Abstract
Lips and the perioral area are of outstanding importance in youthful appearance, attractiveness, and beauty. In contrast to younger and middle aged females, there is only scant published data on minimally invasive procedures to restore and revitalize lips and perioral soft tissue in elderly females. In this review we report the signs of aging in this particular region and the underlying anatomy. We review studies on lip restoration in younger females and present our techniques for elderly women. With an individually tailored approach, elderly females benefit from minimally invasive techniques.
Introduction
Lips are a central part of facial aesthetics due to their color, surface texture, and shape. Well defined and full lips represent attractiveness and beauty. Loss of volume and elasticity of subcutaneous soft tissue, retraction of lip red, bone resorption, loss of teeth, smoking, and ultraviolet exposure contribute to perioral aging and loss of attractiveness. Furthermore, lips are exposed to irritants and environmental factors that challenge the barrier function of their thin horny layer. The lips are conceived as signs of aging, loss of attractiveness, and fragility.Citation1
Lips are part of the aesthetic unit that involves the mouth and the perioral tissue. Aging of this area is characterized by perioral fine lines, marionette lines, and flattening of the cupid bow. The philtrum becomes longer and ill defined, indirectly contributing to a thinner upper lip.Citation2 Furthermore, the dynamics of lip movement change with age. The smile, for instance, gets narrower vertically and wider transversely. People older than 50 years of age lose their ability of a high smile.Citation3
Skin and lip care may help to preserve a youthful and healthy appearance.Citation4,Citation5 Dentistry plays a significant role in restoring perioral and mouth aesthetics, not only in elderly people.Citation6 Restorative techniques of the perioral soft tissue will further enhance the aesthetic outcome of aesthetic restorative dentistry.Citation7
In our review, we will focus on minimally invasive procedures such as dermal filler injection and botulinum toxin A application in women 50 years of age and older. All procedures need a detailed knowledge of anatomy, pharmacology, and technical skills to be safe for patients. The usual medical background is dermatology or plastic surgery. Although the legal situation can vary between countries, attendance of certified courses and workshops by medical societies is highly recommended. This does not, however, replace personal technical skills.
Anatomy
The mandible, maxillary bone, and teeth represent the hard tissue structures that will shape the perioral area and the mouth (). Aging affects these structures. Maxillary retrusion of the maxilla is evident in both fully dentated patients and those with loss of teeth. Deepening of the maxilla supports a posterior positioning of the upper lip and the nasolabial fold.Citation8 Three dimensional computed tomography (CT) demonstrated that mandibular height and length decrease with age.Citation9
Figure 1 Anatomy of upper and lower lip region.
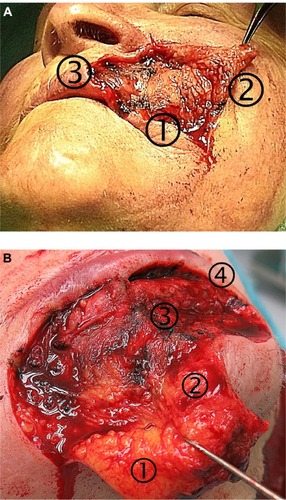
The perioral muscles are arranged in several layers. The orbicularis oris muscle interlaces with perioral muscles, influencing the dynamic actions during speech, smiling, and whistling. On the apical area, fibers of the levator labii superioris insert into the upper lip and the oral sphincter. Laterally, the levator anguli oris and both zygomaticus muscles insert into the upper lip. The risorius muscle and depressor anguli oris insert into the corner of the mouth. The depressor anguli oris is the most superficial mimetic muscle. The lower lip is inserted by the depressor labii inferioris and mentalis, with mentalis also inserting into chin dermis. Both interlace with platysma fibers. Perioral muscles have a different nerve supply from the zygomatic and buccal branches of the facial nerve (zygomaticus, levator anguli oris, levator labii superioris, and part of orbicularis oris), and marginal branches of the facial nerve (part of orbicularis oris, depressor anguli oris, mentalis).Citation10
Superficial fat compartments are arranged in the perioral area. The jowl compartment above the mandible and the nasolabial compartment can influence the lateral upper lip and the corners of the mouth.Citation11 Facial fat is divided into deep and superficial planes. The perioral fat is characterized by a deep department beneath mentalis and orbicularis oris muscles different from small lobuled superficial fat of the lips. The wet–dry transition zone of the lips defines the most anterior border of the submuscular deep fat tissue.Citation12 Cadaveric studiesCitation13 of perioral soft tissue demonstrated a lipomatous area without defined ligamentous attachment. The perioral mound with a scaffold of fine trabecular fibrouse separations defines a separate fat pad compartment. With aging it becomes lipodystrophic and ptotic.Citation13
Deep fat depots have been defined under the melomental (marionette) line. Since these depots are surrounded by retaining ligaments (condensations of fibrous tissue), this may affect volumizing procedures.Citation14 The philtrum is characterized by a fat compartmentation by delicate membranes related to its particular vascular anatomy.Citation15
Sensory innervation of the perioral skin arises from infraorbital nerve branches (upper lip and philtrum), the buccal nerve (corners of the mouth), and the mental nerve (lower lip and chin).Citation10
Grading scales for perioral lines and lip fullness
There is no doubt about the need for validated grading scales to measure effects of aging and objective evaluations of therapeutic trials. A validated 5-point photonumeric lip scale, the lip fullness scale (LFS) has been developed by Carutthers et al.Citation16 Separate grading for upper and lower lips is recommended. The scale ratings are: very thin (0), thin (1), moderately thick (2), thick (3), and full (4).Citation16
The same group of international experts developed a validated grading scale for melomental folds (marionette lines), the marionette line grading scale.Citation17 The 5-point photonumeric scale differentiates no visible folds (0), visible fold with slight indentation (1), moderately deep folds not visible when skin is stretched (2), very long and deep folds (3), and extremely long and deep folds (4).Citation17
A limitation of both grading systems is that they do not address dynamic movements of the area. This is of utmost importance in normal life. There are more grading systems for the perioral area available but a detailed discussion is not the focus of this review.Citation15,Citation16
Dermal fillers
Dermal fillers can be subdivided into temporary and permanent fillers. In this article, we will focus on temporary fillers based on crosslinked hyaluronic acid (HA) fillers. This filler type consists of biphasic (particulate) and monophasic fillers (gel only).Citation17
The injection technique is dependent on the filler, area to inject, and the physician and patient preference. To reduce injection and filling related pain, topical anesthetics or nerve blocks may be used. Some fillers contain lidocain to reduce injection pain. It is possible to use either a multiple puncture technique or a threading technique. The latter needs a lesser number of needle sticks. Filling can be performed retrograde or anterograde. Needle diameter is dependent on the choice of filler. For many HA fillers, 27–30 gauge needles are used. Some investigators prefer cannulas. The injections should be done with a slow motion to reduce pain, bruising, and risk of irregularities. Cold compresses before and after the procedure increase comfort and reduce swelling and tenderness. For lip augmentation the HA filler is often placed near the border of the wet and dry lip. Bleeding, nodule formation, and temporary edema are the most frequent adverse effects.Citation18 Overcorrections and nodules can easily be corrected by injection of hyaluronidase, a big advantage compared to other filler materials.Citation19
Nonaminal stabilized HA ([NASHA] Restylane, Q-Med AB, Uppsala, Sweden) represents a particulate filler type. Restylane Perlane (Q-Med) consists of 10,000 particles/mL. Juvederm (Allergan Inc, Irvine, CA, USA), Belotero (Merz Pharma GmbH and Co, Frankfurt, Germany), Glythone (Pierre Fabre, France and Merz Pharma GmbH and Co), or Teosyal (Teoxane SA, Geneva) are monophasic fillers. Fillers also differ by HA concentration, crosslinking technology, and rheological properties.Citation18,Citation20
In an open trial,Citation21 50 female subjects were treated with a monophasic HA filler (Juverderm Ultra, Allergan Inc) for lip enhancement. Improvement was measured by the LFS. The mean injected volume was 1.6 mL. More than 90% of investigators and subjects were satisfied with the results. At week 12, 71% of subjects had an improvement of ≥1 grade on the LFS. Twelve weeks later, lip improvement was still present for 56% of subjects.Citation21
In a multicenter European trial,Citation22 60 subjects were treated with the HA filler Juvederm Vobella (Allergan). This new filler is based on a new technology called Vycross. Here, incorporation of short chain and long chain HA is used to enhance crosslinking without increasing stiffness. The Juvederm Vobella filler has an elastic modulus, G′, of about 160 Pa, which is lower when compared to other fillers like Juvederm Ultra or Restylane. This creates a smooth soft gel of 15 mg HA/mL. The mean injected volume was 1.2 mL. The improvement of ≥1 grade in the LFS was reported for 98.3% of subjects at 3 months and 48.3% of subjects at 12 months.Citation22
In two studies using biphasic, NASHA Restylane (Q-Med) covering 180 subjects and 1,446 subjects, subject satisfaction after 6 months was 70% and 50.8%, respectively.Citation23,Citation24
Our technique for perioral and lip restoration in elderly women
Selection of patients is a critical issue to ensure a satisfying aesthetic outcome. Medical history is important in the sense of allergies, bleeding disorders, neurologic or autoimmune diseases, immunodeficiencies, or iatrogenic immunosuppression. Body dysmorphic disorders are not limited to younger patients. Such subjects will be inappropriate for filler injections. Scars and history of facial surgery have to be taken into account. Medications and over the counter drugs should be recorded.Citation25
The facial mimics are studied in rest and in motion. With increasing age facial asymmetries will become more prominent. The dental status is important. The findings and the treatment options should be discussed with the patient. The mirror and camera are the most important tools to define with the patient what should be modified to obtain a better appearance.
We included females older than 49 years of age (n = 57) with a mean age of 59.2 ± 7.9 years (age range 50 to 84 years). A total of 199 procedures were performed. The average follow-up was 38 ± 11.5 months.
We used only monophasic HA dermal fillers (Belotero, Glytone, or Juvederm) with 27 or 30 gauge needles. The average amount of filler used per session was 1.6 mL. Botulinum toxin A (Vistabel, Allergan; Bocouture, Merz) was diluted in physiological sodium chloride solution according to the manufacturer’s recommendation. The median amount of botulinum toxin A units (Botox units) in the perioral area was 12 ± 8 units.
The position of the upper lip is modified by the nasolabial fold and the cheek fat pads. A minor lift of the upper lip with an improved show of the wet roll is possible by liquid lift of the cheeks (). Very thin lips, however, will not benefit from this technique.
Figure 2 A 55-year-old woman with thin lips and perioral fine lines and elongation of the philtrum.

Augmentation by filler along the vermillion border (white roll) attenuates the convexity of this area and can improve perioral fine wrinkling (). Soft filler with a lower stiffness is preferred even if the durability is more limited. Stiffer fillers would impair the delicate motion of the lips when speaking, singing, or smiling. Although injections of small amounts of botulinum toxin A are used to improve perioral lines in younger and middle aged females, we would not recommend this method for elderly subjects. Intrinsic and extrinsic aging eventually causes lines in rest that cannot be corrected by botulinum toxin.
Figure 3 A 45-year-old woman with thin lips and flat philtrum.

Figure 4 A 67-year-old woman with perioral fine lines and flattening of philtrum collumelas.

Loss of volume of the upper lips is often associated with flattening of the vermillion border and partial loss of Cupid’s bow. Subdermal injection of filler along the philtrum columns by threading technique improves not only the three dimensional appearance of the philtrum but Cupid’s bow as well (–).
Figure 5 A 60-year-old woman with flattening of Cupid’s bow and downward turn of the commissures.

Deep fat injection of the upper lip into the wet roll is a method to volumize and to reshape. In case of advanced bone resorption or dental problems and loose connective tissue, advanced volumizing may lead to an undeserved ptosis (duckbill look) and loss of fine lip motion. In such cases, plastic surgery and dental restoration may be more appropriate.
The downward turn of the corners of the mouth can be seen in subjects of various ages. Whereas in younger individuals the strength of the platysma and depressor anguli oris is responsible and can be corrected by botulinum toxin injections, this is rarely the case in elderly women.Citation26,Citation27 Ptosis, loss of elasticity, repetitive facial expression, gravity, and extrinsic aging contribute to the downward turn which eventually results in melomental folds. These folds are associated with sadness and older age. Their negative appearance may be further increased by loss of volume in the lateral parts of lower lip. When the corner of the mouth is stretched laterally, a convex curvature of the wet roll becomes obvious (). This is obviously due to partial loss of superficial fat layer.
Figure 6 A 68-year-old woman with flattening of Cupid’s bow, thinning of white rolls, perioral fine lines, and marionette lines.

Deep fat augmentation by filler injection into the wet roll will volumize and reshape the lower lips and elevate the corners of the mouth. This will also reduce the depth of the melomental fold. In case of grade ≥3 of melolabial folds, serial punctures or threading along the fold will be necessary to obtain a good outcome. Only in patients with a strong platysma, small amounts of botulinum toxin A injections into the anterior part of the platysma and close to the mandibular insertion point of the depressor anguli oris will contribute to a lift of the corner of the mouth.Citation26 Injections need to be placed superficially because of the particular muscular anatomy.Citation28 The chin crease can be improved by deep filler placement. In cases of poppy chin, the procedure may be combined with injections of 5–8 units of botulinum toxin A (Botox units).
The satisfaction with perioral rejuvenation in elderly females was high; 96.5% of the females were satisfied or highly satisfied. Adverse effects were mild and temporary. Pain during injection was reduced by cold compresses before and after the procedure. Bruising was the most common (16.1%) adverse effect after rejuvenation. Slight asymmetry was seen in 0.5% of cases. We observed no case of herpes reactivation or bacterial infection.
Conclusion
Facial aging is accompanied by perioral hard and soft tissue changes leading to wrinkles, folds, and loss of contour and volume of the lips. This becomes more pronounced in elderly subjects. With individually tailored filler injection techniques, possibly in conjunction with low dose botulinum toxin, a marked improvement of appearance is realistic. Patients after dental restoration will also benefit from the rejuvenation of perioral soft tissue.
Disclosure
U Wollina received honoraria for lectures and courses by Allergan and Merz.
References
- KleinAWIn search of the perfect lip: 2005Dermatol Surg20053111 Pt 21599160316416644
- LevequeJLGoubanovaEInfluence of age on the lips and perioral skinDermatology2004208430731315178912
- DesaiSUpadhyayMNandaRDynamic smile analysis: changes with ageAm J Orthod Dentofacial Orthop20091363310e1e1019732654
- TrookmanNSRizerRLFordRMehtaRGotzVClinical assessment of a combination lip treatment to restore moisturization and fullnessJ Clin Aesthet Dermatol2009212444820725584
- TrookmanNSRizerRLFordRHoEGotzVImmediate and long-term clinical benefits of a topical treatment for facial lines and wrinklesJ Clin Aesthet Dermatol200923384320729942
- FreseCStaehleHJWolffDThe assessment of dentofacial esthetics in restorative dentistry: a review of the literatureJ Am Dent Assoc2012143546146622547716
- NiamtuJIIIPerioral soft-tissue rejuvenation techniques to enhance esthetic restorative dentistryCompend Contin Educ Dent2003241181181281481681818624129
- PessaJESliceDEHanzKRBroadbentTHJrRohrichRJAging and the shape of the mandiblePlast Reconstr Surg2008121119620018176221
- ShawRBJrKatzelEBKoltzPFKahnDMGirottoJALangsteinHNAging of the mandible and its aesthetic implicationsPlast Reconstr Surg2010125133234220048624
- PendergastPMAnatomy of the face and neckShiffmanMADi GuiseppeACosmetic SurgeryBerlin-HeidelbergSpringer-Verlag20122945
- RohrichRJPessaJEThe fat compartments of the face: anatomy and clinical implications for cosmetic surgeryPlast Reconstr Surg200711972219222717519724
- RohrichRJPessaJEThe anatomy and clinical implications of perioral submuscular fatPlast Reconstr Surg2009124126627119568090
- SullivanPKHoyEAMehanVSingerDPAn anatomical evaluation and surgical approach to the perioral mound in facial rejuvenationPlast Reconstr Surg201012641333134020885255
- GierloffMStöhringCBuderTWiltfangJThe subcutaneous fat compartments in relation to aesthetically important facial folds and rhytidesJ Plast Reconstr Aesthet Surg201265101292129722658728
- Garcia de MitchellCAPessaJESchaverienMVRohrichRJThe philtrum: anatomical observations from a new perspectivePlast Reconstr Surg200812261756176019050528
- CarruthersACarruthersJHardasBA validated lip fullness grading scaleDermatol Surg200834Suppl 2S161S16619021674
- CarruthersACarruthersJHardasBA validated grading scale for Marionette linesDermatol Surg200834Suppl 2S167S17219021675
- WollinaUGoldmanAHyaluronic acid dermal fillers: safety and efficacy for the treatment of wrinkles, aging skin, body sculpturing and medical conditionsClin Med Rev Therapeutics2011310.4137/CMRT.S6928
- AlamMGladstoneHKramerEMAmerican Society for Dermatologic SurgeryASDS guidelines of care: injectable fillersDermatol Surg200834Suppl 1S115S14818547175
- RzanyBBecker-WegerichPBachmannFErdmannRWollinaUHyaluronidase in the correction of hyaluronic acid-based fillers: a review and a recommendation for useJ Cosmet Dermatol20098431732319958438
- SantoroSRussoSArgenzioVBorzacchielloARheological properties of cross-linked hyaluronic acid dermal fillersJ Appl Biomater Biomech20119212713622065390
- FagienSMaasCMurphyDKJuvéderm Lips Study GroupJuvederm ultra for lip enhancement: an open-label, multicenter studyAesthet Surg J201333341442023515385
- GlogauRGBankDBrandtFA randomized, evaluator-blinded, controlled study of the effectiveness and safety of small gel particle hyaluronic acid for lip augmentationDermatol Surg2012387 Pt 21180119222759255
- BosniakSCantisano-ZilkhaMGlavasIPNonanimal stabilized hyaluronic acid for lip augmentation and facial rhytid ablationArch Facial Plast Surg20046637938315545531
- WollinaUGoldmanANaoumCSide effects in aesthetic medicine. Spectrum, management and avoidanceHautarzt2013643155162 German23430168
- GoldmanAWollinaUElevation of the corner of the mouth using botulinum toxin type aJ Cutan Aesthet Surg20103314515021430826
- WollinaUPayneCRAging well – the role of minimally invasive aesthetic dermatological procedures in women over 65J Cosmet Dermatol201091505820367673
- WollinaUKonradHManaging adverse events associated with botulinum toxin type A: a focus on cosmetic proceduresAm J Clin Dermatol20056314115015943491