
Abstract
Hip fractures are a very serious socio-economic problem in western countries. Since the 1950s, orthogeriatric units have introduced improvements in the care of geriatric patients admitted to hospital because of hip fractures. During this period, these units have reduced mean hospital stays, number of complications, and both in-hospital mortality and mortality over the middle term after hospital discharge, along with improvements in the quality of care and a reduction in costs. Likewise, a recent clinical trial has reported greater functional gains among the affected patients. Studies in this field have identified the prognostic factors present upon admission or manifesting themselves during admission and that increase the risk of patient mortality or disability. In addition, improved care afforded by orthogeriatric units has proved to reduce costs. Nevertheless, a number of management issues remain to be clarified, such as the optimum anesthetic, analgesic, and thromboprophylactic protocols; the type of diagnostic and therapeutic approach best suited to patients with cognitive problems; or the efficiency of the programs used in convalescence units or in home rehabilitation care. Randomized clinical trials are needed to consolidate the evidence in this regard.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Osteoporotic hip fractures are one of the main health problems in geriatric patients. A total of 1.3 million hip fractures were diagnosed in 1990,Citation1 and this figure is expected to increase to over 6 million by 2050.Citation2 A total of 80% of the fractures in women and 50% of those in men occur at over 70 years of age.Citation3 Ninety percent of the fractures are a result of falls from standing height.Citation4 The mortality rate can reach 10% during admission in hospital and 30% after 12 months.Citation5,Citation6 Only 50% of those who survive recover the functional level they had before the accidentCitation7,Citation8 and 25% of the patients who were independent before the fall require admission to a home for the elderly.Citation9 The estimated socio-economic costs represent 0.1% of the global health care costs worldwide, reaching 1.4% in the more developed countries.Citation1 The mean age of patients with hip fractureCitation10 and the presence of comorbidityCitation11 are the main reasons warranting orthogeriatric comanagement of these individuals, which reduces the risk of perioperative complications, functional deterioration, and mortality.Citation12
In this regard, geriatric joint trauma management units were introduced in the UK in the mid-twentieth century.Citation13 However, it is over the last 20 years that the design and implementation of coordinated perioperative models have increased.Citation14 Such coordinated patient care has been shown to reduce in-hospital complications,Citation15,Citation16 hospital stay and readmissions,Citation17 disability, and in-hospital mortality.Citation16
A recent editorialCitation18 considers that geriatric medicine improves our knowledge of the extra-traumatology factors that complicate the patient’s course and influence the outcome of treatment. The clinical and social complexity of elderly patients demands close cooperation among the different professionals, with a different approach to management from that applicable to younger individuals.Citation19 In addition to the traditional goals of the orthogeriatric team, there is another crucial objective: patient enrollment in the most appropriate rehabilitation program in order to reduce the need for institutionalization and facilitate functional recovery and reintegration to the regular social setting of the patient.Citation19
In this regard, correct assessment of the previous functional situation and maximum recovery of that situation are of vital importance. The high prevalence of disability following fracture can modify the natural patient referral process after hospital discharge,Citation20 and in this sense the management plan does not conclude with hospital discharge but rather comprises the continuation of patient care beyond the in-hospital process. The actions of the orthogeriatric team thus extend beyond the hospital setting, expanding the benefits of integral geriatric care.Citation19
It is in the UK where the role of orthogeriatrics has been best defined to date, largely as a result of the development of the best practice tariff, introduced in 2010 with the purpose of improving the management of patients with hip fracture.Citation21 Presurgical and postsurgical cognitive assessments were subsequently also included.Citation22 The National Institute for Health and Care Excellence drafted a document on the quality care of patients with hip fracture, underscoring a series of high-quality indicators to be complied with in order to boost efficiency in the management of patients with hip fracture.Citation23
The orthogeriatric care models agree on the suitability of care provided by multidisciplinary teams with knowledge of geriatrics, the advisability of early surgery, the need for a case manager (in this case a geriatrician) throughout the whole process, pain control, avoidance of the appearance or worsening of geriatric syndromes, and correct continuity of care after hospital discharge, thus attempting to recover the functional condition before the time of fracture.Citation24 Such orthogeriatric management has been validated by a recent meta-analysis.Citation25
However, there are still issues requiring study and analysis, such as the optimum thromboprophylactic protocols, correct analgesic regimens, assessment and treatment of cognitive deterioration and nutritional conditions during the in-hospital period, improvement of patient mobility, and postsurgical rehabilitation.Citation24
The present review aims to offer answers to some of these uncertainties regarding the orthogeriatric care of patients with hip fracture and attempts to clarify which measures have improved the management outcomes.
Methods
The present review was carried out by conducting an electronic search in OVID (Medline and Embase), combining the following MeSH keywords: “hip fractures” and “geriatric assessment”, combined with “perioperative management” and “orthogeriatric care”. The search was limited to publications in the last 5 years; in English, Spanish, and French; and in human subjects. A total of 177 articles were obtained, of which 86 were finally selected. The MeSH construction [Hip fractures] AND ([Geriatric assessment] OR “perioperative management”) OR “orthogeriatric care” OR “geriatric syndromes”) was used. Some additional instructions were added for certain specific objectives where necessary. In 14 cases, supplementary information was obtained in the form of references of the selected articles. Details of the evaluation and selection process of the items are shown in .
Figure 1 Flow chart study selection procedure used in literature search.
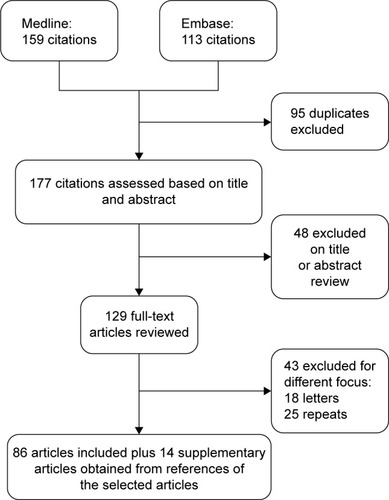
The articles were selected by four investigators based on the following inclusion criteria: randomized clinical trials, cohort studies, case–control studies, observational studies, and before–after analyses in orthogeriatric units; population: geriatric patients with proximal femoral fracture; intervention: orthogeriatric treatment begun perioperatively; and outcomes: surgical delay, length of hospital stay, prognostic factors and mortality, functional recovery, geriatric syndromes, perioperative care such as renal function, anemia, second hip fracture and complications, surgical treatment, and costs.
The exclusion criteria were letters to the Editor, case reports, articles with no available abstract or those with only the abstract published, and studies meeting the inclusion criteria but with ≥50% of the study sample aged under 65 years (ie, predominantly non-geriatric). All the articles were reevaluated by the authors of the review, and final inclusion was restricted to those of sufficient quality to afford information pertinent to the objectives of this review.
The outcome measures examined were mortality, length of hospital stay, functional status, medical complications, destination after discharge, functional recovery, secondary prevention treatments, and readmissions.
Results
The efficiency and benefits of orthogeriatric careCitation14 indicate that the aforementioned multidisciplinary approach should be generalized. However, this patient care model has still not been implemented in many hospitals. The centralization of information in the form of national registries would facilitate the comparison of results between the traditional approach and orthogeriatric management and would allow us to define the benefits of the different implemented models.Citation18 The variants of the model coincide in underscoring the need for early geriatric clinical care and early surgical management,Citation26 since both these measures can reduce in-hospital morbidity–mortality.
A meta-analysis of 35 independent studies recruiting 191,873 patients described greater survival among patients who underwent early surgery (odds ratio [OR] 0.74; 95% confidence interval [CI] 0.67–0.81; P<0.001). Authors calculated odds of death with cutoff of surgical delay in 24 hours (OR 0.74 [95% CI 0.62–0.87; P<0.001]) and 48 hours (OR 0.75 [95% CI 0.68–0.81; P=0.031]). There was no difference in survival when the surgical delay cutoff was established in less than 12 and 96 hours, respectively.Citation27 (The most relevant results included in this review are summarized in .)
Table 1 Summary of the some most relevant studies included in this review
Previously, Vidan et alCitation28 found delays in surgery to be associated with increased mortality from day 6 after fracture. A meta-analysis of 16 observational studies (n=13,478) in turn showed surgery in the first 24 hours, versus in the first 72 hours, to reduce patient mortality.Citation29
The main cause of surgical delays is the lack of available operating rooms.Citation28 Clinical stabilization, based on clinical recommendations and guidelines, on the part of the orthogeriatric teams can contribute to reduce such delays, increasing comorbidity diagnostic precision,Citation30 since the second most important cause of surgical delays is the presence of medical complications.Citation28
Considering the need for early preoperative medical evaluation to avoid clinical contraindications to surgery, four reviews have recommendedCitation31–Citation34 comprehensive geriatric assessment with the purpose of adequately estimating perioperative risk and preventing complications. Likewise, in emphasizing the importance of early clinical care and homogeneity of the management objectives, we consider that the orthogeriatric clinical protocols should also implicate the emergency care service.
As has been pointed out by an editorial,Citation14 another important advantage of such orthogeriatric care is the shortening of hospital stay, despite a lack of analyses by subgroups in different studies, based on the case mix referred to comorbidity and prior functional and social condition. Such shortening of stay is the result of continuously improving quality of care, reducing patient stay in emergency service, facilitating structured management, and incorporating new measures based on evidence.Citation35
Geriatric syndromes
Delirium
The incidence of delirium in elderly individuals with hip fracture varies between 38% and 61% and is greater in patients with dementia.Citation36 In subjects without prior dementia or delirium, the incidence of delirium and nonspecific cognitive dysfunction is lower (21.3%),Citation37 and in such cases hypoactive delirium is the most common presentation.Citation38 Likewise, delirium is a risk factor for poorer survival 6 months after hospital discharge.Citation38
The published interventions for the prevention and treatment of delirium combine different strategies, based on a multifactorial approach or proactive geriatric consultation and follow-up.Citation39 Different studies have reported a decrease in the incidence of delirium in the intervention group,Citation40,Citation41 and even a shorter duration of delirium.Citation42 Data from the subanalysis of a clinical trial,Citation43 only including patients with delirium upon admission, described a significant decrease in postoperative delirium in the orthogeriatric care group, together with a significant decrease in the incidence of urinary tract infections, nutritional problems, and the incidence of falls.
The incidence of delirium can be lowered by assigning patient rooms close to the common areas and rehabilitation facilities, and this measure, moreover, improves patient comfort and contributes to shortening hospital stay.Citation44 Proactive geriatric care, electrolyte normalization and adequate hydration, oxygenation, pain and constipation control, drug monitoring with reviewing of the psychoactive medication used, and early mobilization all contribute to reducing the incidence of delirium.Citation45
Cognitive impairment
Forty percent of all elderly people admitted because of hip fracture suffer from some degree of cognitive impairment.Citation46 Functional recovery of patients with cognitive impairment and hip fracture is variable.Citation43 In this regard, a systematic review has found similar functional gains in patients with and without mild or moderate cognitive impairment.Citation47 In a cohort of 314 elderly patients admitted due to hip fracture, in which 43% suffered from cognitive impairment, walking capacity prior to fracture, the presence of pressure ulcers (bed sores), and the incidence of delirium were found to be more robust predictors of functional recovery than the degree of cognitive impairment.Citation48 In a study published by our groupCitation49 on 1,258 patients with hip fracture, 30% were seen to have dementia prior to admission. The patients without cognitive impairment showed higher walking rates at discharge and after 6 and 12 months than the patients with mild, moderate, or severe dementia – independently of age, prior Barthel score, sex, Charlson score, or presence of delirium upon admission. The mortality rate at discharge and after 1, 6, and 12 months was also lower among the patients without dementia than among those with mild, moderate, or severe dementia. In the adjusted model, the differences remained significant only in the group with severe dementia. Patients with cognitive impairment obtain benefit from rehabilitation programs in orthogeriatric units that use a specific multidisciplinary approach and in rehabilitation centers after hospital discharge.Citation50
Depression
The presence of depression and its treatment increase the risk of fracturesCitation51 and have a negative impact on functional recovery and mortality. Moderate or severe depression upon admission results in poorer recovery at discharge,Citation52 and is predictive of a considerable increase in the institutionalization and mortality rates after 12 months.Citation53,Citation54 Depression in patients with hip fracture has been associated with reductions in plasma dehydroepiandrostenedione and increases in cortisol levels, accelerating progression toward fragility. The cortisol and dehydroepiandrostenedione ratio is higher in individuals with hip fracture than in healthy elderly subjects, and this ratio is a possible mediator between hip fracture and health condition. A study has found post-hip fracture depression to be associated with poorer functional recovery and slower walking speed.Citation55 The screening of depression in these patients could contribute to ensuring better management of the problem and minimizing its negative impact on patient recovery.
Constipation
Constipation is common among patients admitted due to hip fracture and is related to immobilization, loss of intimacy, and use of certain drug substances. In turn, constipation is associated with postoperative complications, a longer mean stay, and higher costs. Nevertheless, the condition is often underdiagnosed.Citation56 Approximately 70% of all patients develop constipation during the first postoperative days, and 62% continue to suffer from the problem up to 1 month after surgery.Citation57 The recommended options to prevent constipation comprise the use of laxatives, an increase in fiber and liquid intake, and the favoring of mobility.Citation58
Malnutrition
Protein–calorie malnutrition increases the risk of falls and fractures. Moreover, the nutritional condition of elderly people with hip fractures tends to worsen during admission, and malnutrition is common among hip fracture patients,Citation59 thereby increasing the risk of complications, mean stay, mortality, and costs. Furthermore, malnutrition is more frequent in elderly individuals with greater comorbidity and functional and cognitive deterioration.Citation60 The detection of malnutrition is important, though the application of rapid detection tools for this purpose is insufficient.Citation61 Nutritional intervention in the postoperative period of these patients does afford clinical benefits in the form of a shorter stay, fewer complications, lesser mortality, and more stable quality of life.Citation62–Citation66 Exhaustive care in the home after hospital discharge, with the inclusion of nutritional measures, significantly improves the nutritional condition of the patients and their functional capacity.Citation67 A recent meta-analysis on perioperative oral nutritional supplementation in elderly patients with hip surgery based on ten studies described a positive effect on serum total protein levels, with a decrease in the number of complications and wound, respiratory and urinary tract infections, though no significant differences in mortality were recorded.Citation68
Swallowing problems can result in denutrition, dehydration, aspiration pneumonia, a longer stay in hospital, and increased costs.Citation69 In one study, 27.7% of the patients who previously had no swallowing problems developed oropharyngeal dysphagia 72 hours after hip fracture surgery – this condition being associated with the presence of prior neurological and/or respiratory illness, postoperative delirium, age, and previous institutionalization.Citation70 The development of dysphagia in the postoperative period is of multifactorial origin, and screening measures should be adopted, particularly in more fragile patients.
Urinary retention and urinary incontinence
In a recent study,Citation71 51.3% of the patients admitted because of hip fracture suffered urinary retention with the need for bladder catheterization – retention in turn being associated with the presence of diabetes, urinary infection, and delirium. Hip fracture likewise has been related to an increased prevalence of urinary incontinence (UI).Citation72 Incontinence after surgery has been associated with the use of drugs and anesthetic agents, appearance of urinary retention and/or infection, constipation, and difficulty in gaining access to bathroom, among other factors. The presence of UI can have a negative impact on functional recovery.Citation73 In one study,Citation74 11% of the patients presented incontinence 72 hours after surgery, and the problem was associated with delirium, urinary infection, cognitive impairment, and depressive symptoms. Furthermore, 12 months after the operation, the patients had poorer function and greater institutionalization and mortality rates than the patients without UI. The probability of developing incontinence during hospitalization has been associated with previous institutionalization, delirium, previous need for medical devices, and walking dependency.Citation75 At 6 months after discharge, the prevalence of incontinence remains high, though after 2 years of follow-up it has been shown that UI, together with personal hygiene and eating, is one of the basic aspects that is most amenable to improvement.Citation76,Citation77 UI should be taken into account by orthogeriatric teams, though the evidence of the efficacy of specific management during admission is not convincing.Citation78
Pressure sores
In a study carried out in several European countries, the prevalence of pressure sores (PSs) in elderly people admitted due to hip fracture was 10% upon admission and 22% at discharge – most of them being of grade I. The factors associated with PSs at discharge were patient age over 70 years, dehydration, moist skin, total Braden score, nutritional status, existence of sensory defects, and presence of diabetes and/or lung disease.Citation79 Other studies have also reported an association with delays in surgery;Citation80 moreover, the presence of such ulcers prolongs hospital stay.Citation81 The use of appropriate clinical pathways in patient care can reduce the incidence of PSs by more than 50%.Citation82 Devices for elevating the heels and the use of pressure-redistributing mattresses have been found to be effective in some studies,Citation83 though other publications with low PS incidence have failed to observe benefits.Citation84 Surgical delay is related to the incidence of PSs, and a meta-analysis mentioned showed a reduction of risk of PSs related to shorter surgical delay (OR 0.48, [95% CI 0.38–0.60; I2=0%]).Citation27
Perioperative care
Renal function
Patients with low glomerular filtration rates present with increased comorbidity, lower hemoglobin (Hb) concentrations upon admission, longer surgical delays, and greater incidence of delirium. At hospital discharge, individuals with higher glomerular filtration rates yield higher motor Functional Independence Measure (FIM) scores. Likewise, low plasma urea levels upon admission have been associated with greater recovery of the motor FIM score and higher total score at discharge.Citation85
Anemia
The management of anemia in geriatric patients with hip fracture is subject to controversy. Upon admission to hospital, ~80% of all fracture patients have Hb values below 11 g/dL. A clinical trialCitation86 randomized patients with hip fracture and anemia to two transfusion thresholds (8 and 10 g/dL, respectively) and no differences were observed in mortality after 30 days or in walking capacity after 60 days. Conversely, Gregersen et alCitation87 randomized patients to two transfusion thresholds in a clinical trial: restrictive (Hb <9.7 g/dL) and liberal (Hb <11.3 g/dL). There were no functional improvement differences, but 30-day and 90-day mortality was higher with the restrictive strategy, hazard ratio =2.4 (95% CI 1.1–5.2; P=0.03) and hazard ratio =2.0 (95% CI 1.1–3.6; P=0.01), respectively. A Cochrane review and meta-analysisCitation88 of 2,722 patients found no differences when two thresholds for red blood cell transfusion were compared: a liberal strategy to maintain a Hb concentration of usually 10 g/dL versus a more restrictive strategy based on symptoms of anemia or a lower Hb concentration, usually 8 g/dL. There was no evidence of a difference between a liberal versus restricted threshold transfusion in mortality at 30 days post-hip fracture surgery or at 60 days postsurgery; neither was there in functional recovery at 60 days. There was low quality evidence of no difference between the transfusion thresholds in postoperative morbidity for the following complications: thromboembolism, stroke, wound infection, respiratory infection (pneumonia), and new diagnosis of congestive heart failure. There was very low-quality evidence of a lower risk of myocardial infarction in the liberal compared with the restrictive transfusion threshold group (risk ratio 0.59, 95% CI 0.36–0.96; three trials; 2,217 participants). Authors concluded that the available evidence does not support the use of liberal red blood cell transfusion thresholds based on a 10 g/dL Hb trigger. Intravenous ironCitation89 has not been found to reduce the transfusion rate, hospital stay, complications, or infections.
Second hip fracture
Many studies have shown that osteoporosis is underdiagnosed and hence undertreated in patients with hip fracture. In this regard, hip fracture represents an opportunity for starting early prevention of new fractures.Citation90 Patients who have suffered hip fracture are at a greater risk of new falls and fractures than the general population. Low scores (≤14 points) on the Norton scale, used to evaluate the risk of PSs, are associated with increased mortality, greater risk of postoperative complications such as urinary infections, and up to threefold higher risk of new falls.Citation91,Citation92 In a population-based 7-year follow-up study of 87,415 patients with a first hip fracture, the incidence of a second hip fracture was 9.2% – the annual risk in patients aged 75 years or older being 4.1%.Citation93 In this study, the presence of obesity, diabetes, arterial hypertension, dyslipidemia, cerebrovascular disease, and/or vision problems was associated with an increased risk of a second fracture, while bisphosphonate therapy was associated with a lesser risk. The most common strategies for avoiding such situations include changes in lifestyle, drug treatment, and prevention of falls.Citation94
Functional recovery
The fundamental aim of orthogeriatric units is to restore the previous independence of the patient.Citation33 Each day of immobilization makes it more difficult to reach this aim due to diminished muscle mass and strength, increased joint stiffness and pain, and loss of confidence – with the consequent fear of falls. A recent meta-analysisCitation25 has evidenced shortened hospital stay and lesser mortality in orthogeriatric units, with no differences in functional recovery. Another meta-analysisCitation95 likewise observed no improvement in the long-term functional outcomes in the orthogeriatric models.
A retrospective cohort study of 1,257 patients with hip fracture recorded a 68% community reincorporation rate after rehabilitation. Likewise, they presented fewer comorbidities, shorter hospital stay, and better functional and cognitive conditions. Use of the motor FIM score made it possible to predict which patients could return home.Citation96
A randomized clinical trialCitation97 found functional gain to be greater in the orthogeriatric care group than among the patients receiving routine trauma care during the follow-up period. At 1 month after discharge, the patients in the orthogeriatric care group presented with a higher Short Physical Performance Battery score; after 4 months this was also accompanied by better cognitive function, greater independence, lesser fear of falls, and better quality of life. In addition, after 12 months, improved scores were observed on the Geriatric Depression Scale. The mean hospital stay was longer in this group, with a larger percentage of patients sent home after hospital discharge.
Early mobilization after the operation is essential since it reduces the incidence of delirium and pneumonia, improves function, and is associated with lesser mortality.Citation98
However, a few studies have examined the relationship between inpatient bed rest and functional outcomes. A prospective cohort study of 532 patients examined the relationship between immobility, function, and mortality in patients with hip fracture. Such patients experienced an average of 5.2 days of immobility. Compared with patients with a longer duration of immobility (ie, at the 90th percentile) in adjusted analyses, patients at the 10th percentile of immobility had a lower 6-month mortality (−5.4%; 95% CI −10.9% to −1.0%) and a better FIM score for locomotion (0.99 points; 95% CI 0.3−1.7 points). The adverse association of immobility was strongest in patients using personal assistance or supervision with locomotion at baseline (difference in 6-month mortality between the 90th and 10th percentile of immobility was −17.1% [P=0.004] for this group and only 1.2% [P=0.38] for patients independent in locomotion at baseline).Citation99
A study on early mobilization investigated the effect of early ambulation (EA) after hip fracture surgery on patient and hospital outcomes. Randomization was either EA (first walk postoperative day 1 or 2) or delayed ambulation (first walk postoperative day 3 or 4). At 1 week postsurgery, patients in the EA group walked further distance than those in the delayed ambulation group (34.70 m [range, r=5–103] versus 29.71 m [r=0–150], P=0.03) and required less assistance to transfer (26.3% versus 50%, P=0.009).Citation100
A subanalysis of a randomized controlled trial, the Trondheim Hip Fracture Trial, compared physical behavior and function during the first postoperative days for hip fracture patients managed with comprehensive geriatric care with those managed with orthopedic care. The comprehensive geriatric care participants had significantly more upright time (mean 57.6 versus 45.1 minute, P=0.016), higher number of upright events (24.1 [SD =22.1] versus 19.0 [SD =16.5], P=0.005), and better Short Physical Performance Battery scores (1.6 [SD =2.0] versus 1.0 [SD =1.6], P=0.002) than the orthopedic care participants.Citation101
Surgical treatment
In patients with subcapital fractures, total arthroplasty versus hemiarthroplasty offers more lasting functional results and better pain control, despite a greater risk of complications (mainly luxation).Citation102 Surgery must take into account the patient’s mental condition, social situation, level of dependency, and quality of bone in deciding the type of operation. Minimally invasive surgical techniques reduce bleeding and transfusion needs versus conventional surgery.Citation103 In a recent meta-analysis, the minimally invasive dynamic hip screw technique in elderly patients with intertrochanteric fractures has been found to be safe and effective, with a more limited blood loss, shorter hospital stay, less pain, and greater functional gain versus the conventional technique.Citation104 However, a later studyCitation105 has failed to record fewer transfusion needs or lower mortality after 1 year when comparing treatment in the form of percutaneous compression plating (PCCP) versus dynamic hip screw. Likewise, there appeared to be no differences in clinical effectiveness when comparing PCCP with the proximal femoral nail anti-rotation technique, though PCCP resulted in lesser blood loss and shorter surgical times.Citation106
General, epidural, or spinal anesthesia in elderly patients with hip fracture exerts no influence upon the incidence of delirium or cognitive impairment, duration of stay, patient destination at discharge, or mortality after 1 year.Citation107
Prognostic factors and mortality
Several studies on orthogeriatric care units have shown a reduction in mortality. These studies have also linked a number of prognostic factors with mortality in elderly patients admitted to hospital with hip fractures. Early identification and specific treatment of these factors could help to reduce hip fracture patients mortality. The results of a meta-analysis showed orthogeriatric collaboration to be associated with a significant decrease in in-hospital mortality and mortality over the long term,Citation25 with a shorter stay in hospital. No improvements were observed in terms of the incidence of delirium, reductions in surgical delay, or functional recovery.
A comparative study has shown that the presence of orthogeriatric unit reduces the 30-day adjusted mortality rate and mean duration of stay.Citation108 The mortality rate and mean stay can be predicted using the Multidimensional Prognostic Index, which contemplates functional, cognitive, nutritional, social, and clinical information and predicts mortality in patients presenting a series of clinical conditions. A study has found high Multidimensional Prognostic Index scores to be associated with longer hospital stays and poorer survival rates.Citation109 A retrospective study analyzed the main comorbidities found in patients admitted due to hip fracture and their influence on mortality. A 12-month post-discharge mortality predictive model, based on comorbidities, included patient age, cognitive impairment, and surgical delay, and was able to explain 26% of the variability in mortality. A second model, based on the complications, included patient age and respiratory complications, and was likewise able to explain 26% of the variability in mortality.Citation110
Another prospective study divided the patients into two age groups (85–89 and >90 years). The older group showed greater mortality. The factors associated with mortality after 6 months were severe disability and postoperative delirium.Citation111 A retrospective study evaluated the activity of an orthogeriatric care unit of geriatric patients diagnosed with hip fracture between 2004 and 2008. Male sex, Barthel score, heart failure, and cognitive impairment were seen to be associated with an increased mortality risk. With regard to function, 63.7%, 77.4%, and 80.1% of the patients had recovered walking capacity at discharge, 1 month, and 6 months after fracture, respectively. The factors associated with poorer functional recovery included cognitive impairment, functional condition, age, cerebrovascular events, Charlson score, and delirium during hospital admission.Citation112
Controversies of the orthogeriatric care model
Different studiesCitation103–Citation115 have confirmed that the orthogeriatric care model reduces mean stay and mortality. An analysisCitation116 divided the patients with hip fracture into two age groups (65–84 versus ≥85 years). The older group showed greater comorbidity and higher prevalence of cognitive impairment, which were not associated with longer surgical delays, though both the length of hospital stay and mortality rate (in-hospital and 30 days and 12 months after discharge) were greater; the percentage of patients entering homes for the elderly after discharge was also higher. The authors concluded that patients aged 85 years or older are high-risk patients and merit specific clinical management. Another retrospective studyCitation117 compared the results corresponding to 6 months before the start of activities of an orthogeriatric team versus the findings 6 months after the start of such activities. The orthogeriatric team activities resulted in shortened stay and increase in the adoption of secondary fracture prevention measures.
A study has analyzed the changes recorded in a department after the introduction of a clinical pathway in hip fractures. The initiative was found to result in a shortened stay and a lesser probability of complications during hospital admission.Citation118 Similar results have been obtained in another studyCitation35 where the introduction of a multidisciplinary management model with preoperative geriatric assessment and daily geriatric clinical care resulted in an increased percentage of patients operated upon within the first 48 hours and a reduction in hospital stay.
However, these data may be interfered with by circumstances that alter routine care, such as weekends. In this regard, a retrospective study of 2,989 consecutive individuals compared patient care on working days versus care provided on weekends. A significant association with mortality after 30 days was observed in the patients admitted on weekends, despite the absence of greater mortality associated with surgery performed on weekends.Citation119
Costs
A study described the compared cost-utility analysis and orthogeriatric care model versus an interconsultation orthogeriatric department. This paper found orthogeriatric care to offer greater cost-effectiveness since the orthogeriatric care model used 23% fewer resources per patient ($14,919 versus $19,363) and avoided 0.226 disability-adjusted life years per patient, adding quality-adjusted life years by lowering the cost of institutionalization per patient, with a reduction of mortality after 1 year.Citation120 A retrospective cohort study in turn compared orthogeriatric care versus routine trauma care, and found the former to result in mean savings of $13,737 per patient, with a decrease in mortality after 12 months.Citation121 Lastly, a randomized, prospective intervention study comparing the care provided in an orthogeriatric unit versus the care provided in a traumatology ward with interconsultation geriatric management found the patients treated in the orthogeriatric unit to have a greater probability of starting rehabilitation in the acute cases ward, with greater recovery of walking capacity, earlier surgery, and shorter hospital stay. All these implied an estimated process cost saving of €1,207–€1,633 per patient, including the avoided stays which is an estimated saving of €3,741 per year.Citation122
Future perspectives and lines of research
It is interesting to mention some recent publications that have evaluated the presence of sarcopenia in patients with hip fracture, in both the acute phase and in the subacute and chronic phases. In a recent study, the prevalence of sarcopenia in patients admitted due to hip fracture was 17.1% (12.4% in males and 18.3% in females).Citation123 In this regard, patients with sarcopenia suffer greater functional loss at discharge. The observed prevalence is low in comparison with the data obtained in other studies.Citation124
Another important point requiring consideration is the difference in predicted function and survival after hip fracture in institutionalized patients. A retrospective cohort of 60,111 patients found that 36.2% of the patients died in the first 180 days after fracture. Of the patients who were not fully dependent before fracture, a total of 53.5% either died or became totally dependent in the first 180 days – the prognosis being poorer in individuals with severe cognitive impairment, subjects over 90 years of age, patients who had not received surgical treatment for the fracture.Citation125
Conclusion
Orthogeriatric units improve the quality standards of care of geriatric patients with hip fracture, such as survival and functional recovery rates, thereby also reducing the length of stay and costs. Some clinical trials and meta-analyses published over the last 5 years support this evidence. Nevertheless, there are still gaps in knowledge regarding specific clinical issues, such as the best approach to pain, choice of certain surgical procedures, Hb threshold for blood transfusion, or measures to reduce the incidence of blood transfusions during hospital admission, and the continuity of care in concrete situations, such as cognitive impairment or institutionalization. Future studies are needed to help answer these questions.
Author contributions
Francisco José Tarazona-Santabalbina and Ángel Belenguer-Varea carried out a selected keyword search and conceived and designed this study. They selected the articles and drafted the manuscript in collaboration Eduardo Rovira and David Cuesta-Peredó. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank Juan María de la Cámara de las Heras, librarian and archivist of Hospital Universitario de la Ribera, for his help in carrying out the necessary literature search for this review.
Disclosure
The authors report no conflicts of interest in this work.
References
- JohnellOKanisJAAn estimate of the worldwide prevalence, mortality and disability associated with hip fractureOsteoporos Int20041589790215490120
- CooperCCampionGMeltonLJHip fractures in the elderly: a world-wide projectionOsteoporos Int199222852891421796
- LauritzenJBSchwarzPLundBChanging incidence and residual lifetime risk of common osteoporosis-related fracturesOsteoporos Int1993331271328481588
- AschkenasyMTRothenhausTCTrauma and falls in the elderlyEmerg Med Clin North Am200624241343216584964
- RocheJJWennRTSahotaOEffect of comorbidities and postoperative complications on mortality after hip fracture in elderly people: prospective observational cohort studyBMJ20053317529137416299013
- MorrisAHZuckermanJDAAOS Council of Health Policy Practice, USAAmerican Academy of Orthopaedic SurgeonsNational Consensus Conference on Improving the Continuum of Care for Patients with Hip FractureJ Bone Joint Surg Am200284-A467067411940633
- BertramMNormanRKempLReview of the long-term disability associated with hip fracturesInj Prev201117636537021486987
- BraithwaiteRSColNFWongJBEstimating hip fracture morbidity, mortality and costsJ Am Geriatr Soc200351336437012588580
- MagazinerJHawkesWHebelJRRecovery from hip fracture in eight areas of functionJ Gerontol A Biol Sci Med Sci2000559M498M50710995047
- KannegaardPNvan der MarkSEikenPExcess mortality in men compared with women following a hip fracture. National analysis of comedications, comorbidity and survivalAge Ageing201039220320920075035
- MorinSLixLMAzimaeeMMortality rates after incident non-traumatic fractures in older men and womenOsteoporos Int20112292439244821161507
- LeibsonCLTostesonANGabrielSEMortality, disability, and nursing home use for persons with and without hip fracture: a population-based studyJ Am Geriatr Soc200250101644165012366617
- DevasMGeriatric OrthopaedicsLondonAcademic Press1977
- SabharwalSWilsonHOrthogeriatrics in the management of frail older patients with a fragility fractureOsteoporos Int201526102387239925986384
- KhasraghiFAChristmasCLeeEJEffectiveness of a multidisciplinary team approach to hip fracture managementJ Surg Orthop Adv2005141273115766439
- VidanMSerraJAMorenoCEfficacy of a comprehensive geriatric intervention in older patients hospitalized for hip fracture: a randomized, controlled trialJ Am Geriatr Soc20055391476148216137275
- FriedmanSMMendelsonDABinghamKWImpact of a comanaged Geriatric Fracture Center on short-term hip fracture outcomesArch Intern Med2009169191712171719822829
- González-MontalvoJIAlarcón AlarcónTOrthogeriatrics in acute patients: to act, but also assess and compare as a way to improveRev Esp Geriatr Gerontol201449310110224656718
- De RuiMVeroneseNManzatoERole of comprehensive geriatric assessment in the management of osteoporotic hip fracture in the elderly: an overviewDisabil Rehabil201335975876522877311
- PillaiAErankiVShenoyRAge related incidence and earl outcomes of hip fractures: a prospective cohort study of 1177 patientsJ Orthop Surg Res20116521261942
- WilsonHHardingKSahotaOBest practice tariff for hip fracture-making ends meet Available from: http://www.bgs.org.ukAccessed January 13, 2016
- Payment by Results Guidance for 2013–2014 Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/214903/Code-of-Conduct-for-Payment-by-Results-in-2013-14.pdfAccessed January 13, 2016
- National Institute for Health and Care ExcellenceQuality Standards for Hip Fracture 2012 Available from: http://www.nice.org.ukAccessed January 13, 2016
- FernandezMAGriffinXLCostaMLManagement of hip fractureBr Med Bull2015115116517226311503
- GrigoryanKVJavedanHRudolphJLOrthogeriatric care models and outcomes in hip fracture patients: a systematic review and meta-analysisJ Orthop Trauma201428e49e5523912859
- Della RoccaGJCristBDHip fracture protocols: what have we changed?Orthop Clin North Am201344216318223544822
- MojaLPiattiAPecoraroVTiming matters in hip fracture surgery: patients operated within 48 hours have better outcomes. A meta-analysis and meta-regression of over 190,000 patientsPLoS One2012710e4617523056256
- VidánMTSánchezEGraciaYCauses and effects of surgical delay in patients with hip fracture: a cohort studyAnn Intern Med2011155422623321844548
- SimunovicNDevereauxPJSpragueSEffect of early surgery after hip fracture on mortality and complications: systematic review and meta-analysisCMAJ2010182151609161620837683
- MarslandDChadwickCProspective study of surgical delay for hip fractures: impact of an orthogeriatrician and increased trauma capacityInt Orthop20103481277128419838708
- NicholasJAPreoperative optimization and risk assessmentClin Geriatr Med201430220721824721361
- HughsonJNewmanJPendletonRCHip fracture management for the hospital-based clinician: a review of the evidence and best practicesHosp Pract20113915261
- WilsonHMulti-disciplinary care of the patient with acute hip fracture: how to optimise the care for the elderly, traumatised patient at and around the time of the fracture to ensure the best short-term outcome as a foundation for the best long-term outcomeBest Pract Res Clin Rheumatol201327671773024836331
- PioliGBaroneAMussiCGIOGThe management of hip fracture in the older population. Joint position statement by Gruppo Italiano Ortogeriatria (GIOG)Aging Clin Exp Res201426554755324566982
- GuptaAThe effectiveness of geriatrician led comprehensive hip fracture collaborative care in a new Acute Hip Unit based in a general hospital setting in the UKJ R Coll Physicians Edinb2014441202624995442
- LundströmMStenvallMOlofssonBSymptom profile of postoperative delirium in patients with and without dementiaJ Geriatr Psychiatry Neurol201225316216923124010
- InouyeSKWestendorpRGJSaczynskiJSDelirium in elderly peopleLancet201491192223992774
- BellelliGMazzolaPMorandiADuration of postoperative delirium is an independent predictor of 6-month mortality in older adults after hip fractureJ Am Geriatr Soc20146271335134024890941
- RoblesMJFormigaFVidánMTDelirium prevention and treatment in elderly hip fractureMed Clínica20141428365369
- MarcantonioERFlackerJMJohn WrightRReducing delirium after hip fracture: a randomized trialJ Am Geriatr Soc200149551652211380742
- DeschodtMBraesTFlamaingJPreventing delirium in older adults with recent hip fracture through multidisciplinary geriatric consultationJ Am Geriatr Soc201260473373922429099
- LundstromMOlofssonBStenvallMPostoperative delirium in old patients with femoral neck fracture: a randomized intervention studyAging Clin Exp Res200719317818617607084
- StenvallMBerggrenMLundströmMA multidisciplinary intervention program improved the outcome after hip fracture for people with dementia – subgroup analyses of a randomized controlled trialArch Gerontol Geriatr2012543e284e28921930310
- SinglerKBiberRWickleinS“N-active”: a new comanaged, orthogeriatric ward: observations and prospectsZ Gerontol Geriatr201144636837422159830
- Colón-EmericCSPostoperative management of hip fractures: interventions associated with improved outcomesBonekey Rep2012124124340216
- SeitzDPAdunuriNGillSSPrevalence of dementia and cognitive impairment among older adults with hip fracturesJ Am Med Dir Assoc201112855656421450227
- AllenJKoziakABuddinghSRehabilitation in patients with dementia following hip fracture: a systematic reviewPhysiother Canada Physiothérapie Canada2012642190201
- Uriz-OtanoFIsidro Uriz-OtanoJMalafarinaVFactors associated with short-term functional recovery in elderly people with a hip fracture. Influence of cognitive impairmentJ Am Med Dir Assoc201516321522025441099
- Tarazona-SantabalbinaFJBelenguer-VareaÁRovira DaudiESeverity of cognitive impairment as a prognostic factor for mortality and functional recovery of geriatric patients with hip fractureGeriatr Gerontol Int201515328929525164866
- MorghenSGentileSRicciERehabilitation of older adults with hip fracture: cognitive function and walking abilitiesJ Am Geriatr Soc20115981497150221797828
- WuQLiuJGallegos-OrozcoJFDepression, fracture risk, and bone loss: a meta-analysis of cohort studiesOsteoporos Int201021101627163520204602
- Dubljanin RaspopovićEMarićNNedeljkovićUDo depressive symptoms on hospital admission impact early functional outcome in elderly patients with hip fracture?Psychogeriatrics201414211812324954835
- GueriniFMorghenSLucchiEDepressive symptoms and one year mortality among elderly patients discharged from a rehabilitation ward after orthopaedic surgery of the lower limbsBehav Neurol201023311712121098965
- MorghenSBellelliGManueleSModerate to severe depressive symptoms and rehabilitation outcome in older adults with hip fractureInt J Geriatr Psychiatry2011261136114321064116
- PhillipsACUptonJDuggalNACarrollDLordJMDepression following hip fracture is associated with increased physical frailty in older adults: the role of the cortisol: dehydroepiandrosterone sulphate ratioBMC Geriatr2013136023773910
- NeighbourCImproving bowel care after surgery for hip fractureNurs Older People20142610162225430842
- TradsMPedersenPUConstipation and defecation pattern the first 30 days after hip fractureInt J Nurs Pract201521559860424758257
- Oral laxative use pre- and post-hip fracture or other emergency orthopedic surgery: a review of the guidelines – PubMed – NCBI [Internet] [cited January 28, 2016 Jan 28]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26180883Accessed May 31, 2016
- DrevetSBioteauCMazièreSPrevalence of protein-energy malnutrition in hospital patients over 75 years of age admitted for hip fractureOrthop Traumatol Surg Res2014100666967424998085
- Koren-HakimTWeissAHershkovitzAThe relationship between nutritional status of hip fracture operated elderly patients and their functioning, comorbidity and outcomeClin Nutr201231691792122521470
- BellJJBauerJDCapraSQuick and easy is not without cost: implications of poorly performing nutrition screening tools in hip fractureJ Am Geriatr Soc201462223724324428255
- EnerothMOlssonU-BThorngrenK-GNutritional supplementation decreases hip fracture-related complicationsClin Orthop Relat Res200645121221716770284
- Botella-CarreteroJIIglesiasBEffects of oral nutritional supplements in normally nourished or mildly undernourished geriatric patients after surgery for hip fracture: a randomized clinical trialJPEN J Parenter Enteral Nutr200832212012818407904
- DuncanDGBeckSJHoodKUsing dietetic assistants to improve the outcome of hip fracture: a randomised controlled trial of nutritional support in an acute trauma wardAge Ageing200635214815316354710
- HoekstraJCGoosenJHMde WolfGSEffectiveness of multidisciplinary nutritional care on nutritional intake, nutritional status and quality of life in patients with hip fractures: a controlled prospective cohort studyClin Nutr201130445546121342737
- PimlottBJJonesCABeaupreLAPrognostic impact of pre-operative albumin on short-term mortality and complications in patients with hip fractureArch Gerontol Geriatr2011531909420684997
- LiuH-YTsengM-YLiH-JComprehensive care improves physical recovery of hip-fractured elderly Taiwanese patients with poor nutritional statusJ Am Med Dir Assoc201415641642224613271
- LiuMYangJYuXThe role of perioperative oral nutritional supplementation in elderly patients after hip surgeryClin Interv Aging20151084985826005339
- AltmanKWYuG-PSchaeferSDConsequence of dysphagia in the hospitalized patient: impact on prognosis and hospital resourcesArch Otolaryngol Head Neck Surg2010136878478920713754
- LoveALCornwellPLWhitehouseSLOropharyngeal dysphagia in an elderly post-operative hip fracture population: a prospective cohort studyAge Ageing201342678278523531439
- AdunskyANenaydenkoOKoren-MoragNPerioperative urinary retention, short-term functional outcome and mortality rates of elderly hip fracture patientsGeriatr Gerontol Int2015151657124418251
- MaggiSMinicuciNLangloisJPrevalence rate of urinary incontinence in community-dwelling elderly individuals: the Veneto studyJ Gerontol A Biol Sci Med Sci2001561M14M1811193226
- LukJKHChiuPKCTamSRelationship between admission albumin levels and rehabilitation outcomes in older patientsArch Gerontol Geriatr2011531848920678814
- SørbyeLWGrueEVHip fracture and urinary incontinence – use of indwelling catheter postsurgeryScand J Caring Sci201327363264222943160
- PalmerMHBaumgartenMLangenbergPRisk factors for hospital-acquired incontinence in elderly female hip fracture patientsJ Gerontol A Biol Sci Med Sci20025710M672M67712242323
- Candel-ParraECórcoles-JiménezMPDel Egido-FernándezMAIndependence in activities of daily living 6 months after surgery in previously independent elderly patients with hip fracture caused by a fallEnfermería Clínica200818630931619080883
- AlarcónTGonzález-MontalvoJIGotorPActivities of daily living after hip fracture: profile and rate of recovery during 2 years of follow-upOsteoporos Int20112251609161320521027
- ParkinsonLChiarelliPByrneJContinence promotion for older hospital patients following surgery for fractured neck of femur: pilot of a randomized controlled trialClin Interv Aging20072470571418225472
- LindholmCSternerERomanelliMHip fracture and pressure ulcers – the Pan-European Pressure Ulcer Study – intrinsic and extrinsic risk factorsInt Wound J20085231532818494637
- Rodriguez-FernandezPAdarraga-CansinoDCarpinteroPEffects of delayed hip fracture surgery on mortality and morbidity in elderly patientsClin Orthop Relat Res2011469113218322121210312
- IrelandAWKellyPJCummingRGTotal hospital stay for hip fracture: measuring the variations due to pre-fracture residence, rehabilitation, complications and comorbiditiesBMC Health Serv Res2015151725609030
- NeumanMDArchanSKarlawishJHThe relationship between short-term mortality and quality of care for hip fracture: a meta-analysis of clinical pathways for hip fractureJ Am Geriatr Soc200957112046205419793159
- DonnellyJWinderJKernohanWGAn RCT to determine the effect of a heel elevation device in pressure ulcer prevention post-hip fractureJ Wound Care2011207314318
- RichSEShardellMHawkesWGPressure-redistributing support surface use and pressure ulcer incidence in elderly hip fracture patientsJ Am Geriatr Soc20115961052105921649630
- AdunskyAMizrahiEHKaplanAElevated blood urea, independent of glomerular filtration rate (GFR), confers increased risk of adverse functional outcome in elderly hip fracture patientsArch Gerontol Geriatr2011532e174e17820875688
- CarsonJLTerrinMLNoveckHLiberal or restrictive transfusion in high-risk patients after hip surgeryN Engl J Med2011365262453246222168590
- GregersenMBorrisLCDamsgaardEMPostoperative blood transfusion strategy in frail, anemic elderly patients with hip fracture: the TRIFE randomized controlled trialActa Orthop201586336337225586270
- BrunskillSJMilletteSLShokoohiARed blood cell transfusion for people undergoing hip fracture surgeryCochrane Database Syst Rev20154CD00969925897628
- YangYLiHLiBEfficacy and safety of iron supplementation for the elderly patients undergoing hip or knee surgery: a meta-analysis of randomized controlled trialsJ Surg Res20111712e201e20721962806
- Colon-EmericCKuchibhatlaMPieperCThe contribution of hip fracture to risk of subsequent fractures: data from two longitudinal studiesOsteoporos Int2003141187988314530910
- HalperinEEngelTShermanSLow admission Norton scale scores are associated with falls long after rehabilitation in the elderly with hip fracturesClin Interv Aging2012743143623109805
- GoldASeverRLermanYAdmission Norton scale scores (ANSS) and postoperative complications following hip fracture surgery in the elderlyArch Gerontol Geriatr201255117317621871678
- ShenS-HHuangK-CTsaiY-HRisk analysis for second hip fracture in patients after hip fracture surgery: a nationwide population-based studyJ Am Med Dir Assoc2014151072573125017390
- LönnroosEKautiainenHKarppiPIncidence of second hip fractures. A population-based studyOsteoporos Int20071891279128517440675
- DeschodtMFlamaingJHaentjensPImpact of geriatric consultation teams on clinical outcome in acute hospitals: a systematic review and meta-analysisBMC Med2013114823433471
- WangCYGrahamJEKarmarkarAMFIM motor scores for classifying community discharge after inpatient rehabilitation for hip fracturePM R20146649349724389348
- PrestmoAHagenGSletvoldOComprehensive geriatric care for patients with hip fractures: a prospective, randomised, controlled trialLancet201538599781623163325662415
- KamelHKIqbalMAMogallapuRTime to ambulation after hip fracture surgery: relation to hospitalization outcomesJ Gerontol A Biol Sci Med Sci200358111042104514630887
- SiuALPenrodJDBoockvarKSEarly ambulation after hip fracture: effects on function and mortalityArch Intern Med2006166776677116606814
- OldmeadowLBEdwardsERKimmelLANo rest for the wounded: early ambulation after hip surgery accelerates recoveryANZ J Surg200676760761116813627
- TaraldsenKSletvoldOThingstadPPhysical behavior and function early after hip fracture surgery in patients receiving comprehensive geriatric care or orthopedic care – a randomized controlled trialJ Gerontol A Biol Sci Med Sci201469333834523902933
- MacaulayWPagnottoMRIorioRDisplaced femoral neck fractures in the elderly: hemiarthroplasty versus total hip arthroplastyJ Am Acad Orthop Surg200614528729316675622
- HoMGarauGWalleyGMinimally invasive dynamic hip screw for fixation of hip fracturesInt Orthop200933255556018478227
- ChengTZhangGZhangXReview: minimally invasive versus conventional dynamic hip screw fixation in elderly patients with intertrochanteric fractures: a systematic review and meta-analysisSurg Innov20111829910521712233
- GaddiDPiarulliGAngeloniAGotfried percutaneous compression plating (PCCP) versus dynamic hip screw (DHS) in hip fractures: blood loss and 1-year mortalityAging Clin Exp Res201426549750324633649
- GuoQShenYZongZPercutaneous compression plate versus proximal femoral nail anti-rotation in treating elderly patients with intertrochanteric fractures: a prospective randomized studyJ Orthop Sci201318697798624085380
- IlangoSPulleRCBellJGeneral versus spinal anaesthesia and postoperative delirium in an orthogeriatric populationAustralas J Ageing2015
- ZeltzerJMitchellRJTosonBOrthogeriatric services associated with lower 30-day mortality for older patients who undergo surgery for hip fractureMed J Aust2014201740941125296064
- AnglemanSBSantoniGPilottoAMPI_AGE Project InvestigatorsMultidimensional prognostic index in association with future mortality and number of hospital days in a population-based sample of older adults: results of the EU funded MPI_AGE ProjectPLoS One2015107e013378926222546
- HendersonCYRyanJPPredicting mortality following hip fracture: an analysis of comorbidities and complicationsIr J Med Sci2015184366767125715773
- MazzolaPBellelliGBrogginiVPostoperative delirium and pre-fracture disability predict 6-month mortality among the oldest old hip fracture patientsAging Clin Exp Res2015271536024880696
- Tarazona-SantabalbinaFJBelenguer-VareaARovira-DaudiEEarly interdisciplinary hospital intervention for elderly patients with hip fractures: functional outcome and mortalityClinics (Sao Paulo)201267654755622760891
- AdunskyALerner-GevaLBlumsteinTImproved survival of hip fracture patients treated within a comprehensive geriatric hip fracture unit, compared with standard of care treatmentJ Am Med Dir Assoc201112643944421450210
- LeungAHLamTPCheungWHAn orthogeriatric collaborative intervention program for fragility fractures: a retrospective cohort studyJ Trauma20117151390139422002614
- BhattacharyyaRAgrawalYElphickHA unique orthogeriatric model: a step forward in improving the quality of care for hip fracture patientsInt J Surg201311101083108624120890
- MoonAGrayADeehanDNeck of femur fractures in patient’s aged more than 85 years-are they a unique subset?Geriatr Orthop Surg Rehabil20112412312723569681
- GregersenMMørchMMHougaardKGeriatric intervention in elderly patients with hip fracture in an orthopedic wardJ Inj Violence Res201242455121502786
- SuhmNKaelinRStuderPOrthogeriatric care pathway: a prospective survey of impact on length of stay, mortality and institutionalisationArch Orthop Trauma Surg201413491261126925060921
- ThomasCJSmithRPUzoigweCEThe weekend effect: short-term mortality following admission with a hip fractureBone Joint J201496-B337337824589794
- GinsbergGAdunskyARasoolyIA cost-utility analysis of a comprehensive orthogeriatric care for hip fracture patients, compared with standard of care treatmentHip Int201323657057523934901
- Della RoccaGJMoylanKCCristBDComanagement of geriatric patients with hip fractures: a retrospective, controlled, cohort studyGeriatr Orthop Surg Rehabil20134101523936734
- González MontalvoJIGotor PérezPMartín VegaAThe acute orthogeriatric unit. Assessment of its effect on the clinical course of patients with hip fractures and an estimate of its financial impactRev Esp Geriatr Gerontol201146419319921507529
- González-MontalvoJIAlarcónTGotorPPrevalence of sarcopenia in acute hip fracture patients and its influence on short-term clinical outcomeGeriatr Gerontol Int Epub201593
- HoAWLeeMMChanEWPrevalence of pre-sarcopenia and sarcopenia in Hong Kong Chinese geriatric patients with hip fracture and its correlation with different factorsHong Kong Med J2016221232926680156
- NeumanMDSilberJHMagazinerJSSurvival and functional outcomes after hip fracture among nursing home residentsJAMA Intern Med201417481273128025055155