
Abstract
Background
Resistance exercise is effective to increase muscle strength for older adults; however, its effect on the outcome of activities of daily living is often limited. The purpose of this study was to examine whether 3-Step Workout for Life (which combines resistance exercise, functional exercise, and activities of daily living exercise) would be more beneficial than resistance exercise alone.
Methods
A single-blind randomized controlled trial was conducted. Fifty-two inactive, community-dwelling older adults (mean age =73 years) with muscle weakness and difficulty in activities of daily living were randomized to receive 3-Step Workout for Life or resistance exercise only. Participants in the 3-Step Workout for Life Group performed functional movements and selected activities of daily living at home in addition to resistance exercise. Participants in the Resistance Exercise Only Group performed resistance exercise only. Both groups were comparable in exercise intensity (moderate), duration (50–60 minutes each time for 10 weeks), and frequency (three times a week). Assessment of Motor and Process Skills, a standard performance test on activities of daily living, was administered at baseline, postintervention, and 6 months after intervention completion.
Results
At postintervention, the 3-Step Workout for Life Group showed improvement on the outcome measure (mean change from baseline =0.29, P=0.02), but the improvement was not greater than the Resistance Exercise Only Group (group mean difference =0.24, P=0.13). However, the Resistance Exercise Only Group showed a significant decline (mean change from baseline =−0.25, P=0.01) 6 months after the intervention completion. Meanwhile, the superior effect of 3-Step Workout for Life was observed (group mean difference =0.37, P<0.01).
Conclusion
Compared to resistance exercise alone, 3-Step Workout for Life improves the performance of activities of daily living and attenuates the disablement process in older adults.
Introduction
The ability to perform daily activities around the house is fundamental for older adults to take care of themselves and live an independent life. Forty percentage of Medicare enrollees reported limitations in basic activities of daily living or instrumental activities of daily living in 2013, excluding 4% of those living in a long-term care facility.Citation1 Experiencing difficulty in activities of daily living or having to rely on others is a contributing factor to long-term care placement and escalated health care costs.Citation2,Citation3
Late-life disability in activities of daily living is in part correlated with age-related decline in muscle mass and strength.Citation4,Citation5 To improve muscle strength in older adults, resistance exercise is an effective approach.Citation6,Citation7 However, whether resistance exercise is also an effective approach to reducing late-life disability in activities of daily living is not clear.Citation8 The effect of physical exercise on the outcome of activities of daily living reported in the systematic review or meta-analysis studies has been trivial or nonsignificant.Citation8–Citation10 Physical gains in muscle strength do not seem to be fully translated to functional gains in performance of activities of daily living in older adults after resistance exercise.
From the perspective of disablement process,Citation11 age-related loss in muscle mass and strength could be regarded as an impairment of the musculoskeletal system. A significant loss of muscle strength can lead to limitations in movements needed to carry out activities of daily living, such as reaching, lifting, or walking. Limitations in movements then further lead to disability in activities of daily living, such as having difficulty in completing personal care tasks and household management. Accordingly, late-life disability in activities of daily living is a progressive process, starting at the level of impairment, moving to the level of functional limitation, and then the level of disability. Resistance exercise has a strong effect on improving muscle strength, which directly addresses the impairment of the musculoskeletal system, the initial portion of the disablement process, but not the entire process.
Moreover, physical exercise, including resistance exercise, generally consists of structured, repetitive movements and is often performed in a gym-like setting to maximize fitness capacity. The structured and repetitive nature of physical exercise is different from goal-directed nature of activities of daily living that are carried out in a home environment (eg, to get dressed). Because of these dissimilarities, older adults may not connect fitness benefits of exercise with the performance of activities of daily living,Citation12 resulting in a reduced effect of exercise on the outcome of activities of daily living.
According to the principle of training specificity, the closer the training resembles the target task, the larger the improvement in the targeted task performance will be.Citation13 Studies based on this principle have utilized mobility exercise, such as rising from a chair, climbing stairs, and walking,Citation14 or simulated daily tasks, such as carrying a weighted laundry basket and using a vacuum cleaner,Citation15,Citation16 as a task-specific exercise intervention. The training paradigm of task-specific training is more approximate to how people perform daily tasks. Nevertheless, its ecological validity remains limited because training still occurs in a gym-like setting in these studies. Additionally, generalizing the improvement to other untrained daily tasks remains questionable.
To overcome the limitation in physical exercise and intensify the effect on the outcome of actives of daily living for older adults, an intervention program should address the entire disablement process in sequence by: increasing muscle strength first, then integrating the improved muscle strength with movements used to carry out daily tasks, and finally, teaching older adults to associate physical benefits from exercise with task demand at home. In other words, exercise that incorporates task-oriented training might be beneficial for older adults to transform physical gains from exercise to functional performance in activities of daily living. The purpose of this study was to compare such a program, called 3-Step Workout for Life,Citation17 to a non-task-oriented resistance exercise program among older adults who were at risk of losing independence to live in the community. The hypothesis was that 3-Step Workout for Life would be more effective than resistance exercise alone at improving the performance of activities of daily living at intervention completion and 6 months after completion (6-month follow-up).
Method
Study design and participants
A single-blind, randomized controlled trial design was used. The study was approved by the Indiana University Institutional Review Board. Older adults were recruited from local subsidized senior housing communities. Inclusion criteria included: 1) being 60 years old or above; 2) having muscle weakness of the upper or lower extremity; and 3) reporting difficulty in performing one or more basic activities of daily living, which included personal hygiene (bathing, grooming, and oral care), dressing, eating, and transferring or functional mobility. Muscle strength was screened using a Jamar hand dynamometer and the Five Times Sit to Stand Test.Citation18 Muscle weakness was defined as having grip strength of the dominant hand below the age norm,Citation19 or taking more than 13.7 seconds to complete the Five Times Sit to Stand Test. Participants were asked whether he or she had difficulty or required assistance, including the use of assistive devices, completing any self-care tasks at home. Examples of basic activities of daily living were read to them. Exclusion criteria included: 1) showing three or more errors on a six-item cognitive impairment screener;Citation20 2) engaging in any moderate-intensity exercise two or more times per week; 3) receiving rehabilitation services or other intensive medical treatment; 4) reporting any terminal illness, cardiovascular, neurological, psychiatric, or orthopedic impairments that are contraindications to exercise; and 5) planning to move away from the community in 6 months. All participants provided written informed consent.
Baseline measurements included demographic information, body mass index, physical functioning tests, and performance of activities of daily living. Additionally, pain intensity and interference were measured using the PEG 3-item pain scaleCitation21 and the degree of depression was measured using the Patient Health Questionnaire-9.Citation22 After baseline assessments, participants within the same housing community were randomly assigned to the 3-Step Workout for Life Group or the Resistance Exercise Only Group. The study statistician who was not involved in recruitment and assessments generated a randomization allocation list with a block size of 2 or 4. All outcome assessors were blinded to the intervention assignment.
Primary outcome
The primary outcome of activities of daily living was measured by the Motor Skills Scale of the Assessment of Motor and Process Skills (AMPS).Citation23 The AMPS is a standardized observational evaluation of 16 motor skills and 20 process skills when an individual performs familiar activities of daily living. The motor skills are the smallest units of performance that can be observed when a participant interacts with daily objects to complete an activity of daily living. For example, when a participant gets dressed, he or she must reach for, grip, and lift the clothing. Reach, grip, and lift are motor skills in the example. Although the process skills were evaluated together with the motor skills, only the outcomes of motor skills were reported in the current study. The psychometric properties of AMPS have been established in the older adult population.Citation24,Citation25
The AMPS was conducted by two occupational therapists who were calibrated as reliable raters of this instrument. The administration of AMPS started with an interview with each participant to identify two challenging but relevant activities of daily living for the participant to perform. Based on the observation of the performance on the selected activities in each participant’s home, each motor skill was scored using a 4-point ordinal scale ranging from markedly deficient (=1), ineffective (=2), and questionable (=3) to competent performance (=4). These raw ordinal scores were then converted into one logit score ranging from -3 to 4 using the AMPS scoring software. The software utilizes many-facet Rasch analyses to account for the challenge of the selected tasks (item difficulty and person ability) and the severity of the rater.Citation26 In other words, scores can be equated from different AMPS raters, different daily tasks that were performed by different participants, or different daily tasks that were performed at different time point by the same participant.
Secondary outcomes
Physical function of the upper and lower extremity were measured by a graduate research assistant using the Box and Blocks TestCitation27 and Timed Up and Go Test.Citation28 Both measures were conducted in a private community room. During the Box and Blocks Test,Citation27 the participant was seated at a table, facing a rectangular box that was divided into two compartments, one of which was filled with 150 1-inch wide wooden blocks. The filled compartment was first placed on the participant’s dominant side. The participant was asked to move one block at a time from the filled compartment and cross the partition to the other compartment for 60 seconds. Each hand was measured separately. The score was the number of blocks that were moved. The Timed Up and Go Test measured functional mobility.Citation28 The test required the participant to stand up from a chair, walk three meters, turn around, walk back, and sit down. Time was measured in seconds. No physical assistance was given during the test.
Intervention
Detail of the 3-Step Workout for Life program has been described elsewhere.Citation17 In short, an interventionist led and supervised the 3-Step Workout for Life Group three times a week for 10 weeks. The program started with progressive resistance strength exercise in small groups of 4 or 6 in a community room three times a week for 5 weeks. Starting at Week 6, the resistance exercise was reduced to 1 day a week. The program was then blended with one-on-one functional exercise 1 day a week and individualized activities of daily living exercise 1 day a week at each participant’s home. The exercise intensity was kept in the moderate intensity range (somewhat hard or hard) using the Borg-10 Rating of Perceived Exertion.Citation29 Exercise sessions occurred on nonconsecutive days.
Both progressive resistance strength exercise and functional exercise utilized elastic tubing. Participants performed two to three sets of 12 repetitions for each muscle group or movement pattern. Resistance was increased if the participant could complete 12 repetitions with ease. The resistance strength exercise focuses on strengthening nine major muscle groups of the upper and lower extremity that are for weight-bearing and lifting. For example, shoulder flexion and extension, and hip flexion and extension. Functional exercise focuses on eight movement patterns required to perform activities of daily living, such as lifting an object to an overhead shelf or standing up from a chair. Particularly, movement patterns in functional exercise emphasize the coordination among joints and muscles for functional use while continuing muscle building. Additionally, participants were asked to name daily activities in which they would apply a similar movement pattern to perform.
The interventionist worked with each participant to select activities to practice in each activities of daily living exercise training session. The interventionist applied six principles (change of load, change of movement distance, change of movement direction, change of movement speed, change of endurance, and change of activity complexity) to adjust physical challenge of selected activities in which participants experienced difficulty and also activities that were essential for them to stay independent at home. For example, if a participant experienced difficulty to restore pantry items to overhead shelves, the interventionist could have had the participant wear a weighted wrist cuff while sorting pantry items (change of load), restore items to a shoulder-high versus overhead shelf (change of movement distance), restore items into different locations on the shelves (change of movement direction), slow down or speed up while storing items (change of movement speed), store five pantry items versus store 10 items at a time (change of endurance), or carry groceries with a shopping bag and store pantry items from the groceries to the overhead shelves (change of activity complexity by combining two tasks, carrying groceries and sorting the pantry items after shopping). These six principles act as catalysts for integrating muscle strength and movement patterns accrued from progressive resistance strength exercise and functional exercise with task demand within the home environment.
The Resistance Exercise Only Group performed progressive resistance strength exercise three times a week for 10 weeks in small groups. Another interventionist led and supervised the group. The exercise content and intensity were identical to the resistance exercise component in the 3-Step Workout for Life program.
The interventionists had received at least 20 hours of training before the trial started. The interventionist must have a background in exercise sciences or rehabilitation. The interventionists recorded attendance, adverse events, and off-session physical exercise at the beginning of each session. If an off-session exercise lasted longer than 20 minutes, the exercise was logged. Onsite visiting was conducted to ensure intervention fidelity for both intervention groups.
Sample size estimation
Sample size estimation was based on the AMPS Motor Skills, which was the primary outcome. A change of 0.5 logits as a clinically meaningful difference has been reported.Citation30 For a conservative estimation, a 0.4 logits improvement with a standard deviation of 0.4 was assumed. A sample size of 25 per group would result in 80% power with a targeted significance level of 2.5% based on the two-sample t-test. This would also allow for an attrition rate of 15%.
Statistical analysis
To evaluate the effects of the intervention programs at postintervention and 6-month follow-up, a repeated-measures mixed effects model using the constrained longitudinal data analysis was conducted.Citation31 The constrained longitudinal data analysis has great efficiency and flexibility to handle missing data with valid inference when data are missing at random.Citation32,Citation33 Time of measurement (baseline, postintervention, 6-month follow-up), and its interaction with each group (3-Step Workout for Life, Resistance Exercise Only) were included in the model. Time of measurement was treated as a categorical variable to estimate nonlinear time effect. Analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). The significance level was set at the 0.05 level.
Results
A total of 144 residents from seven subsidized senior housing communities were screened for eligibility, and 52 were enrolled and randomized. Eight participants, six in the 3-Step Workout for Life Group and two in the Resistance Exercise Only Group, dropped out of the study. Those who dropped out had fewer chronic conditions (mean =3.25 versus 4.64, P=0.03) and higher AMPS Motor Skills scores than those who did not drop out (mean =1.62 versus 1.09 logits, P<0.01). shows the study flow chart, and shows participant characteristics at baseline.
Table 1 Baseline characteristics
Figure 1 The study CONSORT flow diagram.
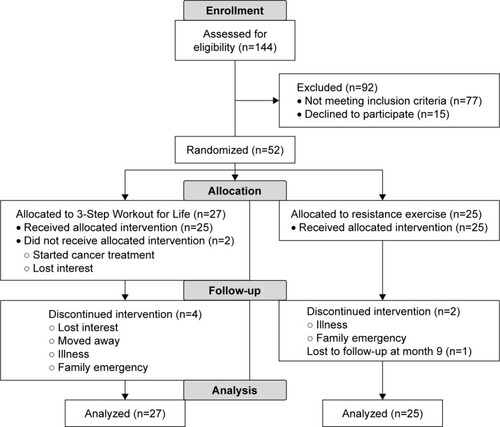
The attendance rate and adverse events in participants who completed the 10-week training were analyzed. The average attendance rate was 95%±5% for the 3-Step Workout for Life Group (n=21) and 90%±8% for the Resistance Exercise Only Group (n=23), t (38.34) =2.49, P<0.05. In total, there were 291 episodes of adverse events in the 3-Step Workout for Life Group (muscle soreness =130; joint pain =122; falls =5; dizziness =9; illness =7; hospitalization =2; other =16), and 512 in the Resistance Exercise Only Group (muscle soreness =204; joint pain =248; falls =7; dizziness =3; illness =9; hospitalization =4; other =37). The data showed a trend of increased number of adverse events in the Resistance Exercise Only Group: median (interquartile range) count =15 (9–17) for the 3-Step Workout for Life Group versus 22 (7–34) for the Resistance Exercise Only Group, P=0.08. Physical exercise logs indicated that activity levels outside the training sessions over the intervention period did not change for both groups.
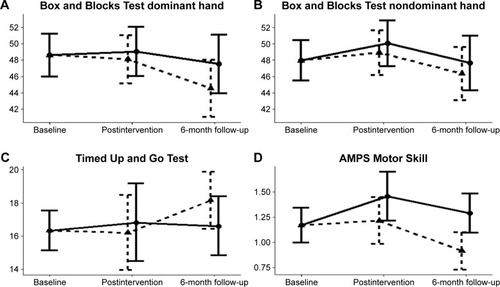
shows estimated changes at postintervention and 6-month follow-up. At postintervention, the 3-Step Workout for Life Group showed a significant improvement from the baseline on the AMPS Motor Skills, mean difference =0.29 logits, P=0.02, while the Resistance Exercise Only Group did not, mean difference =0.04 logits, P=0.71. At the 6-month follow-up, the AMPS Motor Skills score in the 3-Step Workout for Life Group was higher than the baseline; however, the change was not statistically significant, mean difference =0.12 logits, P=0.24. On the contrary, the Resistance Exercise Only Group showed a significant decline from the baseline at the 6-month follow-up, mean difference =3 to 4 using the AMPS scoring software. The 0.25 logits, P=0.01.
Table 2 Comparing mean change from baseline to postintervention and 6-month follow-up
Compared to the baseline, the 3-Step Workout for Life Group did not show a significant change on the Box and Block or Timed Up and Go at either postintervention or 6-month follow-up. The Resistance Exercise Only Group did not show a significant change from the baseline on the Box and Block test or Timed Up and Go at postintervention. However, at the 6-month follow-up, significant declines from the baseline in the Box and Blocks test using the dominant hand, mean difference =3 to 4 using the AMPS scoring software. The 4.05, P=0.02, and Timed Up and Go, mean difference =1.84, P=0.01, were observed in the Resistance Exercise Only Group.
shows the estimated means and 95% confidence intervals of outcome measures at postintervention and 6-month follow-up. After adjusting the differences in baseline, there were no significant group differences in changes from the baseline to postintervention on the Box and Blocks (group mean difference of the dominant hand =0.95, P=0.55; group mean difference of the nondominant hand =1.13, P=0.45), Time Up and Go (group mean difference =0.61, P=0.68), or AMPS Motor Skills (group mean difference =0.24, P=0.13). Similarly, there were no group differences in changes from the baseline to 6-month follow-up on the Box and Blocks (group mean difference of the dominant hand =2.95; P=0.19; group mean difference of the nondominant hand =1.31; P=0.50) or Timed Up and Go (group mean difference =3 to 4 using the AMPS scoring software. The 1.55, P=0.13). However, the 3-Step Workout for Life Group showed a significantly greater performance in the AMPS Motor Skills than the Resistance Exercise Only Group at the 6-month follow-up (group mean difference =0.37, P<0.01).
Figure 2 Estimated means and 95% confidence intervals by outcomes and groups at postintervention and 6-month follow-up.
Abbreviation: AMPS, Assessment of Motor and Process Skills.
Discussion
The main hypothesis of this study is that 3-Step Workout for Life, which addresses the disablement processCitation11 and task-oriented training, would be more effective than resistance exercise alone on improving the performance of activities of daily living in older adults who are at risk of losing independence at home. This hypothesis is partially supported by the results. Although the 3-Step Workout for Life Group showed a significant improvement at postintervention, the improvement was not greater than the Resistance Exercise Only Group. After 6 months of detraining period, however, the 3-Step Workout for Life Group is able to preserve the effect while the effects in the Resistance Exercise Only Group declined significantly. This finding suggests that 3-Step Workout for Life is able to prolong the training effect, which is critical for vulnerable older adults who are inclined to functional decline.
3-Step Workout for Life contains three exercises: progressive resistance strength exercise, functional exercise, and activities of daily living exercises. To disrupt the disablement processCitation11 and help older adults link exercise with the performance of activities of daily living, the three exercises are delivered in a stepwise manner. To our knowledge, this is one of a few exercise programs being structured in this way to maximize the ecological validity. Another similar program is the functional-task exercise program developed by de Vreede et al.Citation34,Citation35 There are three phases in the 12-week functional-task exercise program, practice phase (2 weeks), variation phase (4 weeks), and daily tasks phase (6 weeks). A succeeding phase is built on the prior phase. The program starts with short, simple tasks and then alters the task demand in correspondence to the capability of each participant, such as performing the task as quickly as possible, carrying more weight, or increasing walking distance. de Vreede et alCitation34 found that the functional-task exercise program was more effective than resistance strength exercise at improving functional task performance in healthy community-dwelling elderly women at postintervention. One noticeable difference between de Vreede’s studyCitation34 and this study is that our participants are at risk of becoming frailCitation36 and losing independence at home. Another difference is that the duration in de Vreede’s program is 2 weeks longer than 3-Step Workout for Life, and the proportion of daily tasks training sessions is also higher (18 out of 36 sessions versus 5 out of 30 sessions). Extending the duration of 3-Step Workout for Life or increasing the number of sessions of activities of daily life exercise may augment the effect size on the primary outcome in our study.
The superior effect of 3-Step Workout for Life on the outcome of activities of daily living is observed at the 6-month follow-up. As shown in , the 3-Step Workout for Life Group is able to retain the intervention effect after 6 months of detraining while the intervention effect in the Resistance Exercise Only Group declines below the baseline. The results of Box and Blocks test and Timed Up and Go follow a similar trajectory of decline over the detraining period in the Resistance Exercise Only Group. These findings highlight the limitation of progressive resistance strength exercise. Previous studies in older adults have found that the training effects of resistance exercise are abolished after 6 weeks to 4 months of detraining.Citation37–Citation39 The speed of decline could be steeper in our participants because they had some degree of muscle weakness before entering the trial. To sustain the intervention effect, older adults are recommended to follow a long-term systematic routine of resistance exercise.Citation38 This can be a challenge for older adults in an instance of life event or health problem. A short-term exercise regimen that can induce prolonged training effect is favorable to vulnerable older adults.
The age-associated degenerative process occurring in the neuromuscular system leads to decreased muscle strength as well as motor coordination and control.Citation4,Citation40 While resistance exercise can increase muscle force production,Citation7,Citation41 a positive transfer to improvement on performing daily activities or tasks will require changes in muscle activation patterns as well.Citation42 In other words, a positive transfer is likely to occur when specific muscle activation patterns reinforced through training are required to execute the motor task. In our 3-Step Workout for Life program, this is done through functional exercise. Additionally, the degenerative process occurring at the cortical level is attributed to age-related decline in motor performance, such as the process slow down or becoming less smooth.Citation43 Older adults show over-recruitment of brain regions compared to young adults while performing a motor task.Citation43,Citation44 Therefore, late-life disability in activities of daily living to some extent is a motor skill deficit contributed by decline in the central nervous system and neuromuscular system. Based on this premise, an intervention that involves a task-oriented approach may help older adults regain competence in performing activities of daily living.Citation45 The task-oriented approach is a type of motor learning intervention that has been applied in the field of rehabilitation.Citation46,Citation47 In a task-oriented approach, motor skills are an interplay between different body systems while attempting to achieve a behavioral goal within a confined environment. By actively attempting to reach the behavioral goal, an individual learns to integrate various systems rather than focusing on movements alone. We speculated that the residual effect observed on the primary outcome in the 3-Step Workout for Life Group might be a result of motor learning following the functional exercise and activities of daily living exercise. Similar long-term residual effects were reported in studies which examined functional exercise.Citation34,Citation48 Further research is recommended to elucidate the application of task-oriented approach to reduce late-life disability in activities of daily living.
The most reported adverse events in the present study were muscle soreness and joint pain, which concurs with previous exercise studies.Citation49 However, the Resistance Exercise Only Group seemed to report more adverse events of muscle soreness and joint pain than the 3-Step Workout for Life Group. The stepwise approach in 3-Step Workout for Life could decrease stress to the muscles and joints and then reduce musculoskeletal-related adverse events. Instead of repeatedly training the same single muscle group (eg, biceps) as in the Resistance Exercise Only Group, the same single muscle group was supported by other muscle groups to produce functional movements (eg, carrying) during functional exercise, and then to perform daily tasks (eg, restoring dishes from the dish dryer to the overhead cupboard) during activities of daily living exercise in the 3-Step Workout for Life Group.
Conclusion
Participants in the current study were solely recruited from subsidized senior housing communities, which could limit the generalizability of the findings to older adults who live in the family home or affluent senior housing communities. There are several strengths of this study. The design of 3-Step Work for Life was guided by the disablement model.Citation11 The exercise intervention intensity, frequency, duration, and volume between the 3-Step Workout for Life Group and the Resistance Exercise Only Group were equivalent. The assessment items of AMPSCitation23 were not fixed across residents and evaluation time points, which could avoid “training for the test.” In other words, AMPS is able to show that 3-Step Workout for Life is not to improve specific activities of daily living but to improve the “ability” to perform activities of daily living. To our knowledge, this is the first comparative trial with long-term follow-up on the outcome of activities of daily living in vulnerable older adults. The superior residual effect identified in 3-Step Workout for Life may be critical for older adults, especially those who are unlikely to follow a continuous exercise regimen without an intermediate disruption. 3-Step Workout for Life could be adopted as a restorative approach by health care professionals who provide reablement serviceCitation50 to vulnerable older adults living in the community. In conclusion, compared to progressive resistance strength exercise alone, 3-Step Workout for Life is a relatively safe program with high attendance rates, and, more importantly, it is more effective in preventing the decline in the ability to perform activities of daily living for older adults who are at risk of losing independence at home.
Acknowledgments
The study was supported by the Retirement Research Foundation (grant # 2013-227).
Disclosure
The authors report no conflicts of interest in this work.
References
- Federal Interagency Forum on Aging-Related StatisticsOlder Americans 2016: Key Indicators of Well-beingWashington, DCU.S. Government Printing Office2016
- LuppaMLuckTWeyererSKonigHHBrahlerERiedel-HellerSGPrediction of institutionalization in the elderly. A systematic reviewAge Ageing201039313819934075
- GuralnikJMAlecxihLBranchLGWienerJMMedical and long-term care costs when older persons become more dependentAm J Public Health2002921244124512144976
- HairiNNCummingRGNaganathanVLoss of muscle strength, mass (Sarcopenia), and quality (Specific Force) and its relationship with functional limitation and physical disability: the Concord Health and Ageing in Men ProjectJ Am Geriatr Soc2010582055206221054284
- RantanenTGuralnikJMSakari-RantalaRDisability, physical activity, and muscle strength in older women: the Women’s Health and Aging StudyArch Phys Med Rehabil19998013013510025485
- LiuCJLathamNKProgressive resistance strength training for improving physical function in older adultsCochrane Database Syst Rev2009CD00275919588334
- MartinsWRde OliveiraRJCarvalhoRSde Oliveira DamascenoVda SilvaVZSilvaMSElastic resistance training to increase muscle strength in elderly: a systematic review with meta-analysisArch Gerontol Geriatr20135781523562413
- KeysorJJDoes late-life physical activity or exercise prevent or mini-mize disablement? A critical review of the scientific evidenceAm J Prev Med200325129136
- KeysorJJJetteAMHave we oversold the benefit of late-life exercise?J Gerontol A Biol Sci Med Sci200156M412M42311445600
- GuMOConnVSMeta-analysis of the effects of exercise interventions on functional status in older adultsRes Nurs Health20083159460318546240
- VerbruggeLMJetteAMThe disablement processSoc Sci Med1994381148146699
- MartinGKLatimerAEBrawleyLRJungMEHicksALWeight training to activities of daily living: helping older adults make a connectionMed Sci Sports Exerc20063811612116394963
- GamblePImplications and applications of training specificity for coaches and athletesStrength Cond J2006285458
- LiuC-jShiroyDMJonesLYClarkDOSystematic review of functional training on muscle strength, physical functioning, and activities of daily living in older adultsEur Rev Aging Phys Act20141195106
- ManiniTMarkoMVanArnamTEfficacy of resistance and task-specific exercise in older adults who modify tasks of everyday lifeJ Gerontol A Biol Sci Med Sci20076261662317595417
- DobekJWhiteKGunterKThe effect of a novel ADL-based training program on performance of activities of daily living and physical fitnessJ Aging Phys Act200715132517387226
- LiuC-JJonesYLFormyduvalRMAClarkODTask-oriented exercise to reduce ADL disability in vulnerable elderly: a feasibility study of 3-Step Workout for LifeJ Aging Phys Act20162438439226583695
- GuralnikJMSimonsickEMFerrucciLA short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admissionJ Gerontol199449M85M948126356
- BohannonRWPeolssonAMassy-WestroppNDesrosiersJBear-LehmanJReference values for adult grip strength measured with a Jamar dynamometer: a descriptive meta-analysisPhysiotherapy2006O921115
- CallahanCMUnverzagtFWHuiSLPerkinsAJHendrieHCSix-item screener to identify cognitive impairment among potential subjects for clinical researchMed Care20024077178112218768
- KrebsEELorenzKABairMJDevelopment and initial validation of the PEG, a three-item scale assessing pain intensity and interferenceJ Gen Intern Med20092473373819418100
- KroenkeKSpitzerRLThe PHQ-9: a new depression diagnostic and severity measurePsychiatr Ann20023217
- FisherAGJonesKBAssessment of Motor and Process Skills. Volume 1: Development, Standardization, and Administration Manaul (7th Ed, Revised)Fort Collins, COThree Star Press, INC2012
- DobleSEFiskJDLewisNRockwoodKTest-retest reliability of the Assessment of Motor and Process Skills in elderly adultsOccup Ther J Res199919203215
- HayaseDMosenteenDThimmaiahDZemkeSAtlerKFisherAGAge-related changes in activities of daily living abilityAust Occup Ther J200451192198
- FisherAGThe assessment of IADL motor skills: an application of many-faceted Rasch analysisAm J Occup Ther1993473193298322873
- DesrosiersJBravoGHebertRDutilEMercierLValidation of the Box and Block Test as a measure of dexterity of elderly people: reliability, validity, and norms studiesArch Phys Med Rehabil1994757517558024419
- PodsiadloDRichardsonSThe timed “Up & Go”: a test of basic functional mobility for frail elderly personsJ Am Geriatr Soc1991391421481991946
- BorgGPsychophysical scaling with applications in physical work and the perception of exertionScand J Work Environ Health19901655582345867
- EllisonSFisherAGDuranLThe alternate forms reliability of the new tasks added to the Assessment of Motor and Process SkillsJ Appl Meas20002121134
- LiangK-YZegerSLLongitudinal data analysis of continuous and discrete responses for pre-post designsSankhyā200062134148
- LuKOn efficiency of constrained longitudinal data analysis versus longitudinal analysis of covarianceBiometrics20106689189619764951
- LiuGFLuKMoggRMallickMMehrotraDVShould baseline be a covariate or dependent variable in analyses of change from baseline in clinical trials?Stat Med2009282509253019610129
- de VreedePLSamsonMMVan MeeterenNLDuursmaSAVerhaarHJFunctional-task exercise versus resistance strength exercise to improve daily function in older women: a randomized, controlled trialJ Am Geriatr Soc20055321015667369
- de VreedePLSamsonMMvan MeeterenNLvan der BomJGDuursmaSAVerhaarHJFunctional tasks exercise versus resistance exercise to improve daily function in older women: a feasibility studyArch Phys Med Rehabil2004851952196115605332
- LallyFCromePUnderstanding frailtyPostgrad Med J200783162017267673
- FatourosIGKambasAKatrabasasIStrength training and detraining effects on muscular strength, anaerobic power, and mobility of inactive older men are intensity dependentBr J Sports Med20053977678016183776
- KalapotharakosVIDiamantopoulosKTokmakidisSPEffects of resistance training and detraining on muscle strength and functional performance of older adults aged 80 to 88 yearsAging Clin Exp Res20102213414020440099
- ZechADreyMFreibergerEResidual effects of muscle strength and muscle power training and detraining on physical function in community-dwelling prefrail older adults: a randomized controlled trialBMC Geriatr2012126823134737
- SeidlerRDAlbertsJLStelmachGEChanges in multi-joint performance with ageMotor Control20026193111842268
- ScanlonTCFragalaMSStoutJRMuscle architecture and strength: adaptations to short-term resistance training in older adultsMuscle Nerve20144958459223893353
- BarryBKCarsonRGThe consequences of resistance training for movement control in older adultsJ Gerontol A Biol Sci Med Sci200459M730M754
- SeidlerRDBernardJABurutoluTBMotor control and aging: Links to age-related brain structural, functional, and biochemical effectsNeurosci Biobehav Rev20103472173319850077
- WardNSCompensatory mechanisms in the aging motor systemAgeing Research Reviews2006523925416905372
- Shumway-CookAWoollacottMMotor Control: Translating Research into Clinical PracticePhiladelphia, PALippincott Williams & Wilkins2017
- MastosMMillerKEliassonA-CImmsCGoal-directed training: linking theories of treatment to clinical practice for improved functional activities in daily lifeClin Rehabil200721475517213241
- WinsteinCJWolfSLSchweighoferNTask-oriented training to pormote upper extremity recoverySteinJHarveyRLWinsteinCJZorowitzRDWittenbergGFStroke Recovery and Rehabilitation2nd edNew York, NYDemos Medical2015320343
- Giné-GarrigaMGuerraMPagèsEManiniTMJiménezRUnnithanVBThe effect of functional circuit training on physical frailty in frail older adults: a randomized controlled trialJ Aging Phys Act20101840142420956842
- LiuCJLathamNAdverse events reported in progressive resistance strength training trials in older adults: 2 sides of a coinArch Phys Med Rehabil2010911471147320801270
- AspinalFGlasbyJRostgaardTTuntlandHWestendorpRGReablement: supporting older people towards independenceAge Ageing201645574578