Abstract
Objective
The objective of this study was to analyze the efficacy of multisensory versus muscle strengthening to improve postural control in healthy community-dwelling elderly.
Participants
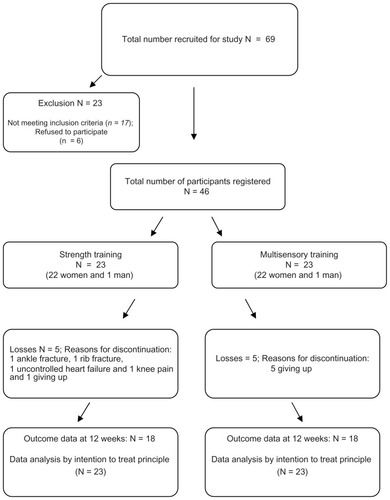
We performed a single-blinded study with 46 community-dwelling elderly allocated to strength (GS, n = 23; 70.18 ± 4.8 years 22 women and 1 man) and multisensory exercises groups (GM, n = 23; 68.8 ± 5.9 years; 22 women and 1 man) for 12 weeks.
Methods
We performed isokinetic evaluations of muscle groups in the ankle and foot including dorsiflexors, plantar flexors, inversion, and eversion. The oscillation of the center of pressure was assessed with a force platform.
Results
The GM group presented a reduction in the oscillation (66.8 ± 273.4 cm2 to 11.1 ± 11.6 cm2; P = 0.02), which was not observed in the GS group. The GM group showed better results for the peak torque and work than the GS group, but without statistical significance.
Conclusion
Although the GM group presented better results, it is not possible to state that one exercise regimen proved more efficacious than the other in improving balance control.
Introduction
Postural control is a key element in the execution of daily activities (eg, walking, sitting and standing from a chair, etc). This complex function requires input from the afferent receptor systems, vestibular, visual, proprioception, and general exterosensibility, in order to generate a motor response allowing the transition between dynamic and static activities.Citation1–Citation3 Aging is associated with a decrease in postural control, which contributes to the increase in falls among the elderly.Citation3–Citation5
One of the most common interventions to prevent the consequences (eg, fractures and falls) of decreased balance is physical exercise. Besides promoting better health conditions, physical exercise can improve postural control and reduce the tendency to falls in this population.Citation6,Citation7 A growing number of studies have demonstrated this association,Citation8 and several exercises have been shown to have some effect on the desired outcome.Citation9 In particular, multisensory exercisesCitation10–Citation12 are characteristically defined by the stimulation of all three afferent systems and the ones that strengthen body muscles.Citation13–Citation16 Although the latter exercises are efficacious in restoring muscle mass and strength, when they are performed in isolation, their effects on postural control have not been well defined.
We believe that interventions that assess how different exercises interfere with postural control will allow a better and customized design of therapeutic programs to achieve a reduction in falls.Citation8,Citation15 The objective of this study was to analyze the efficacy of multisensory versus muscle strengthening to improve postural control in healthy community-dwelling elderly people.
Methods
Design
The local ethics committee approved the study, and all participants signed an informed consent form. We chose a randomized, single-blinded controlled trial. The study design and procedure for recruitment have been described previously. Citation17 The study was performed in a rehabilitation center for outpatients in the central area of São Paulo, Brazil.
Subjects
The inclusion criteria were the following: age between 60 and 75 years; body mass index between 20 and 30; and ability to participate in physical activities. The exclusion criteria were the following: regular physical training in the last 3 months; severe clinical musculoskeletal impairments; implanted prosthesis of previous fractures in the axial skeleton or lower limbs; visual impairment without correction; and a recent complaint of dizziness or falls. Furthermore, subjects were discontinued from the study if they failed to participate in at least three consecutive training sessions. Before any intervention, they were evaluated by a physician in order to determine any clinical condition that might hinder participation in the study.
Assessment
Initially, subjects were assessed with the Timed Up and Go (TUG) test, which requires a subject to stand up, walk 3 m (10 ft), turn, walk back, and sit down. The time taken to complete the test is strongly correlated with the level of functional mobility.Citation18 Afterwards, they were evaluated with a functional balance test using the Berg Balance Scale. This test consists of a range of 14 common tasks that involve both static and dynamic balance, such as reaching, turning, standing, arising, and making transfers.Citation19
Subjects were evaluated before and after the interventions with a force platform (AMTI Inc, Watertown, MA). Where the oscillation of the body center of pressure area could be defined, we assumed this parameter to represent the whole body oscillation.Citation9,Citation10 After calibration, signs of oscillation of the body were recorded with the platform in the on-leg position. Data were captured with Eva software (Hewlett Packard®, Palo Alto, CA), in an acquisition frequency of 100 Hz. The area of movement of the center of pressure was measured in centimeters squared (cm2). We used a routine developed in Matlab (version 6.5®; MathWorks, Upper Saddle River, NJ) to process the data.Citation20
For the assessment of static balance, subjects remained standing barefoot wearing light clothes on the dominant lower limb with open eyes for 10 seconds. In order to calculate the mean, this procedure was repeated three times sequentially, and the subjects were requested to stare at a fixed point within approximately 1 m at eye level. Illumination, noise, and temperature were kept constant and comfortable for all subjects and sessions. One assessor was positioned beside the subject in order to provide support in the event of a fall.
Isokinetic evaluation of the ankle was performed with an isokinetic evaluator (Cybex Humac Norm®; Computer Sports Medicine, Stoughton, MA). Subjects were positioned supine with the hip fixed in 90° and knee flexion of 80°, and straps were used to keep the lower limb in a fixed position. The movements performed at the heel and foot joints included dorsiflexion, plantar flexion, invertion, and evertion.Citation21
Subjects were familiarized with the equipment during three rehearsals with free angular speed in order to get used to the movement to be tested. In order to calculate the mean, testing was performed in five repetitions at an angular speed of 30°/s, with concentric contractions of agonists and antagonists alternately though all ranges of motion. A verbal stimulus during the tests was essential to promote a better effort from subjects. Peak torque (N/m) and total work (J) were recorded.
Interventions
Subjects were asked not to participate in other physical activities and not to change their daily habits during the study. A computer-generated list randomly allocated the subjects to one of two training programs: strength training (GS) or multisensory training (GM). Both groups were subjected to one hour of training sessions on two different days a week. Subjects in both programs remained in training for 12 weeks.Citation9,Citation12
Multisensory exercises program (GM)
Multisensory intervention emphasized the stimuli to sensory systems. A warm-up period before the activity included short walks and games with balls using the hands or feet. These were followed by stretching exercises for hip muscles, flexors, and extensors of the knee, ankle, and paraspinal muscles. Activities were performed both standing and lying down. Resistance exercises for plantar flexors and dorsiflexors as well as squatting and abdominals were performed against gravity in order to strengthen lower limbs and trunk; three series of ten repetitions were performed for each of these exercises.
Subjects also performed activities to stimulate the plantar surface and dynamic balance. They were asked to walk forwards, backwards, and sideways, with eyes both open and closed at different speeds and for various distances. Ground surfaces also varied and included mattresses and different densities of foam rubber. The subjects were also challenged by obstacles, such as ropes, cones, and sticks. Balance training was performed with devices often directed to the following activity in physical therapy: according to the subject’s ability, he or she might be asked to remain standing on uni- or bipedal support with eyes open or closed. These sensorial challenges lasted from 20 to 30 minutes. Finally, motor coordination training was performed by alternate movements of the upper and lower limbs, different positions of the head and neck, both with and without visual stimuli.Citation12,Citation17
Strength exercises program (GS)
The muscle-strengthening program was performed using six different resistance devices with varying resistance: chest press, rowing, leg press, calves, abdominal, and lumbar extension. These devices were chosen because they load the main muscle groups.
At each device, the subjects were oriented to perform three series of exercises with varying loads: the first series of twelve repetitions were performed with a load at 50% of the maximum, the second (ten repetitions) at 75% of the maximum. The third series required eight repetitions at the maximum tolerated load. On the first day of training, the subjects did the exercises with no load in order to get used to the movements and posture. This value was estimated by successive trials and was defined as the load compatible with a complete range of motion, without a slow concentric or eccentric contraction, or sustained apnea. This value was then recorded to set new limits for the next session. The load was increased whenever it was possible to complete the last series of eight repetitions. Complaints of pain and breathing discomfort were actively elicited, and the speed of movements was constantly monitored in both concentric and eccentric phases.Citation17,Citation22,Citation23
Statistical analysis
The analysis considered a two-parallel arm design and an 80% probability of detecting a treatment difference at a two-sided 0.05 significance level. If the true difference between treatments was 1.5 units in TUG, two subjects were added in order to compensate for possible dropouts, which resulted in 46 subjects in the final sample. Data analysis was performed with the statistical package SigmaStat 3.5 for Windows (Systat Software, Point Richmond, CA). We used the principle of intention to deal with possible dropouts, and missing data were input with the mean of the remaining data. This strategy does not change the mean of the sample and prevents reduction of statistical power. However, it reduces the standard deviation and facilitates the identification of statistically significant results. The results were described as means and standard deviations. Comparisons of means at baseline between groups were performed using a two-tailed, independent Student’s t-test or Mann–Whitney U test. Comparisons within the groups after the treatments were performed with a paired Student’s t-test or Wilcoxon test, according to data distribution. The Mann–Whitney U test was used to test the differences in balance outcome variables between the groups in changes during the follow-up. The significance level was 0.05.
Results
From the 69 individuals recruited, 46 were eligible and provided their informed consent to participate. The progress of the participants through the various stages of the study is presented in .
Figure 1 Flow of patients through the study.
There were no statistically significant differences between the groups in terms of the proportion of female and male participants, age, and body mass index (BMI). Clinically, the groups were similar in functional terms before the intervention when TUG, Berg (), and displacement of center of pressure () were compared.
Table 1 General characteristics of participants at baseline (Mean ± SD)
Table 2 Displacement of center of pressure (cm2) (mean and standard deviation) within and between groups before and after interventions
Isokinetic parameters in the right () and left () ankles were very similar before the interventions in both groups, except for total work during invertion of the right ankles. Although the differences were not statistically significant, the mean peak torque and work were less in GS before the intervention. After the intervention, although GS presented with improvement in peak torque in plantar flexion bilaterally and dorsiflexion in the left side, the improvements in total work were not statistically significant. However, GM presented with improvement in peak torque in plantar flexion and dorsiflexion bilaterally and in inversion and eversion on the right side. The total work improvement was statistically significant for plantar flexion and dorsiflexion bilaterally in GM.
Table 3 Peak torque (N/m) and total work (J) of isokinetic assessment of right heel and foot movements (mean and standard deviation) at 30°/s, within and between groups: strength (GS) and multisensory (GM) before and after the interventions
Table 4 Peak torque (N/m) and total work (J) of isokinetic assessment of left heel and foot movements (mean and standard deviation) at 30°/s, within and between groups: strength (GS) and multisensory (GM) before and after the interventions
The comparisons after treatment between the groups of gains after the intervention in all isokinetic parameters were not statistically significant ( and ).
Discussion
We compared the benefits of two exercise regimens on postural control of healthy elderly subjects. Although both intervention groups showed statistically significant improvements in many parameters, and they did somewhat better in the multisensory approach, the differences between the groups were not statistically significant. Thus, although both interventions improved static and dynamic mobility in the healthy elderly subjects, we cannot state that either one is more efficacious.
Static balance is a predictor of independence and risk of falls in the elderly.Citation10,Citation24 Similarly, muscle action around the heel is also important because it is responsible for the control of this joint and thus support to the whole body. This outcome was assessed in this study because it is used in situations in which there is little disturbance of balance and the standing surface is stable, which were the conditions in this study.Citation2
Although the improvement of body oscillation in the GM group was not significantly greater than in the GS group, we believe the results obtained by the GM group are clinically important because the subjects in this group might have achieved better postural control.Citation25 Reduced oscillation of the body center of pressure indicates better postural control, whereas a wide area of oscillation might reflect the deterioration of postural control.Citation2 By testing this displacement in a standing position, it was possible to assess the muscle effort to maintain balance,Citation11 which was confirmed by the results of the isokinetic evaluation in the GM group. The reduced oscillation of the body center of pressure observed in the GM group is associated with the strengthening documented by the peak torque and work in the isokinetic assessment. This association was also observed in another study that used multisensory exercises three times a week for twelve weeks, in which improved action in gastrocnemius and tibialis anterioris resulted in the same improvement in balance.Citation9,Citation12
The elderly lose the ankle strategy for postural control due to the muscle weakness and peripheral sensory loss that occur in aging. Improvement of muscle action in this region, which is the first to be used for maintaining balance, can be a contributing factor in the prevention of falls among the elderly.Citation2,Citation12,Citation26,Citation27
Although the results for the two groups were not statistically different, we observed that only the GM group significantly improved the work of the dorsiflexor and plantar flexor muscles, which are important for the maintenance of static posture.Citation2,Citation12 This result led us to believe that the intensity, duration, and frequency of the strengthening exercises performed by the subjects in this study were not adequate to promote changes in the muscular action of the ankle joint.
The fact that multisensory exercises were able to reduce body sway in participants might be because this training provided sensory stimulation of the visual, vestibular, and somatosensory systems through exercises that were performed on different types of surfaces and densities. Furthermore, they used balls, circuits, and other devices that provided stimuli that enhance balance.Citation9–Citation11,Citation25,Citation28,Citation29
On the other hand, when used alone, muscle-strengthening exercises seem to have no effect on the improvement of balance in the elderly. This may be due to a decrease in sensory information because these exercises were conducted in a sitting position and not in an orthostatic posture in which the balance is most evident.Citation30,Citation31
Although strength exercise is often assumed to be beneficial for balance, one review provided evidence that strength exercise used as an isolated intervention is not uniformly effective in improving balance performance.Citation16 Only 22% of the results of the balance tests examined supported the efficacy of strength exercises as a single modality to improve balance.Citation16 Although there are significant differences between groups after the intervention, our results corroborate the literature in that stimuli of the sensory systems are required to achieve gains in postural control.Citation9,Citation16
Because it confirmed similar findings in other studies, we believe that the evidence in our study is valid and solid. However, the limitations of this study are the reduced sample size, lack of a comparison group with no training, and the design of the strength exercise programs in terms of load, duration, and frequency performed. These aspects can, however, be used as parameters for new steps in the understanding of the effects of multisensory exercises on postural control.
Conclusion
Although the group that performed multisensory exercises presented with a significant reduction of body oscillation and expressive improvement in isokinetic parameters on the heels after training, we cannot state that any of the exercise programs was superior for postural control.
Acknowledgments
The authors thank Leslie Andrews Portes for assistance with the data analysis and the statistics. We also thank Carolina Rodini, Luana Talita Diniz Ferreira, Gemal Emanuel Pirré for their assistance in the subject recruitment and the training. We acknowledge the contributions of Marcelo Alves Mourão and Adilson Gonçalves in the assessment of the functions of the subjects.
Disclosure
The authors declare no conflicts of interest in this work.
References
- AlexanderNBPostural control in older adultsJ Am Geriatric Soc19944293108
- Shumway-CookAWoollacottMMotor Control: Theory and practical applicationsBaltimore, MDWilliams and Wilkins1995
- WoollacottMShumway-CookAAttention and the control of posture and gait: a review of an emerging area of researchGait Posture200216111412127181
- TinettiMESpeechleyMGinterSFRisk factors for falls among elderly person living in the communityN Engl J Med1988319701707
- ChangJTMortonSCRubensteinLZInterventions for the prevention of falls in older adults: systematic review and meta-analysis of randomized clinical trialsBMJ20043281714703521
- MoreyMCSloaneRPieperCFEffect of physical activity guidelines on physical function in older adultsJ Am Geriatr Soc200856101873187818800990
- HubbardREFallahNSearleSDMitnitskiARockwoodKImpact of exercise in community-dwelling older adultsPLoS One200947e617419584926
- BulatTHart-HughesSAhmedAEffect of a group-based exercise program on balance in elderlyClin Interv Aging20072465566018225467
- HoweTERochesterLJacksonABanksPMHBlairVAExercise for improving balance in older peopleCochrane Database Syst Rev20074CD00496317943831
- RogersMERogersNLTakeshimaNIslamMMMethods to asses and improve the physical parameters associated with fall risk in older adultsPrev Med20033625526412634016
- RogersMEFernandezJEBohlkenRMTraining to reduce postural sway and increase functional reach in the elderlyJ Occup Rehabil200111429129811826729
- AlfieriFMGuirroRRJTeodoriRMPostural stability of elderly submitted to multisensorial physical therapy interventionElectromyogr Clin Neurophysiol201050211311920405787
- SeguinRNelsonMEThe benefits of strength training for older adultsAm J Prev Med20032514114914552938
- BruinEDMurerKEffect of additional functional exercises on balance in elderly peopleClin Rehabil20072111212117264105
- NitzJCChoyNLThe efficacy of a specific balance-strategy training program for preventing falls among older people: a pilot randomized controlled trialAge Ageing200433525814695864
- OrrRRaymondJSighMFEfficacy of progressive resistance training on balance performance in older adultsSports Med200838431734318348591
- AlfieriFMRibertoMGatzLSRibeiroCPCLopesJAFBattistellaLRFunctional mobility and balance in community-dwelling elderly submitted to multisensory versus strength exercisesClin Interv Aging2010518118520711437
- PodsiadloDRichardsonSThe timed “Up and Go”: a test of basic functional mobility for frail elderly personsJ Am Geriatr Soc1991391421481991946
- BergKOWoo-DauphineeSLWilliamsJIMakiBMeasuring balance in the elderly: validation of an instrumentCan J Public Health199283Suppl 2S7111468055
- RaymakersJASamsonMMVerhaarHJJThe assessment of body sway and the choice the stability parameter(s)Gait Posture2005211485815536033
- ImamuraMAvaliação Isocinética dos pés de Homens Adultos Normais. [dissertion]São Paulo, BrazilUniversidade de São Paulo1994
- WinettRACarpinelliEDPotential health-related benefits of resistance trainingPrev Med200133550351311676593
- KraemerWJAdamsKVafarelliEAmerican College of Sports MedicineAmerican College of Medicine position stand. Progression models in resistance training for healthy adultsMed Sci Sports Exerc200224236438011828249
- IslamMMNasuERogersMEKoizumiDRogersNlTakeshimaNEffects of combined sensory and muscular training on balance in Japanese older adultsPrev Med20043961148115515539049
- NagyEFeher-KissAMárnaiBDomján-PresznerAAngyanLHorvathGPostural control in elderly subjects participating in balance trainingEur J Appl Physiol20071009710417333243
- ThelenDGSchultzABAlexanderNBAshton-MillerJAEffects of age on rapid ankle torque developmentJ Gerontol A Biol Sci Med Sci199651M2262328808994
- HessJAWoollacottMEffect of high-intensity strength-training of functional measure of balance ability in balance-impaired older adultsJ Manipulative Physiol Ther20052858259016226626
- GauchardGCGangloffPJeandelCPerrinPPPhysical activity improves gaze and posture control in the elderlyNeurosci Res20034540941712657454
- KronhedACGMollerCOlssonBMollerMThe effect of short-term balance training on community dwelling older adultsJ Aging Phys Act200191931
- BellewJWYatesJWGaterDRThe initial effects of low-volume strength training on balance in untrained older men and womenJ Strength Cond Res20031712112812580667
- BarryBKCarsonRGThe consequences of resistance training for movement control in older adultsJ Gerontol200459730754