Abstract
Background
French maritime pine bark extract (PBE) has gained popularity as a dietary supplement in the treatment of various diseases due to its polyphenol-rich ingredients. Oligometric proanthocyanidins (OPCs), a class of bioflavonoid complexes, are enriched in French maritime PBE and have antioxidant and anti-inflammatory activity. Previous studies have suggested that French maritime PBE helps reduce ultraviolet radiation damage to the skin and may protect human facial skin from symptoms of photoaging. To evaluate the clinical efficacy of French maritime PBE in the improvement of photodamaged facial skin, we conducted a randomized trial of oral supplementation with PBE.
Methods
One hundred and twelve women with mild to moderate photoaging of the skin were randomized to either a 12-week open trial regimen of 100 mg PBE supplementation once daily or to a parallel-group trial regimen of 40 mg PBE supplementation once daily.
Results
A significant decrease in clinical grading of skin photoaging scores was observed in both time courses of 100 mg daily and 40 mg daily PBE supplementation regimens. A significant reduction in the pigmentation of age spots was also demonstrated utilizing skin color measurements.
Conclusion
Clinically significant improvement in photodamaged skin could be achieved with PBE. Our findings confirm the efficacy and safety of PBE.
Introduction
French maritime pine bark extract (Pinus maritima, PBE) is a complex mixture of bioflavonoids, with oligometric proanthocyanidins (OPCs) as the major constituents. OPCs are dimers or oligomers of catechin, epicatechin, and their gallic acid esters. The major OPCs in PBE are proanthocyanidin B1 (epicatechin-(4β→8)-catechin), catechin, and epicatechin.Citation1
The process of concentrative extraction of OPCs from pine bark was established by Masquelier et al in 1948.Citation2 OPCs are found in a wide range of other plants, including common foods in an ordinary diet,Citation3,Citation4 and are widely consumed as antioxidant supplements. Recent research has focused primarily on the clinical efficacy of PBE, including a wide range of cardiovascular benefits.Citation5,Citation6 In addition to their antioxidant properties, PBE has been reported to lower blood pressure and to improve glycemic control, the lipid profile, fatty acid synthesis, and the peripheral circulation.Citation7
Skin aging is accelerated on sun-exposed areas.Citation8 Solar ultraviolet radiation is a key factor in the photoaging process of human skin. Ultraviolet radiation generates reactive oxygen species (ROS) and thus leads to oxidative stress. To counteract the harmful effects of oxidative damage by ROS, the skin is naturally equipped with ultraviolet inducible/adaptive antioxidant systems that have evolved to quench intracellular ROS, and consist of a variety of low molecular weight antioxidants (vitamins C and E) and intrinsic antioxidant enzymes for ROS-scavenging activity.Citation9,Citation10 However, antioxidant mechanisms are not completely efficient and their limitations become gradually more pronounced during aging. The end result of this process is an imbalance in cellular redox homeostasis, causing indiscriminate oxidative damage to a wide range of biomolecules.Citation11 Oxidative stress induces proinflammatory cytokines, which in turn increase intracellular levels of ROS.Citation12 Consequently, there is an ageassociated augmentation in both ROS production and in levels of oxidized/degraded proteins.Citation13,Citation14
Localized hyperpigmented lesions recognized as “age spots” are the most visible alterations in photoaged Asian skin.Citation15 They are clinically diagnosed as solar lentigines, and are frequently associated with mottled pigmentation and slight keratosis.Citation16 To date, almost all standard protocols for treating age spots are topical therapies.Citation17,Citation18 Taking photoaging and ultraviolet defense mechanisms into consideration, an oral antioxidant treatment is thought to be an effective option. Orally administered vitamins or botanical polyphenols demonstrate ultraviolet-protective properties in the skin.Citation19–Citation21 OPCs have been reported to be the strongest quenchers of ROS among the various antioxidants.Citation22 Therefore, PBE is expected to prevent photoaging and to improve the appearance of photodamaged skin.
PBE has been used as a food ingredient for thousands of years because of its safety and astringent taste. PBE and other OPC products, such as grape seed extracts, are now widely used as dietary supplements. Extensive research conducted with various formulations of PBE has already established its safety and tolerability for long-term human consumption.Citation23 However, an aqueous green tea extract supplement, which is another popular food source of polyphenols, has recently been reported to have the potential to induce liver failure.Citation24,Citation25 Such adverse reactions appear to happen more often in European countries and in Canada, when high-dose green tea extracts are taken orally for a long time,Citation26–Citation29 although green tea is consumed widely in Japan, China, and other Asian nations, and is becoming more popular in Western nations.
Taking these findings into consideration, in addition to dermatological testing of the efficacy of PBE, we characterized its hepatic safety and efficacy in the improvement of glycemic control and the plasma lipoprotein profile, as was recently shown in animal studies.Citation30 We performed total blood assays, including liver function and cholesterol blood tests. The primary purpose of this study was to evaluate the clinical efficacy and safety of French maritime PBE for improvement of photodamaged facial skin in a randomized trial of oral supplementation with PBE.
Materials and methods
French maritime PBE
French maritime PBE (Flavangenol®) was provided by Toyo Shinyaku Inc, Tosu City, Saga, Japan. Flavangenol is a registered trademark in Japan, and the trademark Toyo-FVG® has been registered in the US.
Patients
We enrolled 112 healthy women younger than 60 years with age spots, mostly diagnosed as solar lentigines, and multiple symptoms of photodamaged skin, including mottled pigmentation, roughness (including dry flaky skin), wrinkles, and swelling. All women enrolled in this study had mild to moderate facial photodamage graded on the Glogau scale between II and III and Fitzpatrick skin phototypes III to IV. After approval by the institutional ethics committee of Fukuoka University, which adheres to the principles of the Declaration of Helsinki, informed consent was obtained from all participants in the study. None of the subjects took topical/systemic retinoids, health food supplements, oral medications such as hormone replacement therapy, or topical medications, or were pregnant 4 weeks prior to enrolling in this study.
Study design
Because of the seasonal fluctuation in daily doses of ultraviolet radiation, all clinical trials were started in December to minimize the influence of seasonal skin changes, such as sun tanning and the darkening of age spots due to environmental ultraviolet light exposure. In order to assess the time course of changes in photoaging scores, clinical assessments were conducted at baseline (study day 1) and every 4 weeks thereafter.
Twenty-four women were enrolled in an open-label, high-dose PBE trial and were treated with 100 mg/day PBE for 12 weeks, while a further 88 women were enrolled in part 1 of a separate low-dose trial and treated with PBE 40 mg/day for a total of 24 weeks in an open-label, randomized, parallel-group comparative fashion. The time course of the low-dose PBE trial is shown in , in which randomization of subjects into groups 1 and 2 was performed using a computer-generated random number table. Allocation to group 1 or group 2 was done by opening the next sequentially numbered, sealed, opaque envelope. Group 1 participants were asked to take PBE 40 mg/day once daily, and to use a cleanser and sunscreen for 24 weeks throughout part 1 of the study. Group 2 participants were merely placed under observation without taking PBE for the first 12 weeks before starting oral treatment with PBE 40 mg/day once daily for the next 12 weeks, and were instructed to use a cleanser and sunscreen for 24 weeks throughout part 1 of the study.
Figure 1 Schematic outline of part 1 and part 2 of study using low-dose pine bark extract.
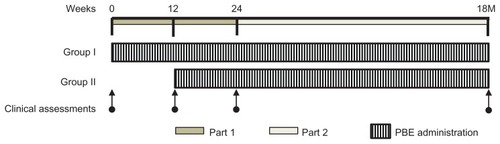
We compared the improvement between subjects who received oral PBE for 24 weeks (group 1) and those who received only 12 weeks of treatment (group 2), corresponding to the latter half of the 24-week treatment period for group 1. At the end of part 1 of the low-dose study, 24 subjects were instructed to take PBE for a further 12 months (part 2 of the study) to evaluate the long-term efficacy and safety of PBE ().
Subjective assessments
The subjects completed a self-assessment questionnaire concerning their facial skin on a scale of 0 to 5 of increasing severity for the following criteria: pigmentation, wrinkles, roughness, dryness, and overall improvement. Each patient was asked to complete a self-assessment questionnaire at the final visit of each study, ie, after 12 weeks of treatment in the high-dose PBE trial or 24 weeks after completing part 1 of the low-dose trial. If a patient checked the “unknown” option, their results were excluded from statistical analysis.
Three board-certified dermatologists subjectively graded the subjects for clinical symptoms, ie, solar lentigines, mottled pigmentation, roughness (including dry/flaky skin), wrinkles, and swelling, based on a standardized assessment scale using photographs, after which an overall evaluation of the results was performed. All assessors remained unaware of subject treatment assignment throughout the trial.
Objective measurements
At each visit, the melanin index of the age spots was evaluated using a method described in a previous report.Citation31 A colorimeter (CR-13, Konica-Minolta, Tokyo, Japan) was used to record facultative forehead skin color by calculating individual typology angle (ITA) degrees, as described elsewhere.Citation32 Fluctuation of facultative skin color was quantified in groups 1 and 2 during part 1 of the low-dose trial. In order to assess for any age-related decrease in epidermal keratinocyte turnover, we planimetrically measured the mean area of tape-stripped, basic fuchsin crystal violet-stained corneocytes by digital image analysis.
Safety assessments
Fasting (10 hours) blood samples were collected from all enrolled subjects on day 0 and after 12 weeks (high-dose trial only), and at 24 weeks and 18 months from the start of the trials for routine hematology, blood chemistry, and urine investigations. A lipid panel measuring high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, triglycerides, and free fatty acids was used to assess the plasma lipoprotein cholesterol profile. Routine hematology tests and examination of serum iron/ferritin levels were used to detect iron deficiency anemia. Aspartate aminotransferase and alanine aminotransferase levels were used to assess the safety of PBE with respect to its potential liver toxicity. Assessment of these tests was conducted by an outside laboratory (BML Inc, Tokyo, Japan). Body weight measurements and body fat percentage assessments were performed for all subjects in the low-dose trial.
Data analysis
All statistical calculations were performed using StatView for Windows, version 5.0.1 (SAS Institute Inc, Cary, NC). The data are presented as the mean ± standard deviation, unless otherwise specified. An unpaired t-test or Mann–Whitney U test was used to compare subjects when equal variance was shown by the F-test or when equal variance was not shown, respectively. For clinical assessments, the Wilcoxon signed-rank test for related samples was used in a time course of trials, and the Mann–Whitney U test was used for comparing the two treatment groups. A two-tailed, independent t-test was performed for grading of clinical assessments, with P values noted. Either Dunnett’s test or the Tukey–Kramer method was used to compare the means of the melanin index at each point during the observational study, with P values noted. Clinical laboratory test results were analyzed statistically using a Student’s two-tailed paired t-test.
Results
Demographics
Twenty-four subjects aged 31–59 (mean 36.9 ± 6.6) years completed 12 weeks of treatment with PBE 100 mg/day in the high-dose trial. Eighty-eight subjects enrolled into part 1 of the 24-week, low-dose, comparative study, and 77 (n = 38 in group 1, n = 39 in group 2) completed the 24-week treatment program and had data available for statistical analysis. The mean age at study entry was 36.7 ± 7.9 years. The background details of the subjects are shown in . There was no significant difference in background features (age or facultative skin color) at study entry between the two groups, suggesting adequate randomization. There were no clinically meaningful differences in laboratory tests or body measurements at study entry. Eleven withdrawals occurred because of poor compliance, amongst which no adverse events were reported. Twenty-four subjects participated in the 18-month part 2 phase of the study, consisting of 15 subjects from group 1 and nine subjects from group 2 who completed the 24-week study and had long-term data available for statistical analysis. Their mean age at study entry was 37.2 ± 4.4 years. Three dropouts occurred because of poor compliance, for whom no adverse events were reported.
Table 1 Baseline demographics of randomized groups (phase I, low-dose PBE trial)
Subjective efficacy assessment
In the high-dose trial, the questionnaire survey about subjective facial symptoms showed that a relatively large number of subjects felt that their facial skin roughness, including dry skin, had improved (). Multiple digital image assessments made by the dermatologists showed that 71% of participants had significant improvement of their age spots.
Table 2 Score assessments of questionnaire survey (high-dose PBE trial, N = 24)
The percentage of group 1 subjects in part 1 of the low-dose trial who answered that their skin symptoms generally became better after starting oral PBE was around 30%, and this number was much larger than that for subjects who felt that their condition was aggravated after 24 weeks (). A similar trend was seen for group 2 patients in the questionnaire, especially those related to facial photoaging symptoms after 24 weeks (). In part 2 of the low-dose trial, over 40% of participants in groups 1 and 2 answered that their photoaging symptoms, including solar lentigines and mottled pigmentation, had improved after 18 months as compared with baseline ().
Table 3A Score assessments of questionnaire survey for group I (phase I, low-dose PBE trial, N = 38)
Table 3B Score assessments of questionnaire survey for group II (phase I, low-dose PBE trial, N = 39)
Table 4 Score assessment of questionnaire survey for 18-month PBE administration (phase II, low-dose PBE trial, N = 21)
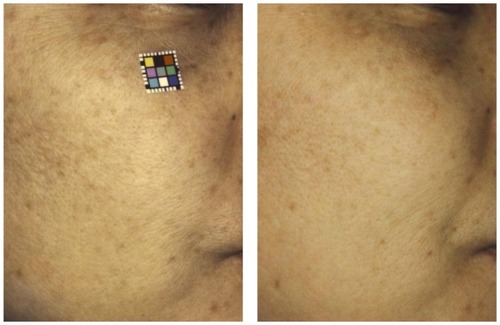
In part 1 of the low-dose trial, photoaging scores in group 1 as assessed by dermatologists after 12 weeks of PBE were compared with those at the beginning of the study. Scores for solar lentigines, mottled pigmentation, roughness, wrinkles, and swelling showed significant improvement at 12 weeks. Scores for solar lentigines, mottled pigmentation, wrinkles, and swelling were significantly improved (). Representative clinical images of a typically improved case before and after PBE are shown in . In Group 2, there were no significant improvements in scores seen 12 weeks after initial observation as compared with scores before treatment. However, after 24 weeks of treatment, which consisted of a 12-week PBE treatment period following a 12-week observation-only period, scores for solar lentigines, mottled pigmentation, and roughness had significantly improved ().
Table 5 Physical examination scores (phase I, low-dose PBE trial)
Figure 2 Before (left) and 6 months after (right) treatment of photodamaged skin with oral pine bark extract.
By comparing the scores between the two groups in part 1 of the low-dose trial, 12 weeks after the initial observation, scores for solar lentigines and skin roughness in part 1 showed significant improvement over those in group 2 () during part 2 of the low-dose trial. All 21 cases showed significantly better scores for solar lentigines, mottled pigmentation, roughness, wrinkles, and swelling compared with those at the end of part 1 (). For part 1 of the low-dose trial, the overall rating for the therapeutic index achieved with low-dose PBE is summarized in . An efficacy rating of slightly improved or better was recorded for 87% of subjects in group 1 and 72% in group 2. In part 2 of the trial, significant overall improvements were recorded for all 21 subjects ().
Table 6 Physical examination scores (phase II, low-dose PBE trial, N = 21)
Table 7A Overall efficacy rate after 24-week low-dose PBE administration (phase I, low-dose PBE trial)
Table 7B Overall efficacy rate after 18-month low-dose PBE administration (phase II, low-dose PBE trial)
Objective measurements
Time course of melanin pigmentation in age spots
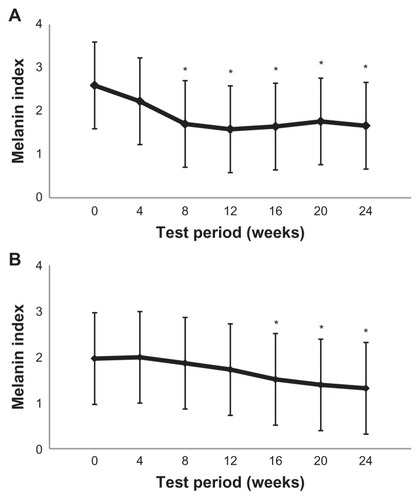
The melanin index was calculated from the L*a*b* values for each digital image of an age spot. In the high-dose trial, the average melanin index of the age spots gradually decreased from baseline over the 12 weeks. A significant decrease in average melanin index scores at weeks 4 and 12 was confirmed using the Tukey–Kramer method (). Twenty- one of the 88 subjects were followed in the low-dose trial. A significant decrease in average melanin index was observed in both groups, with the melanin index scores in group 1 being significantly lower than at baseline between weeks 8 and 24 (P < 0.05), while in group 2, mean melanin index scores were significantly decreased between weeks 16 and 24 (week 16 corresponds to 4 weeks after starting PBE in group 2, ).
Figure 3 The melanin index was significantly decreased after 4 and 12 weeks of oral administration of pine bark extract 100 mg/day.
Notes: The melanin index was calculated according to the method reported by Yamamoto et al.Citation31 Values are expressed as the mean ± standard deviation. *P < 0.05 (Tukey–Kramer method), n = 24.
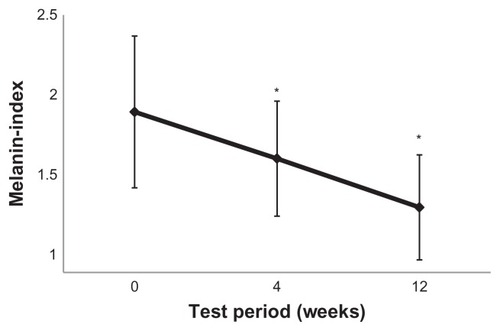
Figure 4 Time course of mean melanin index changes in age spots in group 1 (A) and group 2 (B).
Effects of PBE on facultative facial skin color
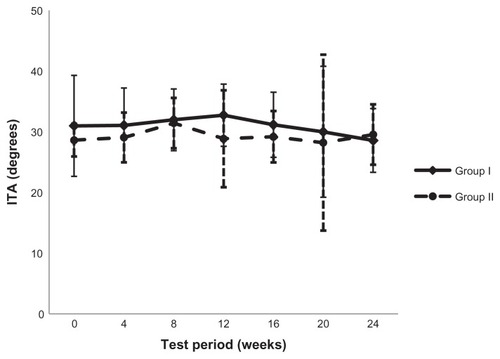
During parts 1 and 2 of the low-dose trial, the whitening effects of PBE on facultative facial skin color were evaluated by average ITA degrees chronologically obtained from a colorimetric assay of forehead skin color. Although the ITA values fluctuated in groups 1 and 2 throughout the study, the average ITA values did not show an overall trend towards lighter values with respect to facial complexion ().
Figure 5 Facultative skin color was assessed using a colorimeter followed by individual typology angle value calculation.
Abbreviation: ITA, individual typology angle.
Effects of PBE on corneocyte size
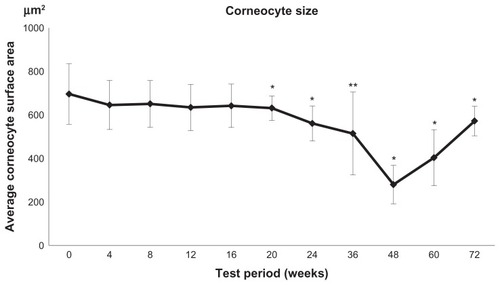
We found a statistically significant reduction in the size of corneocytes in the surface layers of the skin during PBE administration for longer than 5 months, corresponding to the latter periods of parts 1 and 2 in the low-dose trial. This suggests that PBE helped to repair existing skin damage, considering that corneocyte size usually increases with aging ().
Figure 6 Time course of corneocyte size changes measured by a planimetric method during pine bark extract administration.
Safety and tolerability
In the high-dose trial, mean corpuscular volume demonstrated a significant change of values after 12 weeks, but the change was within the normal range. No other hematological parameters showed significant changes (). In the low-dose trial, mean corpuscular hemoglobin showed a significant change of values in group 2 after 24 weeks, but this value change was within the normal range. No other data showed significant changes ().
Table 8A Results of hematology in 24 evaluated cases (high-dose PBE trial, 12-week administration)
Table 8B Results of hematology in 21 evaluated cases (phase II, low-dose PBE trial, 18-month administration)
In the high-dose trial, blood chemistry tests demonstrated significant changes in serum sodium and chloride after 12 weeks of treatment with PBE. There were no other significant changes in blood chemistry parameters ().
Table 9A Results of blood chemistry in 24 evaluated cases (high dose PBE trial, 12-week administration)
Significant changes were observed in aspartate aminotransferase in group 1 in the low-dose trial, 24 weeks after oral administration. In group 2, after 15–18 months of treatment with PBE, serum potassium concentrations changed significantly. However, these were both minor fluctuations within the normal range. Other test values, including glycemic control and plasma lipoprotein profile, did not show any significant changes at 18 months (). Urine examination was entirely normal (data not shown).
Table 9B Results of blood chemistry in 21 evaluated cases (phase II, low-dose PBE trial, 18-month administration)
No significant changes in body weight or body fat percentage were observed during the test period (data not shown). No adverse events were reported during the study, and the tolerability of PBE was deemed to be acceptable. PBE was considered to be systemically safe based on hematology and biochemistry. Although slight but significant fluctuations in the data were observed for some parameters, all values were within the normal biological ranges.
Discussion
We examined the efficacy of PBE in the treatment of photodamaged facial skin, and significant improvement was suggested from multiple dermatological score assessments during this study. A subject questionnaire concerning subjective facial symptoms demonstrated that a relatively large number of subjects felt that the roughness of their facial skin had improved in the high-dose trial. Although improvement in age spots was only recognized by a relatively small number of subjects in the high-dose trial, detailed evaluation of digital images revealed that 71% of participants had improvement of their age spots, albeit to a varying extent. In part 1 of the low-dose trial, there was significant improvement in scores for solar lentigines, mottled pigmentation, skin roughness, and swelling only when subjects were on treatment with PBE. Further, subjects treated with PBE had significantly lower scores for solar lentigines and skin roughness when compared with the untreated patients. Therefore, we consider that both the high-dose and low-dose arms in this study demonstrate a similar trend of improvement in symptoms of photodamaged facial skin. Further significant improvements were seen during the long-term 18-month study (part 2 of the low-dose trial) in almost every photoaging score. This improvement was maintained and enhanced by continuous administration of PBE over a long period. Finally, 72% of the subjects receiving PBE for 12 weeks (group 2) showed improvement versus 87% of those receiving PBE for 24 weeks (group 1). All subjects who completed treatment with PBE for 15–18 months showed improvement in symptoms. In line with the score assessment results, objective biophysical measurements demonstrated a significant gradual decrease in average melanin index during treatment with PBE in both trials.
In an earlier safety evaluation, PBE showed excellent overall tolerability without any side effects.Citation33 Health concerns about prolonged administration of OPCs, such as iron and/or methionine deficiency,Citation34 were ruled out after it was found that there was no abnormal nutritional sequelae, including iron deficiency anemia, elevated cholesterol readings, or liver damage.
In an earlier study of treatment of photoaged skin with oral polyphenols,Citation35 a popular polyphenol-rich green tea extract containing (−)-epigallocatechin gallate (EGCG) was used. Although facial photoaging scores improved on treatment with the green tea extract for the first 12 months, there was no significant antiphotoaging effect after 24 months of treatment. In contrast, gradual improvement of photoaging scores even at 18 months was confirmed in our PBE trial. Demographic diversity in subject age and race might account for the different results seen in these two studies. The mean age of the subjects in the previous study was around 12 years older than in our study, so a less favorable outcome would be expected because of the exponential decline of intrinsic antioxidative potency in the elderly. Our findings in Japanese women might be positively biased by a racial difference, ie, age spots in East Asians often appear as early as in the 20 s and 30 s, while age spots in Caucasians tend to become apparent between the ages of 50 and 60 years.Citation36
The EGCG used in the previous trial was a prodel-phinidin- type flavonoid that also acts as a pro-oxidant, with production of active superoxide radical anions.Citation37 EGCG is beneficial in chemoprevention because of its pro-oxidant nature, and it works as a PI3K/AKT/mTOR pathway inhibitor, triggering apoptosis of cancer cells.Citation38,Citation39 However, this action might cause a pro/antioxidant cellular imbalance and aggravate photoaging of the skin. In contrast, such undesirable effects on the skin are much less likely to occur with (−)-epicatechin, (+)-catechin, or procyanidin-type polymers, that are the main constituents of the OPCs in PBE.
In the skin, PBE has been found to protect capillary wallsCitation40 and to inhibit matrix metalloproteinases.Citation41 Direct assessment of the antioxidant effects of PBE by electron spin resonance spectroscopy showed that PBE had significant antioxidant effects on the facial skin of ultraviolet B-irradiated hairless mice in vivo.Citation1 OPCs have also been reported to be effective inhibitors of tyrosinase in skin-derived melanocytes and in the hyperpigmented skin of ultraviolet-irradiated mice and guinea pigs.Citation42–Citation45 Oral OPC supplements are expected to have desirable effects on photoaging because they promote tissue elasticity, help heal microinjuries, reduce bruising and swelling by strengthening blood vessels, prevent postinflammatory skin pigmentation, restore dermal collagen, and improve the peripheral circulation.Citation46,Citation47 In fact, OPCs from grape seeds have previously been reported to improve melasma to a significant extent.Citation48
A white complexion is a highly desirable symbol of beauty among Asian women, who believe that it is powerful enough to hide a number of faults. PBE did not modify facultative skin color in our trial, suggesting that the skin lightening elicited by PBE is confined to solar lentigines that appear with chronic inflammation, and can persist long after exposure to ultraviolet light. Recent profiling of solar lentigines with cDNA microarrays and immunohistochemical assays revealed a number of upregulated genes for the enzymes that synthesize arachidonic acid, as well as melanogenic and inflammatory genes in those lesions.Citation49
Nuclear factor E2-related factor 2 (Nrf2)/antioxidative response element-mediated phase 2 detoxifying/antioxidant enzymes are induced by OPCs,Citation50 so OPC-activated Nrf2 confers protection against ultraviolet-induced skin inflammation. Citation51 OPCs are expected to be potent suppressors of expression or activity of genes in the melanogenic, inflammatory, and arachidonic acid-synthesizing categories downstream of Nrf2.Citation52,Citation53 Interestingly, the arachidonate 12-lipoxygenase gene (ALOX), which is locally upregulated in solar lentigines,Citation49 may be downregulated by treatment with oral OPCs in mice.Citation54
Another possible lightening mechanism, ie, acceleration of epidermal turnover, is suggested by the significant reduction in corneocyte size by PBE. PBE induces a gentle yet sufficiently effective exfoliating action in the skin to promote release of excess epidermal melanin deposition.Citation55,Citation56
Conclusion
Oral administration of French maritime PBE effectively reduces facial symptoms of photoaging. Long-term administration of PBE is safe and useful for improving the appearance of photodamaged facial skin.
Disclosure
This research was supported by a research grant from Toyo Shinyaku Co, Ltd, Tosu City, Saga, Japan. Toyo Shinyaku Co, Ltd, provided study tablets similar to the TOYO-PBE tablets marketed in the US. Otherwise, the authors report no conflict of interest in this work.
References
- YoshidaAYoshinoFTsubataMIkeguchiMNakamuraTLeeMCDirect assessment by electron spin resonance spectroscopy of the antioxidant effects of French maritime pine bark extract in the maxillofacial region of hairless miceJ Clin Biochem Nutr2011492798621980222
- MasquelierJMichaudJLaparraJDumonMCFlavonoids and pycnogenolsInt J Vitam Nutr Res1979493307311528157
- HammerstoneJFLazarusSAMitchellAERuckerRSchmitzHHIdentification of procyanidins in cocoa (Theobroma cacao) and chocolate using high-performance liquid chromatography/mass spectrometryJ Agric Food Chem199947249049610563922
- CansfieldPEMarquardtRRCampbellLDCondensed proanthocyanidins of fababeansJ Sci Food Agric19803188028127453148
- AnejaRHakePWBurroughsTJDenenbergAGWongHRZingarelliBEpigallocatechin, a green tea polyphenol, attenuates myocardial ischemia reperfusion injury in ratsMol Med2004101–6556215502883
- DieboltMLaflammeKLabbeRAugerFAGermainLAndriantsitohainaRPolyphenols modulate calcium-independent mechanisms in human arterial tissue-engineered vascular mediaJ Vasc Surg200746476477217764876
- MaimoonaANaeemISaddiqeZJameelKA review on biological, nutraceutical and clinical aspects of French maritime pine bark extractJ Ethnopharmacol2011133226127721044675
- FisherGJKangSVaraniJMechanisms of photoaging and chronological skin agingArch Dermatol2002138111462147012437452
- GasperlinMGosencaMMain approaches for delivering antioxidant vitamins through the skin to prevent skin ageingExpert Opin Drug Deliv20118790591921599565
- DreherFMaibachHProtective effects of topical antioxidants in humansCurr Probl Dermatol20012915716411225195
- JunqueiraVBBarrosSBChanSSAging and oxidative stressMol Aspects Med2004251–251615051312
- LaneNA unifying view of ageing and disease: the double-agent theoryJ Theor Biol2003225453154014615212
- LuCYLeeHCFahnHJWeiYHOxidative damage elicited by imbalance of free radical scavenging enzymes is associated with large-scale mtDNA deletions in aging human skinMutat Res19994231–2112110029667
- StadtmanERLevineRLProtein oxidationAnn N Y Acad Sci200089919120810863540
- Nouveau-RichardSYangZMac-MarySSkin ageing: a comparison between Chinese and European populations. A pilot studyJ Dermatol Sci200540318719316154324
- HolzleEPigmented lesions as a sign of photodamageBr J Dermatol1992127Suppl 4148501390186
- GillbroJMOlssonMJThe melanogenesis and mechanisms of skin-lightening agents – existing and new approachesInt J Cosmet Sci201133321022121265866
- PinnellSRCutaneous photodamage, oxidative stress, and topical antioxidant protectionJ Am Acad Dermatol200348111912522365
- Eberlein-KonigBPlaczekMPrzybillaBProtective effect against sunburn of combined systemic ascorbic acid (vitamin C) and d-alphatocopherol (vitamin E)J Am Acad Dermatol199838145489448204
- StahlWSiesHCarotenoids and flavonoids contribute to nutritional protection against skin damage from sunlightMol Biotechnol2007371263017914160
- MittalAElmetsCAKatiyarSKCD11b+ cells are the major source of oxidative stress in UV radiation-irradiated skin: possible role in photoaging and photocarcinogenesisPhotochem Photobiol200377325926412685652
- AfaqFMukhtarHBotanical antioxidants in the prevention of photocarcinogenesis and photoagingExp Dermatol200615967868416881964
- DrielingRLGardnerCDMaJAhnDKStaffordRSNo beneficial effects of pine bark extract on cardiovascular disease risk factorsArch Intern Med2010170171541154720876405
- SarmaDNBarrettMLChavezMLSafety of green tea extracts: a systematic review by the US PharmacopeiaDrug Saf200831646948418484782
- FrankJGeorgeTWLodgeJKDaily consumption of an aqueous green tea extract supplement does not impair liver function or alter cardiovascular disease risk biomarkers in healthy menJ Nutr20091391586219056646
- GalatiGLinASultanAMO’BrienPJCellular and in vivo hepatotoxicity caused by green tea phenolic acids and catechinsFree Radic Biol Med200640457058016458187
- FedericoATisoALoguercioCA case of hepatotoxicity caused by green teaFree Radic Biol Med200743347417602963
- Jimenez-SaenzMMartinez-SanchezCGreen tea extracts and acute liver failure: the need for caution in their use and diagnostic assessmentLiver Transpl2007137106717600357
- Jimenez-SaenzMdel Martinez-SanchezMCAcute hepatitis associated with the use of green tea infusionsJ Hepatol200644361661716427718
- SugayaKIgarashiMKojimaYTsubataMNagaokaIEvaluation of the effect of flavangenol on serum lipid peroxide levels and development of atherosclerosis in spontaneously hyperlipidemic B6. KOR-Apoeshl miceInt J Mol Med2011271333821069260
- YamamotoTTakiwakiHAraseSOhshimaHDerivation and clinical application of special imaging by means of digital cameras and Image J freeware for quantification of erythema and pigmentationSkin Res Technol2008141263418211599
- ParkSBSuhDHYounJIA long-term time course of colorimetric evaluation of ultraviolet light-induced skin reactionsClin Exp Dermatol199924431532010457139
- RohdewaldPA review of the French maritime pine bark extract (Pycnogenol), a herbal medication with a diverse clinical pharmacologyInt J Clin Pharmacol Ther200240415816811996210
- MennenLIWalkerRBennetau-PelisseroCScalbertARisks and safety of polyphenol consumptionAm J Clin Nutr200581Suppl 1326S329S15640498
- ChiuAEChanJLKernDGKohlerSRehmusWEKimballABDouble-blinded, placebo-controlled trial of green tea extracts in the clinical and histologic appearance of photoaging skinDermatol Surg2005317 Pt 285586016029678
- GohSHThe treatment of visible signs of senescence: the Asian experienceBr J Dermatol1990122Suppl 351051092337528
- MeagherLPSpencerPLaneGASivakumaranSFraserKWhat do green tea, grapes seeds, and docks have in common?Chem N Z20056934
- NakasoKYanoHFukuharaYTakeshimaTWada-IsoeKNakashimaKPI3K is a key molecule in the Nrf2-mediated regulation of antioxidative proteins by hemin in human neuroblastoma cellsFEBS Lett20035462–318118412832036
- Van AllerGSCarsonJDTangWEpigallocatechin gallate (EGCG), a major component of green tea, is a dual phosphoinositide-3- kinase/mTOR inhibitorBiochem Biophys Res Commun2011406219419921300025
- BelcaroGCesaroneMRRicciAControl of edema in hypertensive subjects treated with calcium antagonist (nifedipine) or angiotensin-converting enzyme inhibitors with PycnogenolClin Appl Thromb Hemost200612444044417000888
- GrimmTSchaferAHoggerPAntioxidant activity and inhibition of matrix metalloproteinases by metabolites of maritime pine bark extract (pycnogenol)Free Radic Biol Med200436681182214990359
- ShojiTMasumotoSMoriichiNProcyanidin trimers to pentamers fractionated from apple inhibit melanogenesis in B16 mouse melanoma cellsJ Agric Food Chem200553156105611116029003
- ZhuWGaoJThe use of botanical extracts as topical skin-lightening agents for the improvement of skin pigmentation disordersJ Investig Dermatol Symp Proc20081312024
- HanamuraTUchidaEAokiHSkin-lightening effect of a polyphenol extract from Acerola (Malpighia emarginata DC) fruit on UV-induced pigmentationBiosci Biotechnol Biochem200872123211321819060403
- YamakoshiJOtsukaFSanoALightening effect on ultraviolet-induced pigmentation of guinea pig skin by oral administration of a proanthocyanidin-rich extract from grape seedsPigment Cell Res200316662963814629720
- ManachCWilliamsonGMorandCScalbertARemesyCBioavailability and bioefficacy of polyphenols in humans. I. Review of 97 bioavailability studiesAm J Clin Nutr200581Suppl 1230S242S15640486
- WilliamsonGManachCBioavailability and bioefficacy of polyphenols in humans. II. Review of 93 intervention studiesAm J Clin Nutr200581Suppl 1243S255S15640487
- YamakoshiJSanoATokutakeSOral intake of proanthocyanidin-rich extract from grape seeds improves chloasmaPhytother Res2004181189589915597304
- AokiHMoroOTagamiHKishimotoJGene expression profiling analysis of solar lentigo in relation to immunohistochemical characteristicsBr J Dermatol200715661214122317419692
- BakMJJunMJeongWSProcyanidins from wild grape (Vitis amurensis) seeds regulate ARE-mediated enzyme expression via Nrf2 coupled with p38 and PI3K/Akt pathway in HepG2 cellsInt J Mol Sci201213180181822312287
- SawCLHuangMTLiuYKhorTOConneyAHKongANImpact of Nrf2 on UVB-induced skin inflammation/photoprotection and photoprotective effect of sulforaphaneMol Carcinog201150647948621557329
- HirotaAKawachiYYamamotoMKogaTHamadaKOtsukaFAcceleration of UVB-induced photoageing in nrf2 gene-deficient miceExp Dermatol201120866466821569103
- GescherAGerhauserCCancer chemopreventive agents in plants – a continuing challengePlanta Med200874131523152518843591
- ShenGXuCHuRComparison of (−)-epigallocatechin-3-gallate elicited liver and small intestine gene expression profiles between C57BL/6J mice and C57BL/6J/Nrf2 (−/−) micePharm Res200522111805182016132347
- IriyamaSOnoTAokiHAmanoSHyperpigmentation in human solar lentigo is promoted by heparanase-induced loss of heparan sulfate chains at the dermal-epidermal junctionJ Dermatol Sci201164322322822005029
- ChenNHuYLiWHThe role of keratinocyte growth factor in melanogenesis: a possible mechanism for the initiation of solar lentiginesExp Dermatol2010191086587219780816