Abstract
Background
Romania has some of the highest mortality figures in the world attributable to ischemic heart disease and stroke among both men and women.
Objectives
To assess the changes in cardiovascular risk factors and ischemic heart disease in a group of subjects over 65 years of age during 1 year in an urban community of Romania.
Materials and methods
We studied 515 subjects (264 women and 251 men) with a mean age of 73.41±6.44 years, followed up over the course of 1 year in order to determine the changes that occurred in cardiovascular risk factors and in the evolution of ischemic heart disease. At the beginning and after 1 year, we determined the following parameters: anthropometric measurements, blood pressure, smoking status, lipid profile (total cholesterol, triglycerides, high-density lipid cholesterol, low-density lipid cholesterol), fasting plasma glucose, and the presence of ischemic heart disease.
Results
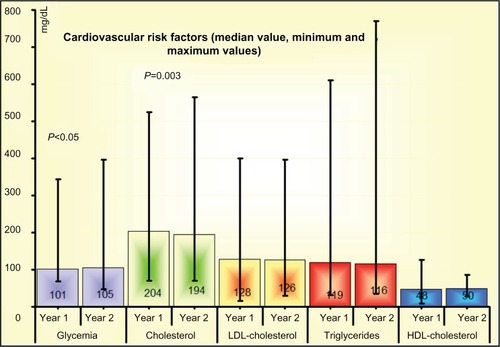
There were no differences between the first and second assessments concerning the incidence of smoking (12.3% versus (vs) 12.5%), obesity (25% vs 26%), diabetes mellitus (19% vs 22.9%), or hypertension (88.2% vs 92.2%). Statistically significant differences were recorded regarding dyslipidemia (40.6% vs 30.3%, P<0.001). Cholesterol median values decreased (204 mg/dL vs 194 mg/dL, P=0.003), while median concentrations of plasma glucose increased (101 mg/dL vs 105 mg/dL, P<0.05). At the same time, we noted a higher incidence of ischemic heart disease (51.65% vs 63%).
Conclusion
Our data show that in subjects over 65 years of age, cardiovascular disease occurs more often in women, but with certain features that should be taken into account. In addition, we point out the importance of reducing cardiovascular risk factors. However, we should not expect a major decrease or improvement in cardiovascular risk factors with such a short follow-up. Such results will be achieved only through long-term interventions.
Introduction
Data provided by the World Health Organization show that during the last decade, cardiovascular disease became the main cause of death worldwide, accounting for 17.3 million deaths per year.Citation1 During 1990–2001, cardiovascular mortality increased from 26% to 28% in developed and developing countries.Citation1 The highest rates of mortality due to cardiovascular diseases, representing approximately 58%, are recorded in Eastern European countries, whereas the lowest (10%) are to be found in the African territories (Saharan Africa).Citation1 However, in financially strong countries, the percentages reach 38%.Citation1 All in all, the incidence of most cardiac diseases increases with the process of aging.
In Romania, although there are important limitations regarding the data-collection system, we can identify a clear tendency of increasing mortality due to ischemic heart disease and stroke. In the 1990s, there was a sudden increase in the prevalence of ischemic heart disease, with a subsequent increasing tendency. According to the latest American Heart Association statistics, published in January 2013, Romania holds fourth place in the world in terms of mortality due to ischemic heart disease and stroke in men, after the Russian Federation, Lithuania, and Bulgaria, and third place in women, after the Russian Federation and Bulgaria.Citation2 While in 1970, 7.33% of the cardiovascular deaths were due to myocardial infarction, the proportion amounted to 13.5% in 1998.Citation3
In this context, this study aims at determining how the main cardiovascular risk factors and ischemic heart disease evolved in the course of 1 year in a group of subjects over 65 years of age in an urban community of Romania.
Materials and methods
We conducted a retrospective study based on medical records issued by general practitioners, aimed at achieving an epidemiological survey of cardiovascular risk factors and cardiac diseases in subjects over 65 years old by highlighting sex differences. The study population was followed prospectively during 1 year (2007–2008) in order to determine the changes that occur in cardiovascular risk profile and cardiovascular disease.
We studied 515 patients (264 women and 251 men) over 65 years of age, evaluated for the presence of cardiovascular risk factors and ischemic heart disease. The mean age was 73.41±6.44 years. Fifty-three patients were lost to follow-up (deceased or with unavailable personal data), and only 462 patients underwent the second assessment (235 women, 227 men).
During the initial evaluation and 1 year after that, the following parameters were determined: anthropometric measurements, blood pressure, smoking status, lipid profile (total cholesterol, triglycerides, high-density lipid [HDL]-cholesterol, low-density lipid [LDL]-cholesterol), fasting plasma glucose, and the presence of ischemic heart disease. Blood glucose was measured by the glucose oxidase method, while serum lipids, total cholesterol, triglycerides, and HDL-cholesterol were measured by using commercially available kits. LDL-cholesterol was estimated using Friedewald’s formula.
According to current European Society of Cardiology guidelines, hypertension was classified as: mild hypertension 140/90–159/99 mmHg, moderate hypertension 160/100–179/109 mmHg, and severe hypertension >180/110 mmHg.Citation4 Data on hypertension were collected from the medical records kept by the patients’ family physicians. Medical files also revealed which patients were under antihypertensive treatment. Uncomplicated hypertension was registered as a cardiovascular risk factor, not as cardiovascular disease.
By using the criteria set out in the National Cholesterol Education Program Adult Treatment Panel III approach to dyslipidemias, total cholesterol levels over 200 mg/dL, LDL-cholesterol levels over 100 mg/dL, triglyceride plasma concentrations exceeding 150 mg/dL, and HDL-cholesterol levels less than 46 mg/dL in women and 40 mg/dL in men were considered pathological.Citation5
Patients were classified according to their body mass index (BMI) as normal weight (BMI ≤25 kg/m2), overweight (BMI between 25 kg/m2 and 29.9 kg/m2) and obese (BMI >30 kg/m2).Citation4
Statistical analysis was performed using SPSS for Windows (version 16.0; IBM Corporation, Armonk, NY, USA) and MedCalc (version 10.3.0.0; MedCalc Software, Ostend, Belgium) software programs. Analysis of the differences between qualitative variables was performed using the χ2 test. The Kolmogorov–Smirnov test was used to assess the normal distribution of continuous numerical variables. The normality condition was met by BMI and serum lipids (total cholesterol and LDL-cholesterol), but not for glycemia, HDL-cholesterol, or triglycerides (so we had to use the Mann–Whitney U test for all variables in order for unitary analysis). Values of P<0.05 were considered statistically significant.
Results
There were no differences between the first and second assessments concerning the incidence of smoking (12.3% versus (vs) 12.5%), obesity (25% vs 26%), diabetes mellitus (19% vs 22.9%), or hypertension (88.2% vs 92.2%). Regarding the presence of dyslipidemia, we found a marked decrease in its prevalence (40.6% vs 30.3%, P<0.001). As shown in and , there were no differences between the two medical assessments regarding the plasma mean levels of triglycerides, HDL-cholesterol, and LDL-cholesterol. However, there was a significant decrease in total cholesterol levels, but also an increase in plasma glucose concentrations ().
Table 1 Comparative values of plasma glucose and lipid fractions between the two medical assessments
Figure 1 Evolution of glucose and lipid-fraction concentrations between the two assessments.
Abbreviations: HDL, high-density lipid; LDL, low-density lipid.
The relationship between sex and cardiovascular risk factors was also assessed. Although at the initial medical evaluation there were significant sex differences in the incidence of smoking, obesity, dyslipidemia, and hypertension, at 1-year follow-up most of them had disappeared (only those concerning smoking and dyslipidemia stayed unchanged) ().
Table 2 Comparative values of cardiovascular risk factors between the two assessments and sex-related differences
During the first assessment, there was a significant difference in all plasma lipid-fraction values between women and men, in contrast to the second evaluation, when these differences were present only in terms of HDL-cholesterol and total cholesterol levels ().
Table 3 Comparative values of plasma glucose and lipid fractions between the two assessments and sex-related differences
A higher incidence of ischemic heart disease (51.65% vs 63%) was noticed during the second evaluation, even though the occurrence of silent ischemic heart disease decreased from 3.9% to 0.2% (P=0.0002), which emphasizes the fact that the increase was due to stable angina pectoris, old myocardial infarction, or other causes of ischemic heart disease (arrhythmias or heart failure), regardless of sex ().
Table 4 Evolution of ischemic heart disease and its complications
The incidence of ischemic heart disease was considerably higher in elderly women than in men, with an increase from 55.7% to 65.1% in women and from 47.4% to 60.8% in men, which revealed a similar growth for both sexes, the ratio differences between men and women being significantly similar. Myocardial infarction amounted to 9.5% in 2008, similar to the values recorded in 2007 (8.7%, not significant). There were no significant differences between the initial evaluation and 1 year later, irrespective of sex (women 5.7% vs 6% in 2008, men 12% vs 13.2% in 2008). Differences regarding stable angina remained unchanged between the two assessments, in both women (24.7% in 2008 vs 21.2% in 2007) and men (12.8% in 2008 and 12.7% in 2007).
Stable angina occurred more often in women, whereas old myocardial infarction was predominant in men during both evaluations. In addition, there were no significant changes in the incidence of heart failure and rhythm disorders between the two assessments (10.48% vs 13.2% and 23.1% vs 26%, respectively).
As for cardioprotective medication, 65% of the patients received aspirin, 71.9% beta-blockers, and 74.9% angiotensin-converting enzyme inhibitors; 48.8% were given statins. Patients over 75 years of age received less medication than those under 75 years: 32% versus 54.2%, respectively (P=0.009). A total of 46.9% of patients with ischemic heart disease received statins.
Discussion
According to the INTERHEART study, traditional cardiovascular risk factors account for most of myocardial infarction risk worldwide in both sexes, ages and in all regions.Citation6 In Eastern Europe, the most frequent modifiable cardiovascular risk factors are smoking, obesity, hypertension, and hypercholesterolemia (serum cholesterol levels over 200 mg/dL). The present study showed that the main investigated cardiovascular risk factors (arterial hypertension, diabetes mellitus, smoking, obesity) had the same incidence 1 year after the initial assessment.
There are insufficient data on the incidence of cardio vascular risk factors in general and the main heart diseases in Romania, especially as after the 1990s there was a heart disease “boom” following the transition from communism to a so-called liberalization. The rise is constant, with no perceptible tendencies of improvement, which could be explained by a drastic lifestyle change, chiefly the prevalence of smoking and fast-food diets.
Hypertension is one of the major cardiovascular risk factors found in Romania, with a constantly growing incidence. In 2006, the occurrence of hypertension was reported to be 40%, and by 2012 it remained unchanged, increasing with age.Citation7,Citation8 The incidence of hypertension was very high in the study group of elderly subjects: 88% in 2007 and 92.2% in 2008. Among the countries of Eastern Europe, Croatia has the highest ratio of hypertensive men (50%) and Bosnia-Herzegovina has the highest number of hypertensive women (45%).Citation1
Romanian epidemiological data show that the incidence of smoking decreased from 29.7% to 22% between 2003 and 2011.Citation9 Presently, 35.2% of Romanian men and 15.3% of Romanian women are smokers.Citation9 In our study, the prevalence of smoking was more than double in men than in women, both during 2007 and 2008. In Eastern Europe, the highest incidence of smoking in men was reported in Ukraine (62%) and in women in Serbia (27%).Citation1
The prevalence of diabetes mellitus increased insignificantly from 19% to 22.9%. Women displayed similar ratios during both years (21.2% vs 23.8%), whereas men presented a significantly higher incidence (from 16.7% to 22%).
In 2007, 40.6% of the subjects displayed dyslipidemia, whereas dyslipidemia was found only in 30.3% of the patients in 2008, the decrease being similar in women and men (from 48.5% to 36.6% in women, and from 32.3% to 23.8% in men). Significantly lower levels were recorded for hypercholesterolemia. The incidence of hypercholesterolemia in Romania amounted to nearly 63%, but only 16% of the subjects were therapeutically controlled (values <175 mg/dL).Citation1 Hypercholesterolemia affects almost 39% of the world population, with more than half this incidence from developing countries. In Eastern Europe, the highest occurrences of unaware hypercholesterolemia can be found in Bulgaria (72%), Latvia (70%) and Croatia (70%).Citation10 Among Romanian subjects over 30 years old, cholesterol levels vary between 192 and 216 mg/dL in men and between 189 and 217 mg/dL in women.Citation1
In our group of elderly Romanian subjects, the lower lipid-fraction levels could be due to both primary and secondary cardiovascular prevention measures and also to the intensive treatment with statins recommended by physicians or even requested by patients who were informed about the role of high lipid-fraction levels in the development of cardiovascular diseases. According to the data provided by the EUROASPIRE (European Heart Survey on secondary and primary prevention of coronary heart disease) III study,Citation10 the statin administration ratio was lower than the all lipid-lowering drugs (88.8%) administration ratio in Europe. In spite of the lower ratio of statin prescription, our study recorded a significant decline in the incidence of dyslipidemia in general and average cholesterol level in particular. The respective changes can be ascribed to the fact that the initial assessment of risk factors had alerted the patients to the presence of dyslipidemia (side by side with the presence of other risk factors), which triggered lifestyle adjustments.
The prevalence of obesity remained similar: 25% in 2007 and 26% in 2008. The ratios remained almost identical in men and women during both years (women, 29.5% in 2007, 29.6% in 2008; men [insignificant difference], 20.3% in 2007, 20.6% in 2008). The incidence of obesity is also growing in Romania in both women (8% [35.9% overweight]) and men (7.6% [49.9% overweight]).Citation11 An alarming increase in obesity was recorded among children and teenagers.Citation11 In Europe, the highest rates of obesity in men and women are to be noticed in Croatia (22%) and Turkey (30%), respectively.Citation1,Citation12
Special attention needs to be paid to the evolution of cardiovascular risk factors and sex-related differences. In our study, the incidence of hypertension was basically identical in both years: 88.2% in 2007 and 92.2% in 2008. Women had higher blood pressure values than men in both years, but a high incidence was found in both sexes. The incidence of hypertension increased with age for both sexes, with a more noticeable increase in women between 45 and 54 years old. In subjects younger than 35 years, hypertension was clearly more common in men than in women.Citation13 However, regardless of age, the presence of hypertension in women is associated with a three- to fivefold higher risk of coronary heart disease.Citation14,Citation15
Our study showed that in elderly subjects, all lipid fractions levels were higher in women than in men, regardless of the assessment moment. Before menopause, total cholesterol and LDL-cholesterol were generally lower in women, whereas HDL-cholesterol was higher than in men.Citation16 Whereas after the age of 50 years, LDL-cholesterol levels remained relatively the same in men, in menopausal women there was a significant increase in LDL-cholesterol levels, reaching maximum values between the ages of 55 and 65 years.Citation16 Thus, after the age of 65 years, the incidence of dyslipidemia was about twice as high in women.Citation17 Menopause also influenced HDL-cholesterol levels, which decreased gradually during the last 2 years preceding menopause and after, especially the HDL2 fraction, which has an important cardioprotective role.Citation16,Citation18 Cardiovascular protection dropped with the decrease in HDL levels. Therefore, low HDL values may be considered major factors for an increased cardiovascular risk in postmenopausal women. However, in our study, HDL-cholesterol levels were higher in women in both years.
Triglyceride levels also increased after menopause.Citation19 Our research showed that the incidence of obesity was higher in elderly women than in men, especially in the first year of observation. Women seemed more likely to display cardiovascular risk factors than men, especially obesity in adolescence, pregnancy, and menopause.Citation16
The increasing occurrence of ischemic heart disease can be attributed to the 1-year aging process of the subjects enrolled in the study. In addition, another explanation could be the fact that the patients who underwent the initial assessment of cardiovascular risk factors were informed about the presence of cardiovascular risk factors and cardiovascular disease. Therefore, the patients probably sought medical advice more often during the following year, so additional cardiovascular diseases perhaps present at the initial assessment but undetected by regular screening tests might have been diagnosed. Ischemic heart disease occurs about 10 years later in women than in men.Citation20,Citation21 In general, the form of ischemic heart disease prevailing in women is angina pectoris, whereas myocardial infarction occurs more often in men, previous assertions being in agreement with our findings.Citation17,Citation22 It is important to emphasize that in the present study, the data were collected from medical records kept by general practitioners, so none of the subjects displayed acute coronary syndromes at the moment of assessment. The highest incidence of ST-segment elevation acute coronary syndromes occurs in young men (under 55 years), the ratio decreasing with age.Citation21 Nearly half of the male patients with ischemic heart disease younger than 65 years came with clinical symptoms of an ST-segment elevation acute coronary syndrome, whereas only 40% of the women did.Citation21 In patients over 65 years of age, the differences between men and women were less significant.Citation21 In women, unstable angina is responsible for most cases of acute coronary syndromes,Citation21,Citation23 especially before the age of 65 years. After the age of 65 years, women present in equal proportions ST-segment elevation and non-ST-segment elevation acute coronary syndromes.Citation13
In the present study, although the main risk factors, chiefly obesity and dyslipidemia, decreased during 1 year, the incidence of ischemic heart disease increased.
The data prove that over 65 years of age, cardiovascular pathology ceases to be sex-related. The increase in the incidence of cardiovascular diseases could be chiefly ascribed to the 1-year aging of the study patients, and secondly to the fact that the initial assessment of the risk factors alerted the patients to their presence and the possibility of cardiovascular diseases, so that more cardiovascular diseases possibly present at initial examination but undetected by regular screening were diagnosed.
Finally, we believe that the results of the present paper present significant data on the incidence of cardiovascular risk factors in a population over 65 years of age of a city that is an academic center, supposedly with highly proficient medical specialists.
In conclusion, the data supplied by our study show that in subjects over 65 years old, cardiovascular disease prevails in women, with some particular characteristics that should be taken into account, and that cardiovascular risk factors need to be addressed and influenced. However, one should not expect a major decrease or improvement in the cardiovascular risk factors during such a short period; positive results will probably be achieved through long-term interventions.
Disclosure
The authors report no conflicts of interest in this work.
References
- ThomasAGGazianoJMGlobal burden of cardiovascular diseaseBonowROMannDLZipesDPLibbyPBraunwald’s Heart Disease: A Textbook of Cardiovascular Medicine9th edPhiladelphiaElsevier Saunders2011119
- GoASMozaffarianDRogerVLHeart Disease and Stroke Statistics – 2013 update: a report from the American Heart AssociationCirculation20131271e6e24523239837
- ZdrengheaDVǎideanGPopDRiscul cardiovascularZdrengheaDVǎideanGPopDCardiologie PreventivăCluj-NapocaCasa Cărţii de Ştiinţă2003344
- ManciaGDe BackerGDominiczakA2007 Guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC)Eur Heart J200728121462153617562668
- GrundySMCleemanJIMerzCNImplications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelinesCirculation2004110222723915249516
- YusufSHawkenSOunpuuSEffects of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control studyLancet2004364943893795215364185
- DorobanţuMBartoşDApetreiEHypertension in Romania: where are we and what can we do? Results from SEPHAR II studyRom J Cardiol20124285292
- DorobanţuMDarabontRGhiorgheSProfile of the Romanian hypertensive patient data from SEPHAR II studyRom J Intern Med201250428529623610976
- Romania Ministry of Health [website on the Internet] Available from: http://www.ms.gov.roAccessed October 10, 2013
- KotsevaKWoodDDe BackerGDe BacquerDPyöräläKKeilUEUROASPIRE III: a survey on the lifestyle, risk factors and use of cardioprotective drug therapies in coronary patients from 22 European countriesEur J Cardiovasc Prev Rehabil200916212113719287307
- EurostatOverweight and obesity – BMI statistics: database Available from: http://epp.eurostat.ec.europa.eu/statistics_explained/index.php/Overweight_and_obesity_-_BMI_statistics#DatabaseAccessed October 10, 2013
- World Health OrganizationWHO global InfoBase2008 Available from: http://www.who.int/infobaseAccessed October 21, 2013
- Stramba-BadialeMFoxKMPrioriSGCardiovascular diseases in women: a statement from the policy conference of the European Society of CardiologyEur Heart J2006278994100516522654
- MaasAHvan der SchouwYTRegitz-ZagrosekVRed alert for women’s heart: the urgent need for more research and knowledge on cardiovascular disease in women: proceedings of the workshop held in Brussels on gender differences in cardiovascular disease, September 29, 2010Eur Heart J201132111362136821406440
- KannelWBBlood pressure as a cardiovascular risk factor: prevention and treatmentJAMA199627520157115768622248
- StanglVBaumannGStanglKCoronary atherogenic risk factors in womenEur Heart J200223221738175212419293
- AndreottiFMarcheseNWomen and coronary heart diseaseHeart200894110811618083955
- StevensonJCCrookDGodslandIFInfluence of age and menopause on serum lipids and lipoproteins in healthy womenAtherosclerosis199398183908457253
- JensenJNilasLChristiansenCInfluence of menopause on serum lipids and lipoproteinsMaturitas19901243213312124647
- WengerNKShawLJVaccarinoVCoronary heart disease in women: update 2008Clin Pharmacol Ther2008831375118043680
- RosengrenAWallentinLK GittABeharSBattlerAHasdaiDSex, age, and clinical presentation of acute coronary syndromesEur Heart J200425866367015084371
- PiloteLDasguptaKGuruVA comprehensive view of sex-specific issues related to cardiovascular diseaseCMAJ20071766S1S4417353516
- SongXTChenYDPanWQLüSZGender-based differences in patients with acute coronary syndrome: findings from Chinese Registry of Acute Coronary Events (CRACE)Chin Med J (Engl)2007120121063106717637223