.05 indicated statistical significance. Statistical analyses were performed using SPSS version 17.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
Study population
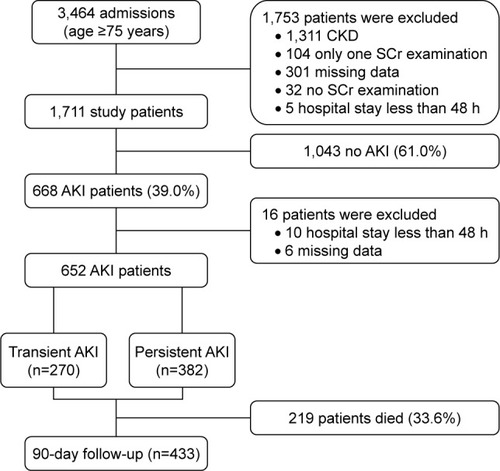
Between January 2007 and December 2015, a total of 3,464 very elderly patients were admitted to the Geriatric Department, and 668 developed AKI during hospitalization. Of these, 10 were excluded for hospital stays <48 h, and six for missing data required for this study, resulting in 652 AKI patients who were suitable for the final evaluation, including 382 (58.6%) patients with persistent AKI and 270 (41.4%) patients with transient AKI. The overall 90-day mortality was 33.6% (219/652). The study flow chart is presented as .
Figure 1 Flow chart of patient inclusion and exclusion.
AKI
Baseline characteristics for all study participants are reported in . There were 652 elderly AKI patients with a median age of 87 (84–91), the majority (623, 95.6%) of whom were male. Among these 652 patients, 308 (47.2%) had stage 1 AKI, 164 (25.2%) had stage 2 AKI, 171 (26.2%) had stage 3 AKI without the need for acute dialysis, and 9 (1.4%) needed dialysis. Oliguria was observed in 35 cases (5.4%).
Table 1 Characteristics of patients with transient and persistent AKI
Clinical characteristics associated with transient and persistent AKI
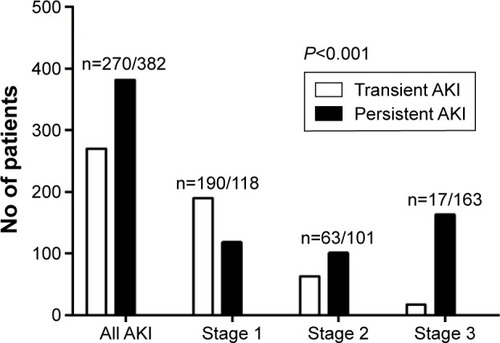
As shown in , comparison of the elderly patients with transient and persistent AKI indicated no significant differences in age (median age: 87 vs 87 years, P=0.400) or body mass index (BMI) (23.3±3.5 kg/m2 vs 22.9±3.0 kg/m2, P=0.149). Similarly, no significant differences were found for preexisting comorbidities (coronary disease P=0.432, hypertension P=0.977, COPD P=0.864, and diabetes mellitus P=0.987) or in baseline renal function (baseline SCr P=0.853 and eGFR P=0.840). Patients with persistent AKI were significantly more likely to be male (97.1% vs 93.3%, P=0.021). Patients with persistent AKI were more frequently treated with mechanical ventilation (MV, 49.0% vs 19.6%, P<0.001), needed dialysis (2.4% vs 0%, P=0.028), and suffered from low mean arterial pressure (MAP, 76±14 mmHg vs 82±14 mmHg, P<0.001) and oliguria (7.6% vs 2.2%, P=0.003). They also had significantly higher SCr (138.0 vs 122.0 μmol/L, P<0.001) and peak SCr (174.3 vs 124.2 μmol/L, P<0.001) levels as well as higher blood urea nitrogen (BUN) (16.2 vs 10.1 mmol/L, P<0.001) and uric acid (393 vs 338.9 μmol/L, P<0.001) levels at the time of AKI diagnosis compared with patients with transient AKI. Low hemoglobin levels (108±23 vs 119±20 g/L, P<0.001), lower prealbumin levels (168 vs 197 g/L, P<0.001), and hypoalbuminemia (33.1±5.4 vs 36.0±5.2 g/L, P<0.001) were more common in patients with persistent AKI. Patients with persistent AKI presented higher mortality rates (53.1% vs 5.9%, P<0.001) and more frequently exhibited stage 2 and 3 AKI (26.4% vs 23.3%, 42.7% vs 6.3%); there were fewer patients with stage 1 AKI 30.9% vs 70.4%; P<0.001; ).
Figure 2 Transient and persistent AKI at different AKI stages in patients with AKI.
Factors associated with persistent AKI
Multivariate logistic regression analysis revealed that persistent AKI was significantly associated with low MAP (odds ratio [OR] =0.985; 95% CI: 0.971–1.000; P=0.043), low hemoglobin levels (OR =0.989; 95% CI: 0.980–0.999; P=0.025), peak SCr levels (OR =1.020; 95% CI: 1.015–1.026; P<0.001), high BUN levels (OR =1.028; 95% CI: 1.000–1.056; P=0.047), high uric acid levels (OR =1.002; 95% CI: 1.000–1.003; P=0.040), and a need for MV (OR =1.610; 95% CI: 1.012–2.562; P=0.044; ).
Table 2 Factors associated with persistent AKI as indicated by logistic regression
Influence of transient or persistent AKI on patient short-term outcomes
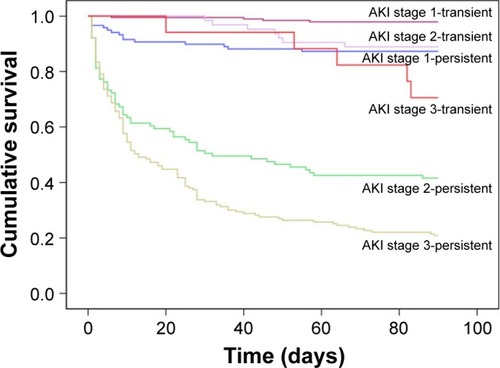
As shown in , the 90-day mortality was 5.9% for patients with transient AKI and 53.1% for patients with persistent AKI (P<0.001). Dialysis was necessary in 2.4% of the persistent AKI patients compared to 0% of the transient AKI (P=0.028) patients. Kaplan–Meier curves showed significant differences in the 90-day mortality between the two groups (log rank P<0.001; ). Within the AKI groups, the 90-day mortality was better in the transient AKI group than in the persistent AKI group (log rank P<0.001; ). The separation of the curves continued throughout the follow-up period, with an increased probability of death during the follow-up with increasing degrees of AKI (). However, in each of the AKI subgroups, the short-term mortality of patients with transient AKI was better than that of patients with persistent AKI. Only patients with transient AKI stage 3 appeared worse than patients with persistent AKI stage 1.
Figure 3 Kaplan–Meier survival curves according to transient and persistent AKI (log-rank test: P<0.001).
Abbreviation: AKI, acute kidney injury.
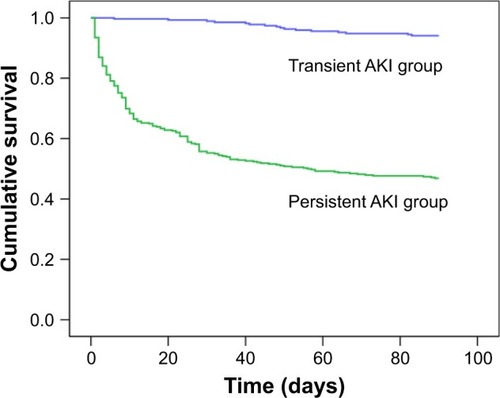
Figure 4 Kaplan–Meier survival curves according to AKI stage (log-rank test: P<0.001).
Of the 652 AKI patients, the 90-day mortality was 33.6% (219/652). Survivors were significantly more likely to have hypertension (77.4% vs 68.5%, P=0.026). BMI (22.2±2.8 vs 23.5±3.3 kg/m2, P<0.001), baseline SCr (64.0 vs 78.0 μmol/L, P<0.001), and baseline eGFR (83.6 mL/min/1.73 m2 vs 76.7 mL/min/1.73 m2, P<0.001) differed significantly between those who died and survived.
As shown in , nonsurvivors were more likely to have required MV and to have had sepsis upon AKI diagnosis than were survivors (65.3% vs 22.4%, 53% vs 33%, respectively; both P<0.001). Oliguria (11.4% vs 2.3%, P<0.001) and low MAP (71±13 vs 82±13 mmHg, P<0.001) were more frequent among nonsurvivors. Likewise, lower prealbumin levels (142 vs 204 g/L, P<0.001), low hemoglobin levels (102±23 vs 118±20 g/L, P<0.001), hypoalbuminemia (31.0±4.9 vs 36.0±5.0 g/L, P<0.001), higher magnesium levels (0.9 vs 0.9 mmol/L, P=0.023), and higher phosphate levels (1.3 vs 1.2 mmol/L, P<0.001) were more frequent in those who died. As expected, the survivors had lower SCr, BUN, uric acid, and peak SCr levels at the time of AKI diagnosis (all P<0.001). Accordingly, the prevalence of persistent AKI was significantly higher in the death group (92.7% vs 41.3%, P<0.001).
Table 3 Comparison of clinical characteristics between elderly AKI survivors and nonsurvivors
also shows the relationship between the AKI stage and short-term outcome; AKI severity was associated with a significantly higher 90-day mortality (8.7% for stage 1 patients, 30.1% for stage 2, and 61.2% for stage 3). Unsurprisingly, outcomes worsened with more advanced AKI stage (P<0.001 for the three stages).
In the multivariate Cox regression analysis, persistent AKI (HR =5.741; 95% CI: 3.356–9.822; P<0.001) and more severe AKI stages (stage 2: HR =3.363; 95% CI: 1.973–5.732; P<0.001 and stage 3: HR =4.741; 95% CI: 2.807–8.008; P<0.001) were associated with the 90-day mortality (). The other independent risk factors for 90-day mortality included BMI, low MAP, low prealbumin levels, infection, oliguria, and BUN levels.
Table 4 Multivariate Cox regression analysis for 90-day mortality
Discussion
We performed a single-center retrospective analysis to describe the epidemiology of AKI and its outcome associations in very elderly patients. Although older people have a high risk to develop AKI, there is no information regarding the incidence and clinical significance of transient versus persistent AKI in such patients. The present study adds interesting information by exploring the relationship between transient and persistent geriatric AKI and short-term mortality. First, nearly 42.0% of the patients with AKI had transient AKI according to the KDIGO criteria. These patients exhibited a temporary decline of renal function and were less likely to have had oliguria and required acute dialysis. Second, geriatric patients with persistent AKI were independently associated with a higher 90-day mortality, and transient AKI was not associated with poorer short-term outcomes. Third, MV affects an elderly patient’s renal function, but does not affect short-term survival. Finally, the outcome of patients with transient AKI stage 3 was worse than that of those with persistent AKI stage 1. This finding further suggests that the distinction between transient and persistent AKI, based on full reversal within 3 days, might be a relevant end point for future studies aiming to improve the ability to predict short-term outcomes.
The first interesting finding from our study is that AKI was diagnosed in 668/1,711 patients (39.0%), and up to 42% of the AKI patients exhibited transient AKI. The higher incidence according to the KDIGO definition primarily resulted from the close monitoring of patients with mild (stage 1) AKI. We thought that this was important because, in contrast to intensive care unit patients, patients in general departments did not have routine daily SCr measurements because many clinicians rely on blood tests as needed and not on a daily basis. The proportion of patients with two or more SCr measurements during hospitalization ranged from 25% to 30% in previous reports.Citation19,Citation21,Citation22 Even for patients with two SCr examinations in 7 days, AKI would be missed in 48% of the patients. Indeed, although the KDIGO criteria provide a 48-hour or 7-day window for diagnosis, these criteria are not commonly used in the real clinical setting. Therefore, some geriatric patients with AKI could be misclassified as not having AKI or, in cases of early AKI, as persistent rather than transient AKI. This could lead to an underestimation of the effect of AKI on mortality, especially in the case of transient AKI. We also divided the AKI patients into transient AKI and persistent AKI groups based on the SCr levels 3 days post-AKI. In contrast, some authors distinguish between transient and persistent AKI based on the differences between admission and discharge SCr values. However, admission SCr values may be affected by the hemodynamics or metabolic status at the time of presentation; thus, it is inappropriate to consider this level as a baseline for renal function for study patients. In elderly patients, various chronic comorbidities and the necessity of prolonged MV can often extend hospital stays. Thus, an evaluation at hospital discharge may also not be an ideal timing.
Several studies that have assessed the prognostic impact of transient changes in renal function during hospitalization show conflicting results.Citation20,Citation23–Citation25 Few studies have evaluated the prognostic impact of transient or persistent AKI in very elderly patients. It has been postulated that transient AKI is not a benign form of AKI that does not reduce mortality. In our study, 42% of hospital-acquired AKI cases were transient. Transiency did not increase the risk of mortality in patients, suggesting that transient geriatric AKI may be a benign form of AKI. In a large multicenter, retrospective study, Uchino et al examined 3,641 AKI patients using the Risk, Injury, Failure, Loss and End-stage Kidney Disease (RIFLE) definition.Citation24 They reported that transient AKI (defined as recovery of renal function to a non-AKI RIFLE category within 3 days after AKI onset) represented 32.1% of all AKI patients, that both transient and persistent AKI were independently associated with a poorer outcomes. The authors also found that patients with persistent AKI had a higher risk of death than did patients with transient AKI. Similarly, Choi et al retrospectively analyzed 2,110 patients who had been diagnosed with acute myocardial infarction, of whom 11% developed AKI (KDIGO criteria); transient AKI (defined as normalization of SCr levels at discharge) occurred in 65% of those with AKI.Citation25 In this study, transient AKI was independently associated with increasing long-term mortality. In contrast, in a study by Perinel et al, which was a retrospective multicenter analysis that included 283 critically ill AKI patients (Acute Kidney Injury Network criteria),Citation20 persistent AKI was defined as nonrecovery within 3 days, and recovery was defined as the absence of oliguria and a return to baseline SCr levels (or a 50% reduction). In this study, 175 patients had persistent AKI, and 108 patients had transient AKI. The authors reported no independent associations between persistent AKI and poor outcomes.
The third interesting finding is the effect of MV on elderly patients. Unlike other studies, we did not find that MV was associated with 90-day mortality,Citation26 but was associated with persistent AKI. First, MV may affect the kidney by causing hemodynamic abnormalities and affecting renal perfusion by decreasing GFR by reducing cardiac output and stimulating hormonal and sympathetic pathways.Citation27 Second, MV through the manipulation of permissive hypercapnia or permissive hypoxemia can lead to renal hypoperfusion, decreased GFR, and functional renal insufficiency.Citation28 Our results also confirmed that patients with persistent AKI had a higher frequency of MV requirements and lower MAP levels compared with patients with transient AKI. The independent risk factors associated with persistent kidney injury were MV and low MAP.
The last interesting finding is in agreement with earlier studies, as we found a graded relationship between AKI severity and mortality.Citation4,Citation29,Citation30 However, for each level of AKI, the outcome of patients with transient AKI stage 3 was worse than that of those with persistent AKI stage 1. This indicates that milder AKI affects patients’ long-term outcomes, while severe AKI affects patients’ short-term outcomes. In addition to the greater susceptibility to AKI, its diagnosis in elderly patients can be difficult or delayed, due to loss of muscle mass, and consequently lower baseline SCr level, masking an increase of its values in kidney injury pathologies, justifying the search for biomarkers of early injury, such as neutrophil gelatinase-associated lipocalin or kidney injury molecule-1.
Consistent with previous studies, we found that high uric acid was associated with persistent AKI.Citation31–Citation34 The plausible explanations were as follows. Uric acid has been linked to AKI via crystal-independent mechanisms, as well as crystal-dependent pathways.Citation32 High uric acid level can cause renal vasoconstriction and impair autoregulation, which results in decreased renal blood flow and GFR.Citation32,Citation33 Sánchez-Lozada et al reported that even a mild elevation of uric acid can induce renal vasoconstriction and persistent glomerular hypertension in rats without evidence of intratubular crystal precipitation.Citation35 In addition, uric acid has been shown to worsen renal function via proinflammatory pathways involving chemokine expression with leukocyte infiltration, as well as proliferation of vascular smooth muscle cells and inhibition of endothelial function.Citation33,Citation34
Interestingly, previous studies reported that being male is one of the most potent risk factors for AKI. However, our multivariate analysis showed that being male was insignificant for predicting persistent AKI in this study. We speculate that this may have been caused by the small number of females in the study. In the next study, we aim to analyze the potent risk factor of being female on AKI mortality in elderly patients.
Conclusion
AKI is common in very elderly patients, and transient renal injury represents close to 42% of all cases of geriatric AKI. More frequent SCr measurements may be helpful for the early diagnosis of transient geriatric AKI. Additionally, persistent geriatric AKI is independently associated with a significantly higher risk of 90-day mortality.
Disclosure
The authors report no conflicts of interest in this work.
References
- ChaoCTLinYFTsaiHBWuVCKoWJAcute kidney injury network staging in geriatric postoperative acute kidney injury patients: shortcomings and improvementsJ Am Coll Surg2013217224025023870218
- ElmistekawyEMcDonaldBHudsonCClinical impact of mild acute kidney injury after cardiac surgeryAnn Thorac Surg201498381582225086946
- ReentsWHilkerMBorgermannJAcute kidney injury after on-pump or off-pump coronary artery bypass grafting in elderly patientsAnn Thorac Surg2014981914 discussion 14–1524881861
- ChaoCTTsaiHBWuCYThe severity of initial acute kidney injury at admission of geriatric patients significantly correlates with subsequent in-hospital complicationsSci Rep201551392526355041
- YokotaLGSampaioBMRochaEBalbiALPonceDAcute kidney injury in elderly intensive care patients from a developing country: clinical features and outcomeInt J Nephrol Renovasc Dis201710273328210101
- PannuNJamesMHemmelgarnBKlarenbachSAlberta Kidney Disease NetworkAssociation between AKI, recovery of renal function, and long-term outcomes after hospital dischargeClin J Am Soc Nephrol20138219420223124779
- ChawlaLSKimmelPLAcute kidney injury and chronic kidney disease: an integrated clinical syndromeKidney Int201282551652422673882
- RewaOBagshawSMAcute kidney injury-epidemiology, outcomes and economicsNat Rev Nephrol201410419320724445744
- NisulaSKaukonenKMVaaraSTFINNAKI Study GroupIncidence, risk factors and 90-day mortality of patients with acute kidney injury in Finnish intensive care units: the FINNAKI studyIntensive Care Med201339342042823291734
- EknoyanGLameireNEckardtKKasiskeBKidney disease: improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injuryKidney Int Suppl201221138
- ChronopoulosACruzDNRoncoCHospital-acquired acute kidney injury in the elderlyNat Rev Nephrology20106314114920125094
- ChaoCTWuVCLaiCFAdvanced age affects the outcome-predictive power of RIFLE classification in geriatric patients with acute kidney injuryKidney Int201282892092722763817
- ThakarCVChristiansonAFreybergRAlmenoffPRenderMLIncidence and outcomes of acute kidney injury in intensive care units: a Veterans Administration studyCrit Care Med20093792552255819602973
- LiborioABLeiteTTNevesFMTelesFBezerraCTAKI complications in critically ill patients: association with mortality rates and RRTClin J Am Soc Nephrol2015101212825376761
- BagshawSMUchinoSCruzDA comparison of observed vs estimated baseline creatinine for determination of RIFLE class in patients with acute kidney injuryNephrol Dial Transplant20092492739274419349297
- MehtaRLTimed and targeted therapy for acute kidney injury: a glimpse of the futureKidney Int2010771194794920467432
- LevinAStevensPESummary of KDIGO 2012 CKD Guideline: behind the scenes, need for guidance, and a framework for moving forwardKidney Int2014851496124284513
- LeveyASStevensLASchmidCHA new equation to estimate glomerular filtration rateAnn Intern Med2009150960461219414839
- XuXNieSLiuZEpidemiology and clinical correlates of AKI in Chinese hospitalized adultsClin J Am Soc Nephrol20151091510151826231194
- PerinelSVincentFLautretteATransient and persistent acute kidney injury and the risk of hospital mortality in critically Ill patients: results of a multicenter cohort studyCrit Care Med2015438e269e27525962084
- YangLXingGWangLAcute kidney injury in China: a cross-sectional surveyLancet2015386100021465147126466051
- LuRMucino-BermejoMJArmignaccoPSurvey of acute kidney injury and related risk factors of mortality in hospitalized patients in a third-level urban hospital of ShanghaiBlood Purif201438214014825471326
- TianJBarrantesFAmoateng-AdjepongYManthousCARapid reversal of acute kidney injury and hospital outcomes: a retrospective cohort studyAm J Kidney Dis200953697498119362401
- UchinoSBellomoRBagshawSMGoldsmithDTransient azotaemia is associated with a high risk of death in hospitalized patientsNephrol Dial Transplant20102561833183920054022
- ChoiJSKimYAKimMJRelation between transient or persistent acute kidney injury and long-term mortality in patients with myocardial infarctionAm J Cardiol20131121414523558040
- Daher EdeFJunior SilvaGBVieiraAPAcute kidney injury in a tropical country: a cohort study of 253 patients in an infectious diseases intensive care unitRev Soc Bras Med Trop2014471868924603743
- KoynerJLMurrayPTMechanical ventilation and the kidneyBlood Purif2010291526819923815
- BrodenCCAcute renal failure and mechanical ventilation: reality or myth?Crit Care Nurse20092926275 quiz 7619339448
- BagshawSMGeorgeCBellomo R; CommitteeADMEarly acute kidney injury and sepsis: a multicentre evaluationCrit Care2008122R4718402655
- HobsonCEYavasSSegalMSAcute kidney injury is associated with increased long-term mortality after cardiothoracic surgeryCirculation2009119182444245319398670
- CheungpasitpornWThongprayoonCHarrisonAMEricksonSBAdmission hyperuricemia increases the risk of acute kidney injury in hospitalized patientsClinical kidney journal201691515626798461
- EjazAADassBKambhampatiGLowering serum uric acid to prevent acute kidney injuryMed Hypotheses201278679679922503466
- LapsiaVJohnsonRJDassBElevated uric acid increases the risk for acute kidney injuryAm J Med20121253302.e309e317
- ShimadaMDassBEjazAAParadigm shift in the role of uric acid in acute kidney injurySemin Nephrol201131545345822000653
- Sanchez-LozadaLGTapiaESantamariaJMild hyperuricemia induces vasoconstriction and maintains glomerular hypertension in normal and remnant kidney ratsKidney Int200567123724715610247