
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
Left ventricular hypertrophy (LVH) is one of the preclinical manifestations of hypertensive target organ damage (TOD). However, it remains unclear which electrocardiographic criterion perform better in diagnosing LVH.
Purpose
To investigate the consistency of LVH diagnosed by electrocardiography (ECG) and echocardiography (ECHO). Taking LVH by ECHO as reference, to compare three different ECG criteria (Sokolow-Lyon, Cornell and Cornell Product criteria) and find the best ECG indicator for identifying LVH in community-based elderly Chinese.
Patients and methods
Echocardiography and electrocardiography were applied to define LVH in 1789 elderly Chinese aged >65 years old in communities located at the northern Shanghai. Echocardiographic LVH (ECHO-LVH) was defined by left ventricular mass indexed for Body Surface Area (LVM/BSA) or for height2.7 (LVM/height2.7). Electrocardiographic LVH (ECG-LVH) was defined by Sokolow-Lyon (SL), Cornell and Cornell Product (CP) criteria. ECHO-LVH was defined by LVM/BSA≥125 g/m2 in male or ≥110 g/m2 in female (LVH1); LVM/BSA≥115 g/m2 in male, or ≥95 g/m2 in female (LVH2) and LVM/height2.7 ≥51 g/m2.7 in male or ≥47 g/m2.7 in female (LVH3).
Results
As compared with SL and Cornell criteria, CP had the greatest correlation coefficient in the association with echocardiography-defined LVH, except for LVM/BSA in men. Of note, CP criterion had the greatest area under curve of ROC than Cornell criterion and the SL index, not only in total population but also in subgroups classified by blood pressure.
Conclusion
In ECG-LVH criteria, CP criterion complies better than SL index and Cornell criterion in assessing cardiac hypertrophy.
Introduction
Left ventricular hypertrophy (LVH) is one of the preclinical manifestations of hypertensive target organ damage (TOD).Citation1 It is an independent risk factor of cardiovascular events and the diagnosis of LVH in the early stage is a strong predictor of morbidity.Citation2–Citation5 Long-term increased afterload may generate cardiac remodeling, which explains the formation mechanism of LVH.
Electrocardiography (ECG) and echocardiography (ECHO) can be applied to detect LVH in clinical practice. The diagnosis of LVH should preferably be made by ECHO because it can visually measure every parameter of cardiac structure in a noninvasive method. Furthermore, its high sensitivity and specificity make it a golden standard for the LVH detection. However, many conditions have restricted ECHO application in routine clinical practice, including operators’ uneven levels and high expense. The 12-lead resting ECG, another noninvasive method for detecting LVH, on the other hand, is more convenient, economic, and suitable for screening in a large scope.
More than 30 ECG criteria have been invented to define LVH over the past decades,Citation6 including Lewis voltage, Gubner–Ungerleider voltage, RaVL, Romhilt–Estes score, left ventricular strain, RV6:RV5 ratio, Framingham criterion, Perugia criterion, and so on. But a few of them are still used in routine clinical practice. For instance, Sokolow et al developed Sokolow voltage to detect LVH in 1949 for the first time and it was widely used in the past.Citation7 Lyon and Rappaport developed the method successively. Sokolow-Lyon (SL) index is a classical approach to define LVH, and it calculates the sum of QRS voltage of S wave in V1 and R wave in V5 or V6. Some investigators pointed out that QRS duration is an independent predictor of LVH;Citation8 as a result, Cornell criterion and Cornell voltage-duration product (CP) were developed. The Cornell criterion means S wave in V3 plus R wave in aVL, and the CP criterion means Cornell criterion multiplied by the QRS duration.
In some studies, it was indicated that Cornell and CP criteria performed better than the SL index,Citation9 whereas some studies tend to deliver a different opinion.Citation10,Citation11 It remains unclear which ECG criterion shows better reasoning in diagnosing LVH. Considering most ECG criteria have been established in the Caucasian, we aim to compare three different ECG criteria, taking LVH by ECHO as reference, to find out the best ECG indicator for identifying LVH in a community-based elderly Chinese.
Materials and methods
Study design and subjects
The Northern Shanghai Study (NSS) is a prospective population study with 1,789 community-dwelling elderly Chinese aged >65 years old. A systematic cardiovascular risk was conducted. Individuals who met the following eligible criteria were enrolled for this study: 1) those who are aged >65 years of age (based on birthday in their identity card); 2) those who volunteer to sign an informed consent; 3) long-term residents in northern part of Shanghai. Individual is excluded if he or she is: 1) unwilling to participate in the clinical study; 2) suffering from severe cardiac disease (New York Heart Association IV) or end-stage renal disease (Chronic kidney disease stage 4 or above); 3) diagnosed with cancer with life expectancy of less than 5 years; 4) developed stroke within 3 months; 5) suffering from other diseases to quit the study; 6) against the protocol; and 7) losing contact with laboratory staff. A total of 1,758 participants out of 1,789 subjects of NSS were included in the study, with 31 excluded because of absence of data. Subjects were notified both through phone calls and local neighborhood committees. Each subject was asked to undergo laboratory and clinical tests at either the Tenth People’s Hospital of Tongji University or in the communities. The operators of ECG and ECHO were well-trained and we would readily test again if it was necessary to ensure accuracy of the data obtained from ECG and ECHO. All participants signed the informed consent. The protocol of the present study was approved by the ethics committee of the Shanghai Tenth People’s Hospital. The study was conducted in accordance with the Declaration of Helsinki.
ECG
A 12-lead resting ECG was recorded at 25 mm/s and 1 mV/cm standardization with equipment that have frequency response characteristics conforming to the recommendations of the American Heart Association.Citation12 Electrocardiographic QRS wave voltage was detected in this study. Parameters include the voltage of the S wave of the leads V1 (SV1) and V3 (SV3), R wave of lead V5 (RV5) and aVL (RaVL), and the duration of QRS wave. Several electrocardiographic indices, namely SL index, Cornell criterion, and Cornell QRS duration product, were applied to assess high voltage of left ventricle to diagnose LVH. LVH was diagnosed as SV1 + RV5 ≥3.5 mV for SL index,Citation7 SV3 + RaVL ≥2.8 mV in males and ≥2.0 mV in females for Cornell criterion,Citation13 and (SV3 + RaVL) × QRS duration ≥244 mV/ms in males and (SV3 + RaVL + 0.6) × QRS duration ≥244 mV/ms in females for CP criterion.Citation14
ECHO
Echocardiographic measurement was performed by one sonographer who was blind to other data. Interventricular septum (IVS), left ventricular internal diameter (LVID), and posterior wall thickness (PWT) were measured, and left ventricular mass (LVM) was calculated using the American Society of Echocardiography (ASE) recommended formula:
LVM was standardized by body surface area (BSA) and body height2.7 as LVM/BSA and LVM/height,2.7 respectively. LVH was diagnosed as LVM/BSA >95 g/m2 in females and >115 g/m2 in malesCitation15 as per the novel ASE criterion, LVM/BSA >110 g/m2 in females and >125 g/m2 in malesCitation1 according to the former ASE criterion, and LVM/height >51 g/m2.7 in males and >47 g/m2.7 in femalesCitation16 by other criteria.
Statistical analyses
All data statistics were analyzed using SAS software, version 9.3 (SAS Institute, Cary, NC, USA) and SigmaPlot software, version 12.5 (Systat Software, Inc., San Jose, CA, USA). All measured values were reported as means ± SD for continuous variables, numbers and percentages in parenthesis for categorical variables. Pearson’s correlation coefficients were used to evaluate the degree of correlation between the three ECG criteria and the two indexed LVMs, namely LVM/BSA and LVM/height2.7, and chi-squared test was used to analyze the categorical variables. Fisher transformation analysis was conducted to compare the correlation coefficients. Receiver operating characteristic (ROC) curves and the areas under the curves analyses were conducted to compare the sensitivity and specificity for the three ECG criteria using conventional cut-off values. P<0.05 was considered statistical significance.
Results
Characteristics of participants
Characteristics of participants by gender are shown in , including conventional cardiovascular risk factors, hypertensive TOD, and ECG and ECHO parameters. Among 1,758 participants, 784 (44.6%) were men, of which 336 (19.1%) participants were suffering from diabetes, and 921 (52.4%) from hypertension. Men, compared with women, were significantly taller (164.4±6.1 vs 154.8±5.7 cm, P<0.001), and had higher BSA (1.76±0.15 vs 1.58±0.14 m2, P<0.001), S wave amplitude in V3 lead (0.82±0.46 vs 0.65±0.42 mV, P<0.001), QRS duration (95.90±15.35 vs 87.47±12.81 ms, P<0.001), SL index (2.61±0.85 vs 2.31±0.73, P<0.001), Cornell criterion (1.23±0.57 vs 1.08±0.53), PWT (9.27±1.57 vs 8.96±1.54 mm, P<0.001), LVID (47.90±7.05 vs 45.75±6.43 mm, P<0.001), and LVM (161.0±57.1 vs 143.1±48.1 g, P<0.001), but lower CP criterion (118.8±64.7 vs 147.5±53.1 mV/ms, P<0.001) and LVM/height2.7 (40.8±14.3 vs 44.2±15.5, P<0.001).
Table 1 Characteristics of participants by gender
Characteristics of participants by hypertensive status are shown in . All observation indices, such as age, R wave amplitude in lead aVL, S wave amplitude in lead V3, QRS duration, SL index, Cornell criterion, CP criterion, IVS, PWT, LVID, LV, LVM/BSA, and LVM/height2.7 had significantly greater value in hypertensive participants (P<0.05).
Table 2 Characteristics of participants by hypertensive status
Correlations between ECG and ECHO parameters
As shown in , SL, Cornell, and CP parameters were all significantly correlated with LVM/BSA in total population, in both men and women (all P≤0.01). There were no significant differences in correlation coefficients among those parameters by the Fisher transformation analysis. As for LVH parameter and LVM/height2.7, all the three ECG parameters were significantly correlated in total population, in both men and women (P<0.01), except for the association of LVM/height2.7 with SL index in females (P=0.09).
Table 3 Correlation coefficient (R) between the electrocardiographic and echocardiographic parameters for the detection of LVHin total participants, in both males and females
Discrepancies in the diagnosis of LVH by ECG and ECHO
In , echocardiograph-diagnosed LVH is defined by LVM/BSA ≥125 g/m2 in males and ≥110 g/m2 in females as LVH1, by LVM/BSA ≥115 g/m2 in males and ≥95 g/m2 in females as LVH2, and by LVM/height2.7 ≥51 g/m2.7 in males and ≥47 g/m2.7 in females as LVH3. In order to determine whether the Chinese method is superior to the commonly used SL criterion, we conducted SL-China criterion as well. Electrocardiograph-diagnosed LVH is defined by SV1 + RV5 ≥4.0 mV in males and ≥3.5 mV in females by the SL-China criterion, by SV1 + RV5 ≥3.5 mV irrespective of genders for SL criterion, by SV3 + RaVL ≥2.8 mV in males and ≥1.0 mV in females for Cornell criterion, and by (SV3 + RaVL) × QRS duration ≥244 mV/ms in males and (SV3 + RaVL + 6) × QRS duration ≥244 mV/ms in females for CP criterion. Significant discrepancies were found between LVH diagnosed by the Cornell criterion and LVH1 (P=0.02), between LVH diagnosed by the Cornell criterion and LVH2 (P=0.04), between LVH diagnosed by the CP criterion and LVH2 (P=0.02), and between LVH diagnosed by the CP criterion and LVH3 (P<0.01). Of note, LVH diagnosed by the SL-China criterion and SL criterion were significantly and consistently different from LVH1, LVH2, and LVH3 (all P<0.01); furthermore, SL criterion was slightly superior to SL-China criterion.
Table 4 Chi-squared test between LVH diagnosed by ECG and by ECHO
Area under receiver operating characteristic (ROC) curve
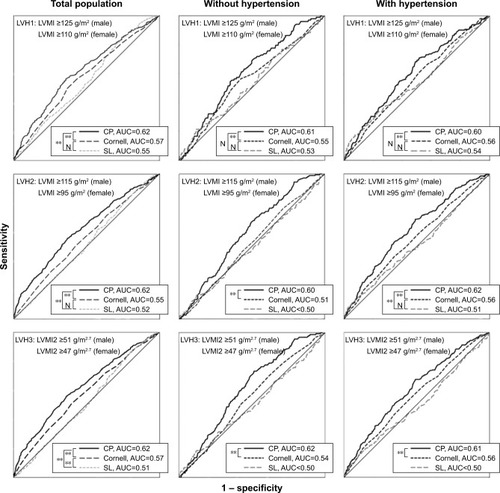
In , the ROC curve is applied to estimate the diagnostic value of CP criterion compared to Cornell and SL in detecting LVH. As shown in , CP criterion has the largest area under curve, not only in total population but also in subgroup classified by hypertension.
Figure 1 ROC curve with three electrocardiographic criteria for detecting LVH1, LVH2, and LVH3, the ROC curve for defining LVH1 using LVM indexed for BSA (LVMI) ≥125 g/m2 in males and ≥110 g/m2 in females; the ROC curve for defining LVH2 using LVM indexed for BSA (LVMI) ≥115 g/m2 in males and ≥95 g/m2 in females; the ROC curve for defining LVH3 using LVM indexed for BSA (LVMI2) ≥51 g/m2.7 in males and ≥47 g/m2.7 in females. N indicates P>0.05 and **indicates P<0.01.
Discussion
In this study, three commonly used ECG criteria, the SL index, Cornell criterion, and CP criterion, were compared for detecting LVH in a large community-based elderly population located in the northern part of Shanghai, taking echocardiograph-defined LVH as reference. The major finding of this study was that CP criterion is superior to SL index and Cornell criterion for LVH assessment.
Two LVM indices were determined by echocardiograph in this study, namely, LVM/BSA and LVH/height2.7. The index of LVM to height2.7 was supposed to be a more sensitive one for estimating LVH.Citation17 Moreover, the index of LVM to BSA was implemented as well. As shown in , there was no significant difference of LVM/BSA between genders (P=0.54), whereas the difference of LVM/height2.7 between genders is significant (P<0.001). On the contrary, previous study by Simone et alCitation17 and Park et alCitation18 reported the opposite results. The difference may rely on different populations.
Okin et al,Citation8 Hsieh et al,Citation4 Molly et al,Citation14 Xie et al,Citation19 and Peguero et alCitation20 argued that isolated QRS voltage amplitude combined with QRS duration might enhance diagnostic sensitivity when ECG was used to detect LVH in the previous studies. We analyzed CP criterion, the composite one that is derived by multiplying Cornell voltage criterion and QRS duration, together with Cornell voltage criterion and SL index. The higher correlation coefficient, lower chi-squared values and greater area under the ROC curve of CP criterion make it the best indicator to evaluate LVH, and this is in accordance with previous studies by Salles et alCitation21 and by Xie et al.Citation19 However, subjects from the Salles’s study were resistant hypertensives with a prevalence of LVH 87%, which is much higher than the current study.
Even integrating isolated QRS voltage without QRS duration, Cornell criterion is still superior to SL index in detecting LVH.Citation22 The same findings are detected in the study by Casale et alCitation23 as well. Based on a meta-analysis by Pewsner et al,Citation24 the highest sensitivity of electrocardiographic LVH (ECG-LVH) was 68%. Nevertheless, the lowest is only 0, and the sensitivity in most of the collected studies ranges from 10% to 30%. By studying different ethnic groups, Rodrigues et alCitation25 and Park et alCitation18 demonstrated that Cornell criterion performs better than SL index, though the sensitivity of both criteria is low.
Of note, an overwhelming majority of Chinese clinicians adopt a gender-specified SL index to diagnose LVH and the threshold is defined as SV1 + RV5 ≥4.0 mV in males and ≥3.5 mV in females.Citation26 Comparison of SL-China and SL index is shown in . Though the discrepancies between the two SL criteria and ECHO were still high (P<0.01), SL-China even had larger chi-squared values than commonly used SL index. Over the past 60 years, Chinese clinicians have been keeping faith in the conventional ECG-LVH criterion formed in the 1950s.Citation26 In addition, a recent investigation by Antikainen et alCitation27 reported that there is no significant increase in the risk of any cardiovascular events associated with LVH diagnosed by SL index. Moreover, Wong et alCitation28 and Courand et alCitation29 once proposed to give up SL criterion as well.
The findings of this study have important clinical implications. The expenditure of LVH diagnosed by ECHO is much greater than by ECG. Besides, ECG is cheaper and more convenient in routine clinical practice than ECHO or magnetic resonance imaging. Generally, ECHO is used for correct diagnosis of LVH in inpatients rather than to screen LVH in community or outpatients. LVH is a common hypertensive TOD. It has significant association with events related to cardiovascular diseases. Therefore, it is very important to diagnose LVH. As the diagnostic accuracy of the SL criterion is very low, Cornell criterion, especially CP criterion, should be implemented in routine clinical practice. Okin et al successfully applied CP to detect LVH in the LIFE study. Because the algorithm of CP criterion is slightly complex, it is strongly recommended to adapt this algorithm to the inbuilt software, in order to automatically offer those indices to physicians and decision-makers. Considering the differences between LVH electrocardiographic criteria in their ability to detect LV, CP criterion is recommended.
It is noteworthy that the study results are derived from a population-based cross-sectional study. Therefore, we aim at investigating the accuracy of different ECG-based formulas in estimating cardiac hypertrophy rather than the prognostic value of those formulas for predicting future cardiovascular events and mortality. With the ongoing follow-up, the prognostic data will be provided in the near future.
The findings of the present study need to be interpreted within the context of its limitations. First, we only applied conventional echocardiograph to define LVH, without using some novel technologies, such as tissue Doppler imaging or speckle tracking. But our conventional measurements are also widely applied in the routine clinical practice. Second, though some ECG measurements were repeated for some cases with large discrepancies, we did not perform the analysis for the day-to-day variability of measurements.
Conclusion
In summary, by comparing echocardiographic-LVH with ECG-LVH in a community-based cohort, it is indicated that CP criterion performs better than Cornell voltage criterion and SL index. CP may substitute the SL index to detect LVH, particularly in China.
Author contributions
Original data was provided by Wei Zhang, Yiwu Zhou, Bin Bai, Shikai Yu, Jing Xiong, Chen Chi, Jiadela Teliewubai and Jue Li for this study. Methods and protocol were formulated and designed by Jacques Blacher, Yi Zhang and Yawei Xu. Manuscript was drafted by Wei Zhang and Yiwu Zhou. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgments
We would like to express our gratitude to all those who participated in the Northern Shanghai Study. We also thank Yuyan Lu, Hongwei Ji, Ximin Fan, Kai Wang, and Bhavana Rajbanshi for their contribution and valuable advice. This analysis is taken from the Northern Shanghai Study, which receives financial support from the Shanghai municipal government (Grant IDs 2013ZYJB0902 and 15GWZK1002). Dr Yi Zhang was supported by the National Nature Science Foundation of China (Grant IDs 81300239 and 81670377). The preliminary results of our research were presented orally at the ESH conference, and the abstract was published in the Journal of Hypertension. The hyperlink is: https://insights.ovid.com/crossref?an=00004872-201609001-00424.
Disclosure
The authors report no conflicts of interest in this work.
References
- ManciaGRoseiEACifkovaREuropean Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertensionEur Heart J2003342821592219
- BluemkeDAKronmalRALimaJAThe relationship of left ventricular mass and geometry to incident cardiovascular events: the MESA (multi-ethnic study of atherosclerosis) studyJ Am Coll Cardiol200852252148215519095132
- NarayananKReinierKTeodorescuCElectrocardiographic versus echocardiographic left ventricular hypertrophy and sudden cardiac arrest in the communityHeart Rhythm20141161040104624657425
- HsiehBPPhamMXFroelicherVFPrognostic value of electrocardiographic criteria for left ventricular hypertrophyAm Heart J2005150116116716084164
- VerdecchiaPSchillaciGBorgioniCPrognostic significance of serial changes in left ventricular mass in essential hypertensionCirculation199897148549443431
- HancockEWDealBJMirvisDMAmerican Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; American College of Cardiology Foundation; Heart Rhythm Society. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: Part V: electrocardiogram changes associated with cardiac chamber hypertrophy: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized ElectrocardiologyJ Am Coll Cardiol20095311992100219281932
- SokolowMLyonTPThe ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leadsAm Heart J194937216118618107386
- OkinPMRomanMJDevereuxRBKligfieldPElectrocardiographic identification of increased left ventricular mass by simple voltage-duration productsJ Am Coll Cardiol19952524174237829796
- CrowRSPrineasRJRautaharjuPHannanPLiebsonPRRelation between electrocardiography and echocardiography for left ventricular mass in mild systemic hypertension (results from treatment of mild hypertension study)Am J Cardiol19957517123312387778546
- BacharovaLSzathmaryVKovalcikMMateasikAEffect of changes in left ventricular anatomy and conduction velocity on the QRS voltage and morphology in left ventricular hypertrophy: a model studyJ Electrocardiol201043320020819709670
- SundströmJLindLArnlövJZetheliusBAndrénBLithellHOEchocardiographic and electrocardiographic diagnoses of left ventricular hypertrophy predict mortality independently of each other in a population of elderly menCirculation2001103192346235111352882
- KossmannCEBrodyDABurchGERecommendations for standardization of leads and of specifications for instruments in electrocardiography and vectorcardiographyCirculation19673535836026021338
- CasalePNDevereuxRBKligfieldPElectrocardiographic detection of left ventricular hypertrophy: development and prospective validation of improved criteriaJ Am Coll Cardiol1985635725803161926
- MolloyTJOkinPMDevereuxRBKligfieldPElectrocardiographic detection of left ventricular hypertrophy by the simple QRS voltage-duration productJ Am Coll Cardiol1992205118011861401620
- LangRMBadanoLPMor-AviVRecommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular ImagingEur Heart J Cardiovasc Imaging201516323327125712077
- de SimoneGDevereuxRBDanielsSRKorenMJMeyerRALaraghJHEffect of growth on variability of left ventricular mass: assessment of allometric signals in adults and children and their capacity to predict cardiovascular riskJ Am Coll Cardiol1995255105610627897116
- de SimoneGDanielsSRDevereuxRBLeft ventricular mass and body size in normotensive children and adults: assessment of allometric relations and impact of overweightJ Am Coll Cardiol1992205125112601401629
- ParkJKShinJHKimSHA comparison of Cornell and Sokolow-Lyon electrocardiographic criteria for left ventricular hypertrophy in Korean patientsKorean Circ J201242960661323091505
- XieLWangZCorrelation between echocardiographic left ventricular mass index and electrocardiographic variables used in left ventricular hypertrophy criteria in Chinese hypertensive patients: PP.29.149Hellenic J Cardiol201051539140120876051
- BetjemanTJRigalesLHoffmanISaberioLPJorgePElectrocardiographic criteria for the diagnosis of left ventricular hypertrophyJ Am Coll Cardiol201770141829183128958340
- SallesGLeocádioSBlochKNogueiraARMuxfeldtECombined QT interval and voltage criteria improve left ventricular hypertrophy detection in resistant hypertensionHypertension20054651207121216203872
- ChapmanNMayetJOzkorMLampeFCThomSAPoulterNRQT intervals and QT dispersion as measures of left ventricular hypertrophy in an unselected hypertensive populationAm J Hypertens2001145 Pt 145546211368467
- CasalePNDevereuxRBAlonsoDRCampoEKligfieldPImproved sex-specific criteria of left ventricular hypertrophy for clinical and computer interpretation of electrocardiograms: validation with autopsy findingsCirculation19877535655722949887
- PewsnerDJüniPEggerMBattagliaMSundströmJBachmannLMAccuracy of electrocardiography in diagnosis of left ventricular hypertrophy in arterial hypertension: systematic reviewBMJ2007335762271117726091
- RodriguesSLD’AngeloLPereiraACKriegerJEMillJGRevision of the Sokolow-Lyon-Rappaport and Cornell voltage criteria for left ventricular hypertrophyArq Bras Cardiol2008901465318317640
- HuangWClinical electrocardiographyPeople’s Medical Publishing House1956 Chinese
- AntikainenRLPetersRBeckettNSLeft ventricular hypertrophy is a predictor of cardiovascular events in elderly hypertensive patients: hypertension in the very elderly trialJ Hypertens201634112280228627552643
- WongKYLimPOWongSYMacwalterRSStruthersADMacdonaldTMDoes a prolonged QT peak identify left ventricular hypertrophy in hypertension?Int J Cardiol2003892–317918612767541
- CourandPYLantelmePGossePElectrocardiographic detection of left ventricular hypertrophy: time to forget the Sokolow-Lyon index?Arch Cardiovasc Dis2015108527728025937357