

Abstract
Background and Purpose
Elevated high-density lipoprotein cholesterol (HDL-C) levels have displayed protection against cardiovascular disease. However, the association between specific lipoprotein classes and first ischemic stroke (IS) has not been well defined, particularly in higher-risk hypertensive populations. Our study evaluated the associations of HDL-C with first IS in a Chinese hypertensive population.
Methods
The study population was obtained from a community-based cohort study of hypertension in Lianyungang and Rongcheng, China. A nested case-control design was used that included 2463 identified first IS cases and 2463 controls matched by age ± 1 year, sex, and region.
Results
After adjusting for potential confounders, HDL-C was inversely associated with first IS (adjusted odds ratio [aOR]: 0.91; 95% confidence interval [CI]: 0.85–0.98). HDL-C levels of at least 65.4 mg/dL displayed a significant protective effect for first IS (aOR: 0.82; 95% CI: 0.69–0.98). Conversely, adverse effects of first IS were observed for low-density lipoprotein cholesterol (LDL-C) levels ≥138.1 mg/dL (aOR: 1.20; 95% CI: 1.02–1.42) and triglyceride (TG) levels ≥140.8 mg/dL (aOR: 1.27; 95% CI: 1.09–1.49). The risk associations of LDL-C and TG with first IS were attenuated in the presence of high HDL-C (≥53.0 mg/dL); an increased risk of first IS was only found in the presence of low HDL-C (<53.0 mg/dL) when LDL-C (aOR: 1.66; 95% CI: 1.19–2.31) and TG (aOR: 1.47; 95% CI: 1.17–1.84) were combined with HDL-C for analysis.
Conclusion
In this community-based Chinese hypertensive population, higher HDL-C was a significant protective factor of first IS. These data add to the evidence describing the relationship between lipids and IS and suggest that HDL-C maybe is a marker of IS risk in Chinses hypertensive population.
Data Availability
The study protocol and statistical analysis plan of this article are available from the corresponding author upon reasonable request. All data requests should first be submitted to Gang Li for consideration. Access to available fully anonymized data may be granted 12 months after publication. Requesters will be asked to complete an application form detailing specific requirements, rationale, and proposed use. A data-sharing agreement must be signed. Requested data will be made available, along with supporting documentation (eg, data dictionary) on a secure server.
Results
Study Participants and Baseline Characteristics
We analyzed 2463 IS cases and 2463 matched controls (). The cases were more likely to have higher SBP (153.1 ± 21.9 vs 147.7 ± 20.8 mmHg, P < 0.001), DBP (90.0 ± 13.7 vs 86.7 ± 13.1 mmHg, P < 0.001), fasting glucose levels (6.5 ± 2.5 vs 6.0 ± 2.0 mmol/L, P < 0.001), BMI (26.0 ± 4.0 vs 25.5 ± 3.7 kg/m2, P < 0.001), and total homocysteine levels (14.1 ± 7.8 vs 13.5 ± 8.8 umol/L, P = 0.009) than controls. Because of our matching criteria, cases and controls were similar in age and sex. In the analysis of baseline lipid profiles, compared to the controls, IS cases had significantly higher levels of TG (143.7 ± 96.0 vs 129.0 ± 86.2 mg/dL, P < 0.001) and LDL-C (128.7 ± 32.7 vs 126.1 ± 32.4, P = 0.004) but a significantly lower level of HDL-C (59.6 ± 15.1 vs 62.0 ± 15.6 mg/dL, P < 0.001); the mean TC level was similar in the two groups (213.2 ± 47.4 vs 212.8 ± 46.5 mg/dL, P = 0.751) ().
Table 1 Baseline Characteristics of Study Participants with First Ischemic Stroke and Age- and Sex-Matched Controls
Associations of Specific Types of Blood Lipids with First IS
When HDL-C levels were examined as a continuous variable in an adjusted model that included potential confounders and TG and LDL-C levels, a protective effect was found with an adjusted odds ratio (aOR) of 0.91 (95% CI: 0.85–0.98) for one SD increase in the HDL-C level. This translated into a 9% reduction in the odds of experiencing stroke (). When HDL-C levels were categorized as tertiles, a significant protective effect was observed for IS in patients with levels of at least 65.4 mg/dL (aOR: 0.82; 95% CI: 0.69–0.98; P for trend = 0.029). However, this significant association was no longer present when HDL-C was categorized according to the current clinical criteria (<40 mg/dL in males and <50 mg/dL in females) (). Furthermore, none of the baseline variables showed effect modification of the associations between HDL-C and IS after the stratified analyses (Online Table I).
Table 2 Association of Fasting Serum Lipid Levels with Incident Risk of First Ischemic Stroke
Figure 1 Smoothing curves for the association of first IS with HDL-C, TG, LDL-C and TC. All the panels adjusted for body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting glucose, smoking status, alcohol consumption, use of antihypertensive drugs, and glucose-lowering drugs, total homocysteine (tHcy), and estimated glomerular filtration rate (eGFR). HDL-C (A): adjusted for all the above variables plus TG and LDL-C.TG (B): adjusted for all the above variables plus TC.LDL-C (C): adjusted for all the above variables plus HDL-C and TG.TC (D): adjusted for all the above variables plus TG.
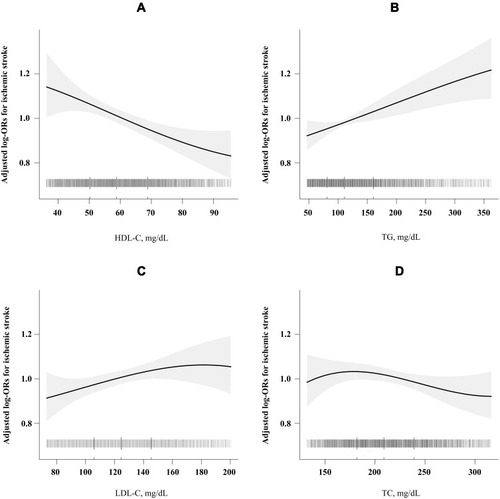
There was a significant positive association between TG levels and the risk of first IS after adjustment for potential confounders, as shown in . A one SD increase in TG concentration was associated with a 10% increased risk of first IS (aOR: 1.10; 95% CI: 1.02–1.17). When TG and LDL-C levels were categorized as tertiles, a significant adverse effect of first IS was observed for TG levels of at least 140.8 mg/dL (aOR: 1.27; 95% CI: 1.09–1.49; P for trend = 0.003) and LDL-C levels of at least 138.1 mg/dL (aOR: 1.20; 95% CI: 1.02–1.42; P for trend = 0.027) (). When LDL-C levels were examined as a continuous variable, no significant positive association was found with an aOR of 1.04 (95% CI: 0.97–1.12) for one SD increase in the LDL-C level () (). There was no significant relationship between TC levels and the risk of IS () ().
Combined Associations of HDL-C and LDL-C or TG with First IS
We performed stratified analyses to assess the effect of LDL-C (per one SD increment) on first IS by HDL-C tertiles. , which displays the association between LDL-C and the risk of first IS, indicates that there were different tendencies with different HDL-C levels. Only low HDL-C levels (<53.0 mg/dL) displayed a positive tendency with IS. The positive relationship between LDL-C and the risk of IS was attenuated in patients with higher HDL-C levels (≥53.0 mg/dL). Similarly, when LDL-C levels were categorized as tertiles, the highest risk for first IS was reported in participants with low HDL-C (<53.0 mg/dL) and high LDL-C (>138.1mg/dL) levels; these participants had a 66% higher risk of first IS than those with high HDL-C (>65.4 mg/dL) and low LDL-C (<111.4 mg/dL) levels (aOR: 1.66; 95% CI: 1.19–2.31; P = 0.003) (). The other combinations of HDL-C and LDL-C showed no significant associations with first IS.
Table 3 Combined Association of HDL-C and LDL-C Tertiles with First IS
Figure 2 Association of LDL-C or TG with first IS stratified by HDL-C levels. (A) Adjusted for body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting glucose, smoking status, alcohol consumption, use of antihypertensive drugs, and glucose-lowering drugs, total homocysteine (tHcy), and estimated glomerular filtration rate (eGFR) and TG (continuous). (B) Adjusted for body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting glucose, smoking status, alcohol consumption, use of antihypertensive drugs, and glucose-lowering drugs, total homocysteine (tHcy), and estimated glomerular filtration rate (eGFR) and LDL-C (continuous).
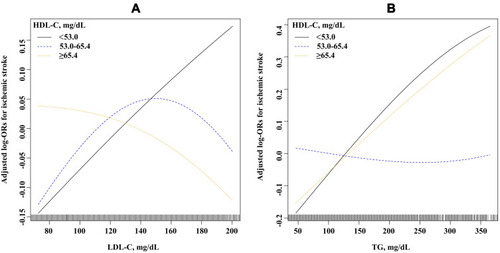
In the combined analysis investigating the associations of HDL-C and TG levels with first IS, the association of TG with first IS displayed a positive tendency only at lower HDL-C levels (<65.4 mg/dL); conversely, no significant association was found between the highest HDL-C tertile (>65.4 mg/dL) (). Similarly, patients with low HDL-C (<53.0 mg/dL) and high TG (>140.8 mg/dL) levels had a 47% higher risk of first IS (aOR: 1.147; 95% CI: 1.17–1.84; P < 0.001) than those with high HDL-C (>65.4 mg/dL) and low TG (<89.5 mg/dL) levels ().
Table 4 Combined Association of HDL-C and TG Tertiles with First IS
Discussion
To our knowledge, this is the first study to evaluate the prospective association between lipid profiles and the risk of IS in a community-based Chinese hypertensive population with no history of stroke and CHD. Our study contributes the following new insights into the HDL-C-IS association, for which previous studies have yielded conflicting results. This community-based case-control study demonstrated a protective effect of higher HDL-C levels for IS in a Chinese hypertensive population. This protective relationship was also observed in the combined analysis of HDL-C levels with LDL-C or TG and the risk of IS. In this combined analysis, elevated LDL-C and TG levels were no longer positively associated with first IS in the presence of higher HDL-C levels.
The relationship between abnormal serum lipid levels and stroke is less clear than this relationship for CHD. The protective effects of increased HDL-C levels on the risk of myocardial infarction have been established by numerous epidemiological studies;Citation6 however, this protective effect was not clear for stroke. Some cohort studies including the Framingham Heart Study have reported no association between HDL-C and IS;Citation12 however, some epidemiological studies support an inverse association.Citation13–Citation15 The absence of a consistent relationship between HDL-C and stroke may be partially explained by the heterogeneity of stroke, the focus on cardiovascular events rather than on stroke events, and the lack of classification of stroke subtypes. Furthermore, no significant reduction in CVD was observed including IS events in the AIM-HIGH and HPS2-THRIVE studies in association with HDL-C levels.Citation16,Citation17 However, these studies evaluated patients with a history of CVD. In contrast to the many studies conducted in Western countries, few Asian studies have been performed in this field; moreover, HDL-C levels were reported to be inversely associated with the risk of first IS in these studies.Citation10,Citation18,Citation19 Our current study provides further evidence of a protective effect of HDL-C on first IS. Moreover, this protective association was not evident when using the current clinical binary threshold, which underscores the need to consider HDL-C as a continuous trait rather than the current binary cutoff. The mechanisms of how HDL-C protects against CVD including IS are often explained by the ability of HDL to remove cholesterol from the periphery for delivery to the liver and excretion in the bile, a process termed reverse cholesterol transport.Citation20 The reverse cholesterol transport capacity of HDL-C is a potent protection for LDL-C oxidationCitation21,Citation22 and possesses anti-inflammatory properties.Citation23 Few previous studies have examined the combined associations of LDL-C and HDL-C with first IS. In a nested case-control study in the China Kadoorie Biobank (CKB) of Chinese populations, the associations of LDL-C and HDL-C with IS occurred independently of one another.Citation10 However, we found that the association between LDL-C and first IS differed by HDL-C levels. A positive relationship was found between LDL-C and the risk of IS only when combined with a low HDL-C level (<53.0 mg/dL). In other words, high HDL-C might attenuate the association between LDL-C and IS. Notably, our participants and those from the CKB study display differing characteristics. First, the average age of IS cases in our study was 67.6 years whereas it was 54.3 years in the CKB study. Secondly, our study included participants with hypertension (mean SBP of 153.1 mmHg for IS cases), whereas only slightly more than half of the participants were hypertensive (56.8%) (mean SBP was 144.1 mmHg for IS cases) in the CKB study.
The role of TG levels in atherosclerosis has remained unclear, and clinical recommendations have fluctuated from a need to reduce levels to not providing any advice on treatment.Citation24 Some studies, but not all, support a positive association between TG and the risk of first IS.Citation25,Citation26 Our study found that higher TG levels were a significant risk factor for the first IS incident in this Chinese hypertensive population. Furthermore, our study showed that the TG-IS association varied according to HDL-C levels. Only patients with low HDL (<53.0 mg/dL) and high TG (>140.8 mg/dL) levels had a significantly increased risk of first IS. The combined association of high TG and low HDL-C levels strongly predicted CHD in many studies.Citation27,Citation28 Consistently, many studies have shown that adjusting for HDL-C attenuates the association of TG with the risk of CVD.Citation29 The attenuation of the TG effect on CVD risk by high HDL-C is most likely caused by metabolic interactions.Citation30
Several limitations of our study design deserve discussion. The fact that this study was conducted in a community-based hypertensive population is both a strength and a limitation. The most important risk factor of atherosclerosis at the population level is hypertension,Citation31 and a study found that the protective association between high HDL-C and stroke was more significant in the hypertension subgroup.Citation32 However, our findings must be interpreted cautiously in non-hypertensive populations. Our study population was drawn from two coastal areas of China and thus may not represent the entire Chinese population. We only examined fasting lipids status and statin use at baseline, and it is not entirely clear whether the participants made changes to their diet or medications during the follow-up period. Although we controlled for important covariables, we cannot exclude the possibility of residual confounding. Finally, as an observational study, we cannot make a causal conclusion between lipid levels and first IS.
Conclusions
In this Chinese hypertensive population, we have shown that HDL-C levels were a significant protective factor for IS risk. Elevated LDL-C and TG levels were no longer associated with first IS in the presence of high HDL-C. These findings, if further confirmed, suggest a new paradigm that possibly shifts from LDL-C as the center of focus to HDL-C as an important player in first IS in Chinese hypertensive populations.
Acknowledgments
We acknowledge the contribution of all the research staff as well as the study participants who have participated in this study. No medical writer or editor was involved in the creation of this manuscript. The abstract of this paper was presented at the International Stroke Conference 2020 name “HDL-C levels inversely associated with first ischemic stroke in a Chinese hypertensive population” as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Stroke Journal name “HDL-C levels inversely associated with first ischemic stroke in a Chinese hypertensive population”.
Abbreviations
aOR, adjusted odds ratio; BMI, body mass index; CDC, Centers for Disease Control and Prevention; CHD, coronary heart disease; CI, confidence interval; CVD, cardiovascular disease; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; HHPCP, H-type Hypertension Prevention and Control Public Service Project; IS, ischemic stroke; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; TC, total cholesterol; TG, triglycerides.
Disclosure
The authors report no conflicts of interest in this work.